
Jips 17 48
Jips 17 48
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- Transmigrating Into The Heartthrob's Cannon Fodder - This Concubine Is in ShanyangDocument667 pagesTransmigrating Into The Heartthrob's Cannon Fodder - This Concubine Is in ShanyangLia KaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Equine Internal Medicine 4th EdDocument1,564 pagesEquine Internal Medicine 4th EdJacky Sieras100% (1)
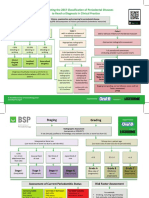
- BSP FlowchartDocument2 pagesBSP FlowchartShahrukh ali khan100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Evaluationand Comparisonofthe Effectof Different Border Molding Materialson 0 AComplete Denture Retention Aniinvivoi StudyDocument7 pagesEvaluationand Comparisonofthe Effectof Different Border Molding Materialson 0 AComplete Denture Retention Aniinvivoi StudyShahrukh ali khanNo ratings yet
- Comparison of Complete Denture Fabricated by Two Different Border Molding Materials, in Terms of Patients' SatisfactionDocument4 pagesComparison of Complete Denture Fabricated by Two Different Border Molding Materials, in Terms of Patients' SatisfactionShahrukh ali khanNo ratings yet
- Complete Denture IntroductionDocument3 pagesComplete Denture IntroductionShahrukh ali khanNo ratings yet
- Staging and GradingDocument4 pagesStaging and GradingShahrukh ali khanNo ratings yet
- Diagnosis and Treatment Planning Part 1Document12 pagesDiagnosis and Treatment Planning Part 1Shahrukh ali khanNo ratings yet
- Effects of Ageing On Edentulous Mouth: BoneDocument6 pagesEffects of Ageing On Edentulous Mouth: BoneShahrukh ali khanNo ratings yet
- Dental Bleaching: Presenter: DR Shahrukh Ali Khan Resident R1 Prosthodontics Aga Khan University, HospitalDocument47 pagesDental Bleaching: Presenter: DR Shahrukh Ali Khan Resident R1 Prosthodontics Aga Khan University, HospitalShahrukh ali khanNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleShahrukh ali khanNo ratings yet
- Clinics in SurgeryDocument5 pagesClinics in SurgeryShahrukh ali khanNo ratings yet
- Common Mistakes in Clinical ResearchDocument6 pagesCommon Mistakes in Clinical ResearchShahrukh ali khanNo ratings yet
- FDS Amp 2020Document140 pagesFDS Amp 2020Shahrukh ali khan100% (1)
- Evaluation of Signs, Symptoms, and Occlusal Factors Among Patients With Temporomandibular Disorders According To Helkimo IndexDocument8 pagesEvaluation of Signs, Symptoms, and Occlusal Factors Among Patients With Temporomandibular Disorders According To Helkimo IndexShahrukh ali khanNo ratings yet
- Bloodborne Pathogens Learner Course Guide: Florida Department of HealthDocument30 pagesBloodborne Pathogens Learner Course Guide: Florida Department of HealthShahrukh ali khanNo ratings yet
- Infection Control in DentistryDocument69 pagesInfection Control in DentistryShahrukh ali khanNo ratings yet
- Necrosis and Types of NecrosisDocument2 pagesNecrosis and Types of NecrosisHisham NesemNo ratings yet
- Hieronymus Revised Rate BookDocument323 pagesHieronymus Revised Rate BookPetrut Valentin100% (2)
- Immunity EPIDocument37 pagesImmunity EPIluttomiayvonneNo ratings yet
- Criterios de Clsificacion de Espondilitis AnquilosanteDocument16 pagesCriterios de Clsificacion de Espondilitis AnquilosanteWilkerson PerezNo ratings yet
- VATA DOSHA Edit PDFDocument3 pagesVATA DOSHA Edit PDFAashray KothaNo ratings yet
- Hagan and Brunerx27s Infectious Diseases of DomestDocument2 pagesHagan and Brunerx27s Infectious Diseases of DomestNopparach ManadeeNo ratings yet
- Multiple Disability Original HandoutDocument42 pagesMultiple Disability Original HandoutHabtamu DebasuNo ratings yet
- The Onset of Acute Type A Aortic Dissection Following Recovery of Type B Intramural Haematoma-A Case ReportDocument4 pagesThe Onset of Acute Type A Aortic Dissection Following Recovery of Type B Intramural Haematoma-A Case ReportNguyễn Thời Hải NguyênNo ratings yet
- Preoperative Preparation and Postoperative CareDocument103 pagesPreoperative Preparation and Postoperative Carechowhan04No ratings yet
- Dwnload Full Research Methods For Social Work 8th Edition Rubin Test Bank PDFDocument35 pagesDwnload Full Research Methods For Social Work 8th Edition Rubin Test Bank PDFmatte.caudalebvf100% (12)
- RDS DR Idham-Dr RismaDocument38 pagesRDS DR Idham-Dr RismaReynaldo Rahima PutraNo ratings yet
- Drug Study-Nifedipine-BALLON, Karlo C.Document2 pagesDrug Study-Nifedipine-BALLON, Karlo C.Melinda Cariño Ballon100% (1)
- Sabino Rebagay Memorial High SchoolDocument6 pagesSabino Rebagay Memorial High SchoolRina RomanoNo ratings yet
- 2010 Nurse Protocol ManualDocument749 pages2010 Nurse Protocol Manualjeenath justin doss100% (2)
- Malignant Pleural Effusion1Document56 pagesMalignant Pleural Effusion1getnusNo ratings yet
- Dr. Jay Davidson: Let'S "Talk" WithDocument32 pagesDr. Jay Davidson: Let'S "Talk" WithDorian GrayNo ratings yet
- THEORIES of CRIME CAUSATION NOTESDocument12 pagesTHEORIES of CRIME CAUSATION NOTESLombroso's follower100% (1)
- HEALTH TALK of EncopresisDocument15 pagesHEALTH TALK of EncopresisAmit RanjanNo ratings yet
- Hospital Waste ManagementDocument40 pagesHospital Waste Managementamir khanNo ratings yet
- Pharma Module 4Document4 pagesPharma Module 4Chelsy Sky SacanNo ratings yet
- EuphorbiaceaeDocument14 pagesEuphorbiaceaeHaritha V HNo ratings yet
- Jeyakumar Dhileeban Rrroll 41Document34 pagesJeyakumar Dhileeban Rrroll 41Rupesh TamizhaNo ratings yet
- Eva Bolton Haematuria Presentation WebDocument52 pagesEva Bolton Haematuria Presentation WebereczkieNo ratings yet
- LV Systolic FunctionDocument36 pagesLV Systolic Functionsruthimeena6891No ratings yet
- Healing With Light and Color GuideDocument31 pagesHealing With Light and Color GuidemariyastojNo ratings yet
- Lesson Plan: Pre-Reading BeginnerDocument15 pagesLesson Plan: Pre-Reading BeginnerMazidah Ida IsmailNo ratings yet
- Shaw 2004Document7 pagesShaw 2004Mouloudi NajouaNo ratings yet
- MedicalCheckUp - Physical Examination PDFDocument3 pagesMedicalCheckUp - Physical Examination PDFCielo Baez ArceNo ratings yet



















































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- Transmigrating Into The Heartthrob's Cannon Fodder - This Concubine Is in ShanyangDocument667 pagesTransmigrating Into The Heartthrob's Cannon Fodder - This Concubine Is in ShanyangLia KaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Equine Internal Medicine 4th EdDocument1,564 pagesEquine Internal Medicine 4th EdJacky Sieras100% (1)
- BSP FlowchartDocument2 pagesBSP FlowchartShahrukh ali khan100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Evaluationand Comparisonofthe Effectof Different Border Molding Materialson 0 AComplete Denture Retention Aniinvivoi StudyDocument7 pagesEvaluationand Comparisonofthe Effectof Different Border Molding Materialson 0 AComplete Denture Retention Aniinvivoi StudyShahrukh ali khanNo ratings yet
- Comparison of Complete Denture Fabricated by Two Different Border Molding Materials, in Terms of Patients' SatisfactionDocument4 pagesComparison of Complete Denture Fabricated by Two Different Border Molding Materials, in Terms of Patients' SatisfactionShahrukh ali khanNo ratings yet
- Complete Denture IntroductionDocument3 pagesComplete Denture IntroductionShahrukh ali khanNo ratings yet
- Staging and GradingDocument4 pagesStaging and GradingShahrukh ali khanNo ratings yet
- Diagnosis and Treatment Planning Part 1Document12 pagesDiagnosis and Treatment Planning Part 1Shahrukh ali khanNo ratings yet
- Effects of Ageing On Edentulous Mouth: BoneDocument6 pagesEffects of Ageing On Edentulous Mouth: BoneShahrukh ali khanNo ratings yet
- Dental Bleaching: Presenter: DR Shahrukh Ali Khan Resident R1 Prosthodontics Aga Khan University, HospitalDocument47 pagesDental Bleaching: Presenter: DR Shahrukh Ali Khan Resident R1 Prosthodontics Aga Khan University, HospitalShahrukh ali khanNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleShahrukh ali khanNo ratings yet
- Clinics in SurgeryDocument5 pagesClinics in SurgeryShahrukh ali khanNo ratings yet
- Common Mistakes in Clinical ResearchDocument6 pagesCommon Mistakes in Clinical ResearchShahrukh ali khanNo ratings yet
- FDS Amp 2020Document140 pagesFDS Amp 2020Shahrukh ali khan100% (1)
- Evaluation of Signs, Symptoms, and Occlusal Factors Among Patients With Temporomandibular Disorders According To Helkimo IndexDocument8 pagesEvaluation of Signs, Symptoms, and Occlusal Factors Among Patients With Temporomandibular Disorders According To Helkimo IndexShahrukh ali khanNo ratings yet
- Bloodborne Pathogens Learner Course Guide: Florida Department of HealthDocument30 pagesBloodborne Pathogens Learner Course Guide: Florida Department of HealthShahrukh ali khanNo ratings yet
- Infection Control in DentistryDocument69 pagesInfection Control in DentistryShahrukh ali khanNo ratings yet
- Necrosis and Types of NecrosisDocument2 pagesNecrosis and Types of NecrosisHisham NesemNo ratings yet
- Hieronymus Revised Rate BookDocument323 pagesHieronymus Revised Rate BookPetrut Valentin100% (2)
- Immunity EPIDocument37 pagesImmunity EPIluttomiayvonneNo ratings yet
- Criterios de Clsificacion de Espondilitis AnquilosanteDocument16 pagesCriterios de Clsificacion de Espondilitis AnquilosanteWilkerson PerezNo ratings yet
- VATA DOSHA Edit PDFDocument3 pagesVATA DOSHA Edit PDFAashray KothaNo ratings yet
- Hagan and Brunerx27s Infectious Diseases of DomestDocument2 pagesHagan and Brunerx27s Infectious Diseases of DomestNopparach ManadeeNo ratings yet
- Multiple Disability Original HandoutDocument42 pagesMultiple Disability Original HandoutHabtamu DebasuNo ratings yet
- The Onset of Acute Type A Aortic Dissection Following Recovery of Type B Intramural Haematoma-A Case ReportDocument4 pagesThe Onset of Acute Type A Aortic Dissection Following Recovery of Type B Intramural Haematoma-A Case ReportNguyễn Thời Hải NguyênNo ratings yet
- Preoperative Preparation and Postoperative CareDocument103 pagesPreoperative Preparation and Postoperative Carechowhan04No ratings yet
- Dwnload Full Research Methods For Social Work 8th Edition Rubin Test Bank PDFDocument35 pagesDwnload Full Research Methods For Social Work 8th Edition Rubin Test Bank PDFmatte.caudalebvf100% (12)
- RDS DR Idham-Dr RismaDocument38 pagesRDS DR Idham-Dr RismaReynaldo Rahima PutraNo ratings yet
- Drug Study-Nifedipine-BALLON, Karlo C.Document2 pagesDrug Study-Nifedipine-BALLON, Karlo C.Melinda Cariño Ballon100% (1)
- Sabino Rebagay Memorial High SchoolDocument6 pagesSabino Rebagay Memorial High SchoolRina RomanoNo ratings yet
- 2010 Nurse Protocol ManualDocument749 pages2010 Nurse Protocol Manualjeenath justin doss100% (2)
- Malignant Pleural Effusion1Document56 pagesMalignant Pleural Effusion1getnusNo ratings yet
- Dr. Jay Davidson: Let'S "Talk" WithDocument32 pagesDr. Jay Davidson: Let'S "Talk" WithDorian GrayNo ratings yet
- THEORIES of CRIME CAUSATION NOTESDocument12 pagesTHEORIES of CRIME CAUSATION NOTESLombroso's follower100% (1)
- HEALTH TALK of EncopresisDocument15 pagesHEALTH TALK of EncopresisAmit RanjanNo ratings yet
- Hospital Waste ManagementDocument40 pagesHospital Waste Managementamir khanNo ratings yet
- Pharma Module 4Document4 pagesPharma Module 4Chelsy Sky SacanNo ratings yet
- EuphorbiaceaeDocument14 pagesEuphorbiaceaeHaritha V HNo ratings yet
- Jeyakumar Dhileeban Rrroll 41Document34 pagesJeyakumar Dhileeban Rrroll 41Rupesh TamizhaNo ratings yet
- Eva Bolton Haematuria Presentation WebDocument52 pagesEva Bolton Haematuria Presentation WebereczkieNo ratings yet
- LV Systolic FunctionDocument36 pagesLV Systolic Functionsruthimeena6891No ratings yet
- Healing With Light and Color GuideDocument31 pagesHealing With Light and Color GuidemariyastojNo ratings yet
- Lesson Plan: Pre-Reading BeginnerDocument15 pagesLesson Plan: Pre-Reading BeginnerMazidah Ida IsmailNo ratings yet
- Shaw 2004Document7 pagesShaw 2004Mouloudi NajouaNo ratings yet
- MedicalCheckUp - Physical Examination PDFDocument3 pagesMedicalCheckUp - Physical Examination PDFCielo Baez ArceNo ratings yet