Download as docx, pdf, or txt
You might also like
- Lab09 Therapy4 IronDeficiencyDocument5 pagesLab09 Therapy4 IronDeficiencyHayna Rose100% (1)
- HELLP Concept Map RevisedDocument1 pageHELLP Concept Map RevisedwandaNo ratings yet
- Hypokalemia 180813073624Document26 pagesHypokalemia 180813073624korotkofNo ratings yet
- AutoPilot Using Telegram - Over $200 DailyDocument6 pagesAutoPilot Using Telegram - Over $200 DailyRobert BillingtonNo ratings yet
- Designer MilkDocument30 pagesDesigner MilkParashuram Shanigaram67% (6)
- Dr. S. Ismat BukhariDocument36 pagesDr. S. Ismat Bukharishravani100% (1)
- G6PD Deficiency Group 6Document36 pagesG6PD Deficiency Group 6Christian Darwin Llanes100% (2)
- G6PD DeficiencyDocument16 pagesG6PD DeficiencyRona SalandoNo ratings yet
- G 6 PDDocument45 pagesG 6 PDPat TuazonNo ratings yet
- Glucose-6-Phosphate Dehydrogenase Deficiency - Overview: Symptom Treatment Prevention All InformationDocument2 pagesGlucose-6-Phosphate Dehydrogenase Deficiency - Overview: Symptom Treatment Prevention All InformationJinky TenezaNo ratings yet
- Hypopituitarism - ThomasDocument40 pagesHypopituitarism - Thomasguidance100% (1)
- Case Study 2Document4 pagesCase Study 2api-2451636590% (1)
- g6pd BrochureDocument2 pagesg6pd BrochureMaha GaberNo ratings yet
- Antiadrenergic DrugsDocument19 pagesAntiadrenergic DrugsshivanshpandeNo ratings yet
- Diuretics TabulationDocument3 pagesDiuretics TabulationAna Rika Javier HarderNo ratings yet
- Classification of Sympatholytic DrugsDocument4 pagesClassification of Sympatholytic DrugsHlaSoe WinNo ratings yet
- EndometriosisDocument6 pagesEndometriosissalamredNo ratings yet
- DIC Case StudyDocument7 pagesDIC Case StudyRobertNo ratings yet
- Diabetes MellitusDocument15 pagesDiabetes Mellitusfayeniwa100% (1)
- Liver Pathophysiology and Schematic Diagram BGFJNDocument1 pageLiver Pathophysiology and Schematic Diagram BGFJNKate Mylhen Espenido EnerlanNo ratings yet
- Anemia in Kidney DiseaseDocument6 pagesAnemia in Kidney DiseaseBazz DanteNo ratings yet
- Nursing Care Plan (NCP) : Patient & Family Centered (In Priority Order)Document1 pageNursing Care Plan (NCP) : Patient & Family Centered (In Priority Order)WorodNo ratings yet
- Pathophysiology of Heart FailureDocument2 pagesPathophysiology of Heart FailureJaysellePuguonTabijeNo ratings yet
- Addison Disease, Penyakit AddisonDocument11 pagesAddison Disease, Penyakit AddisonKertiasihwayanNo ratings yet
- Patients With Hypertensive Nephropathy and Chronic Kidney Disease Might Not Benefit From Strict Blood Pressure Control PDFDocument10 pagesPatients With Hypertensive Nephropathy and Chronic Kidney Disease Might Not Benefit From Strict Blood Pressure Control PDFSayf QisthiNo ratings yet
- HyperlipidemiaDocument17 pagesHyperlipidemiabent alfay7a2No ratings yet
- CyclosporineDocument24 pagesCyclosporinesanchit_J14No ratings yet
- Management of Upper GI BleedingDocument55 pagesManagement of Upper GI BleedingNatnaelNo ratings yet
- Warfarin Mechanism of ActionDocument7 pagesWarfarin Mechanism of ActionIna GrigorasNo ratings yet
- Diabetes Mellitus Type 2Document16 pagesDiabetes Mellitus Type 2MTs MIFDANo ratings yet
- Antihyperlipidemic Drugs: Key Terms Chapter ObjectivesDocument9 pagesAntihyperlipidemic Drugs: Key Terms Chapter ObjectivesSasa AbassNo ratings yet
- AnemiaDocument6 pagesAnemiaGladz DomingoNo ratings yet
- This Study Resource Was Shared Via: HypoparathyroidismDocument1 pageThis Study Resource Was Shared Via: HypoparathyroidismDeo FactuarNo ratings yet
- Hyperglycemia Crisis: Dr. Netty NurnaningtyasDocument34 pagesHyperglycemia Crisis: Dr. Netty Nurnaningtyasnetty nurnaningtyas100% (1)
- Glomerular FiltrationDocument3 pagesGlomerular FiltrationyolandadwiooNo ratings yet
- Learning Objectives:: Pathophysiology & Therapeutics, I (MSPR 521) Lecture No. 14Document9 pagesLearning Objectives:: Pathophysiology & Therapeutics, I (MSPR 521) Lecture No. 14adzhangNo ratings yet
- Pharmacology of Antidiabetic Drugs For Second Year Medicine StudentsDocument54 pagesPharmacology of Antidiabetic Drugs For Second Year Medicine StudentsAmanuel MaruNo ratings yet
- General Prescribing Guidelines For Geriatric PatientsDocument41 pagesGeneral Prescribing Guidelines For Geriatric PatientsBharath Gowda100% (1)
- Compilation Drugstudy, NCP Cva (1) - BadetDocument14 pagesCompilation Drugstudy, NCP Cva (1) - BadetLizette Villanueva-UntalanNo ratings yet
- Disease Spotlight: Diabetes Mellitus: Insulin Insulin Is A Drug That Is Used To ControlDocument7 pagesDisease Spotlight: Diabetes Mellitus: Insulin Insulin Is A Drug That Is Used To ControlMIR SARTAJNo ratings yet
- Case Study HyperkalemiaDocument10 pagesCase Study HyperkalemiaJamaica Cerrero100% (1)
- HyperphosphatemiaDocument18 pagesHyperphosphatemiaS.R.Cogo100% (1)
- Case Study Anemia-1Document6 pagesCase Study Anemia-1Melsya H UtamiNo ratings yet
- Clinical Pharmacy Lab - Quiz Part 2Document4 pagesClinical Pharmacy Lab - Quiz Part 2Aassh DcmbrNo ratings yet
- Case PresentationDocument6 pagesCase PresentationYrrem UbaganNo ratings yet
- Mechanism of HypertensionDocument4 pagesMechanism of HypertensionAlya Putri KhairaniNo ratings yet
- HypokalemiaDocument7 pagesHypokalemiaNader SmadiNo ratings yet
- Case Study of AnemiaDocument3 pagesCase Study of AnemiaAmina Tariq100% (1)
- ThalassemiaDocument1 pageThalassemiaJobelle Fernandez-SantosNo ratings yet
- Predisposing Conditions, Management and Prevention of Chronic Kidney DiseaseDocument52 pagesPredisposing Conditions, Management and Prevention of Chronic Kidney DiseaseSaad MotawéaNo ratings yet
- Cushing's SyndromeDocument5 pagesCushing's SyndromesummerduskNo ratings yet
- NCP GeDocument14 pagesNCP GeSuluhTriUtomoNo ratings yet
- SchizophreniaDocument39 pagesSchizophreniaChikezie OnwukweNo ratings yet
- Medication Administration Knowledge AssessmentDocument4 pagesMedication Administration Knowledge AssessmentkateNo ratings yet
- ACE InhibitorsDocument2 pagesACE InhibitorsJosephine Irena100% (1)
- Acute GlomerulonephritisDocument12 pagesAcute Glomerulonephritiskuchaibaru90No ratings yet
- Idiopathic Thrombocytopenic Purpura: Overview With Report of A CaseDocument4 pagesIdiopathic Thrombocytopenic Purpura: Overview With Report of A CaseHernan GonzalezNo ratings yet
- Radio PharmaceuticalsDocument48 pagesRadio PharmaceuticalsKris Joy EbonNo ratings yet
- Diabetes Type 2 HassanDocument26 pagesDiabetes Type 2 Hassanyash_acharya007100% (1)
- Case No. 6: Glucose 6 Phosphate Deficiency: Mham - First YearDocument52 pagesCase No. 6: Glucose 6 Phosphate Deficiency: Mham - First YearReham QueNo ratings yet
- Glucose 6 Phosphate Dehydrogenase DeficiencyDocument29 pagesGlucose 6 Phosphate Dehydrogenase Deficiencypurplelavender12No ratings yet
- G6PD Deficiency, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandG6PD Deficiency, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 3.5 out of 5 stars3.5/5 (5)
- EntheogenDocument1 pageEntheogenReham QueNo ratings yet
- BREASTDocument11 pagesBREASTReham QueNo ratings yet
- Percussion Borders of Heart (PD)Document1 pagePercussion Borders of Heart (PD)Reham QueNo ratings yet
- CardiacDocument1 pageCardiacReham QueNo ratings yet
- The HipsDocument2 pagesThe HipsReham QueNo ratings yet
- Learning Objectives Male Reproductive System: 1. Identify Corpora AmylaceaDocument16 pagesLearning Objectives Male Reproductive System: 1. Identify Corpora AmylaceaReham QueNo ratings yet
- Cystic and Florid Squamous Metaplasia in Pleomorphic Adenoma of Palate - A Diagnostic DilemmaDocument3 pagesCystic and Florid Squamous Metaplasia in Pleomorphic Adenoma of Palate - A Diagnostic DilemmaReham QueNo ratings yet
- Nose and Paranasal SinusesDocument35 pagesNose and Paranasal SinusesReham QueNo ratings yet
- Table 2.1 Cervical Vertebrae: LargeDocument14 pagesTable 2.1 Cervical Vertebrae: LargeReham QueNo ratings yet
- Meaning and Nature of ResearchDocument11 pagesMeaning and Nature of ResearchReham Que100% (1)
- PhenylketonuriaDocument7 pagesPhenylketonuriaReham QueNo ratings yet
- The Research ProblemDocument10 pagesThe Research ProblemReham QueNo ratings yet
- The Mechanism of Cholesterol Gallstones Formation and Strategy of Their Nonsurgical TherapyDocument9 pagesThe Mechanism of Cholesterol Gallstones Formation and Strategy of Their Nonsurgical TherapyReham QueNo ratings yet
- Descriptive Statistics: Lesson 4Document24 pagesDescriptive Statistics: Lesson 4Reham QueNo ratings yet
- JTD Cus 2020 015 2Document9 pagesJTD Cus 2020 015 2Reham QueNo ratings yet
- Thalamus Group 8Document16 pagesThalamus Group 8Reham QueNo ratings yet
- Zoology Comparative Anatomy Chordate CharacteristicsDocument2 pagesZoology Comparative Anatomy Chordate CharacteristicsReham QueNo ratings yet
- Biochemistry DMDocument1 pageBiochemistry DMReham QueNo ratings yet
- Guidelines For A Healthy Vegetarian DietDocument47 pagesGuidelines For A Healthy Vegetarian DietReham QueNo ratings yet
- Swu-Mham College of Medicine Department of Anatomy Section of Neuroanatomy WorksheetsDocument4 pagesSwu-Mham College of Medicine Department of Anatomy Section of Neuroanatomy WorksheetsReham QueNo ratings yet
- Cooperation Under The Security DilemmaDocument49 pagesCooperation Under The Security Dilemmaabzal kojaixanNo ratings yet
- NCM - 103Document5 pagesNCM - 103Delma SimbahanNo ratings yet
- Spear 4 Module 3Document4 pagesSpear 4 Module 3Cherry Mae AlvaricoNo ratings yet
- Mels Subtype DescriptionsDocument11 pagesMels Subtype DescriptionsclaraNo ratings yet
- Cse320 MCQDocument12 pagesCse320 MCQAnsh Gulati ji100% (1)
- March of The Metro Gnome Lesson PlanDocument2 pagesMarch of The Metro Gnome Lesson Planapi-607297153No ratings yet
- Bharat Heavy Electricals LimitedDocument4 pagesBharat Heavy Electricals LimitedkmbkrisNo ratings yet
- RTS Unit 1 NotesDocument24 pagesRTS Unit 1 NotesSAROJ RAJANo ratings yet
- Reading 23 NovDocument5 pagesReading 23 NovAdhwa QurrotuainiNo ratings yet
- Sealwell-Pump Mechanical SealsDocument8 pagesSealwell-Pump Mechanical SealsVaibhav JainNo ratings yet
- Clinical Laboratory of San Bernardino, IncDocument40 pagesClinical Laboratory of San Bernardino, Inckharberson1613No ratings yet
- Physica Medica: Slobodan Devic, Nada Tomic, David LewisDocument16 pagesPhysica Medica: Slobodan Devic, Nada Tomic, David LewisFrederico GomesNo ratings yet
- Joint Summary SheetDocument1 pageJoint Summary Sheetchandana kumarNo ratings yet
- Rizals First Published Essay El Amor PatDocument23 pagesRizals First Published Essay El Amor PatNelly MesiasNo ratings yet
- LIC Exp Date: AetnaDocument66 pagesLIC Exp Date: AetnaTrudyNo ratings yet
- Darwin's Natural SelectionDocument2 pagesDarwin's Natural Selectionsofia alamiaNo ratings yet
- Current Affairs Capsule For SBI/IBPS/RRB PO Mains Exam 2021 - Part 2Document253 pagesCurrent Affairs Capsule For SBI/IBPS/RRB PO Mains Exam 2021 - Part 2King SammyNo ratings yet
- Mikala Conway - Meal PlanDocument3 pagesMikala Conway - Meal Planmikala conwayNo ratings yet
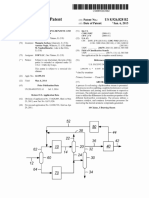
- United States Patent: Serban Et AlDocument9 pagesUnited States Patent: Serban Et AlMutia Herlisa14No ratings yet
- TDC Case FinalDocument3 pagesTDC Case Finalbjefferson21No ratings yet
- FIP Corrosion Protection of Prestressing SteelsDocument79 pagesFIP Corrosion Protection of Prestressing SteelsRizwanNo ratings yet
- Tech Report - Docx.hDocument8 pagesTech Report - Docx.hHuzaif samiNo ratings yet
- About EthiopianDocument7 pagesAbout EthiopianTiny GechNo ratings yet
- Hank Kolb 3Document3 pagesHank Kolb 3gr8_amaraNo ratings yet
- Summer Farm: By: Norman Maccaig Group: Camila Luna and Estrella LinDocument8 pagesSummer Farm: By: Norman Maccaig Group: Camila Luna and Estrella LinJamieDuncanNo ratings yet
- Insulation Resistance (IR) Values - IndexDocument8 pagesInsulation Resistance (IR) Values - IndexAbdullah Al AsikNo ratings yet
- Analog Communication Model ExamDocument20 pagesAnalog Communication Model ExamwalternampimadomNo ratings yet
- 001 GEYSERSD23Final PDFDocument100 pages001 GEYSERSD23Final PDFVasu ThakurNo ratings yet