Download as pdf or txt
You might also like
- CP TumorsDocument21 pagesCP TumorsDr. T. Balasubramanian100% (4)
- DR Clark Purity Kidney Cleanse DirectionsDocument4 pagesDR Clark Purity Kidney Cleanse DirectionsrolickaNo ratings yet
- Birthing Facility IPCR RM Ver 1Document4 pagesBirthing Facility IPCR RM Ver 1RvBombeta50% (2)
- Presbycusis: J. R. Kearns, MDDocument5 pagesPresbycusis: J. R. Kearns, MDnick_mdNo ratings yet
- DD PresbikusisDocument3 pagesDD PresbikusisJ KrystalNo ratings yet
- Presbycusis: Dr. George Backleh Dept. of Otolaryngology/ Head and Neck Surgery Hadassah University Hospital JerusalemDocument16 pagesPresbycusis: Dr. George Backleh Dept. of Otolaryngology/ Head and Neck Surgery Hadassah University Hospital Jerusalemrezky_oktarianti_syahputriNo ratings yet
- Sensorineural Hearing LossDocument19 pagesSensorineural Hearing LossBenitaNo ratings yet
- Kja 17 45 PDFDocument5 pagesKja 17 45 PDFAgnice SimanjuntakNo ratings yet
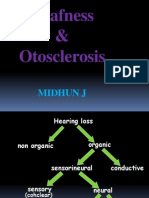
- Deafness & Otosclerosis: Midhun JDocument44 pagesDeafness & Otosclerosis: Midhun JRohit R PillaiNo ratings yet
- Background: MeningitisDocument7 pagesBackground: MeningitisranmiNo ratings yet
- Presbycusis: Sang Hoon Kim, Seung Geun YeoDocument6 pagesPresbycusis: Sang Hoon Kim, Seung Geun YeoLuluk AisyahNo ratings yet
- What Is Presbycusis?: OtosclerosisDocument8 pagesWhat Is Presbycusis?: OtosclerosisIndraRukmanaHamimPartIINo ratings yet
- PresbyacusisDocument15 pagesPresbyacusisP MilanNo ratings yet
- O To SclerosisDocument23 pagesO To SclerosisJennifer Dixon100% (1)
- OtosclerosisDocument36 pagesOtosclerosisShamsheer ShaikNo ratings yet
- Prevention and Rehabilitation of Old Age DeafnessDocument8 pagesPrevention and Rehabilitation of Old Age DeafnessXilena HerreraNo ratings yet
- Suddensnhl 160220190525Document80 pagesSuddensnhl 160220190525mariahovhannisyanNo ratings yet
- 12 P69344 Pho Kapitel 4 S47 52 PDFDocument6 pages12 P69344 Pho Kapitel 4 S47 52 PDFprofesor conanNo ratings yet
- OtosclerosisDocument9 pagesOtosclerosisHelgaNo ratings yet
- O To SclerosisDocument9 pagesO To SclerosisHelgaNo ratings yet
- Nelson Chen 2004 The Relationship of Tinnitus Hyperacusis and Hearing LossDocument5 pagesNelson Chen 2004 The Relationship of Tinnitus Hyperacusis and Hearing LossSanjay SunakNo ratings yet
- OtosclerosisDocument31 pagesOtosclerosisashry909100% (1)
- Nikolaus Ronald Indra 4Document137 pagesNikolaus Ronald Indra 4Florence StellaNo ratings yet
- GOTB - Group 7 - Geriatric WorldDocument3 pagesGOTB - Group 7 - Geriatric WorldReza Afif FebriansyahNo ratings yet
- Otosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandOtosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Cortical DeafnessDocument5 pagesCortical DeafnesssakuraleeshaoranNo ratings yet
- Cochlear OtosclerosisDocument6 pagesCochlear OtosclerosisadriricaldeNo ratings yet
- Presbycusi S: By: April Fischer CSD 771 Case StudyDocument26 pagesPresbycusi S: By: April Fischer CSD 771 Case Studyminal madcapNo ratings yet
- Meniere's DiseaseDocument50 pagesMeniere's DiseaseRaisa CleizeraNo ratings yet
- Otosclerosis An Update On Diagnosis and Treatment.3Document6 pagesOtosclerosis An Update On Diagnosis and Treatment.3andiNo ratings yet
- Hertzano 2020Document12 pagesHertzano 2020Moisés AarónNo ratings yet
- Batson2017 OtosclerosisDocument6 pagesBatson2017 OtosclerosisnuhajazminNo ratings yet
- Tinnitus and Hyperacusis: Facts, Theories, and Clinical ImplicationsFrom EverandTinnitus and Hyperacusis: Facts, Theories, and Clinical ImplicationsNo ratings yet
- Matsy CytoDocument7 pagesMatsy CytoDarem SoNo ratings yet
- NEJM - 2010 điếc sâu tiếng anhDocument14 pagesNEJM - 2010 điếc sâu tiếng anhPhong HoàngNo ratings yet
- Parkinsons Disease and Hearing LossDocument8 pagesParkinsons Disease and Hearing LossJohn OmandacNo ratings yet
- Hipoacusia en AdultoDocument9 pagesHipoacusia en AdultoAngela Cañari ChumpitazNo ratings yet
- Indications To Administer Special Tests: (1) Cochlear PathologyDocument11 pagesIndications To Administer Special Tests: (1) Cochlear PathologyASMAA NOORUDHEENNo ratings yet
- What Is PresbycusisDocument4 pagesWhat Is PresbycusisNisa UcilNo ratings yet
- Presbycusis JournalDocument11 pagesPresbycusis JournalJairah CandaoNo ratings yet
- Hearing Impairment in Older People: A Review: Lisa Fook, Rosemary MorganDocument5 pagesHearing Impairment in Older People: A Review: Lisa Fook, Rosemary MorganMANGKAGENo ratings yet
- 114 Barera CsDocument15 pages114 Barera Cskaloydiaz09No ratings yet
- Kasus PresbycusDocument29 pagesKasus PresbycusSMA N 1 TOROHNo ratings yet
- Voicedisordersinthe Elderly: Karen M. Kost,, Robert T. SataloffDocument13 pagesVoicedisordersinthe Elderly: Karen M. Kost,, Robert T. SataloffFernanda MerichesNo ratings yet
- Otosclerosis & Acostic NeuromaDocument44 pagesOtosclerosis & Acostic NeuromaAbdullah AnsarNo ratings yet
- Meniere's Disease & OtosclerosisDocument44 pagesMeniere's Disease & OtosclerosisNadzirah Ahmad JailaniNo ratings yet
- Perubahan Sistem Penglihatan Dan Pendengaran Pada GeriatriDocument65 pagesPerubahan Sistem Penglihatan Dan Pendengaran Pada GeriatriT' Ade PermanaNo ratings yet
- Case Report Mata 2Document4 pagesCase Report Mata 2Hanung PujanggaNo ratings yet
- Otosclerosis: Aditya Ghosh Roy PGT-2 M.S. E.N.T. N.R.S.M.C.HDocument130 pagesOtosclerosis: Aditya Ghosh Roy PGT-2 M.S. E.N.T. N.R.S.M.C.Hanon_205487480No ratings yet
- Case Study - Macarambon, FDDocument5 pagesCase Study - Macarambon, FDUmar MacarambonNo ratings yet
- Bulvar and Psevdobulbar SyndromeDocument4 pagesBulvar and Psevdobulbar SyndromeresearchparksNo ratings yet
- Hearing Loss AssessmentDocument31 pagesHearing Loss AssessmentKIBET ERNEST MUTAINo ratings yet
- Otosclerosis Content PDFDocument12 pagesOtosclerosis Content PDFAhmed MorsyNo ratings yet
- Snoring, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSnoring, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- JOURNAL CLINICAL ManggalaDocument24 pagesJOURNAL CLINICAL ManggalaEndika CahyoNo ratings yet
- Revision Topics in OtologyDocument294 pagesRevision Topics in OtologyDr. T. Balasubramanian100% (3)
- Original Article: Bilirubin and The Auditory SystemDocument4 pagesOriginal Article: Bilirubin and The Auditory SystemjennyNo ratings yet
- CURRENT Diagnosis & Treatment in Otolaryngology-Head & Neck Surgery, 3eDocument3 pagesCURRENT Diagnosis & Treatment in Otolaryngology-Head & Neck Surgery, 3eStephanie Vania EmbangNo ratings yet
- Genetic Hearing LossDocument20 pagesGenetic Hearing LossZyan D. RiveraNo ratings yet
- HHS Public Access: Hearing Loss in AdultsDocument13 pagesHHS Public Access: Hearing Loss in AdultsClara ScemamaNo ratings yet
- SeminarDocument36 pagesSeminarKhadira MohammedNo ratings yet
- 2015 - Hildrew - A Newborn With Three Cochlear Turns Case Report and Literature ReviewDocument3 pages2015 - Hildrew - A Newborn With Three Cochlear Turns Case Report and Literature ReviewkingNo ratings yet
- Drugs Used in Otology and Their FormulationsDocument4 pagesDrugs Used in Otology and Their FormulationsAnish RajNo ratings yet
- Ramsay Hunt SyndromeDocument3 pagesRamsay Hunt SyndromeAnish RajNo ratings yet
- Middle Ear Risk Index (MERI)Document2 pagesMiddle Ear Risk Index (MERI)Anish RajNo ratings yet
- Pars Flaccida Retraction ClassificationDocument2 pagesPars Flaccida Retraction ClassificationAnish RajNo ratings yet
- Drtbalu'S Otolaryngology Online: OtophymaDocument2 pagesDrtbalu'S Otolaryngology Online: OtophymaAnish RajNo ratings yet
- Sudden Sensorineural Hearing Loss by DrtbaluDocument3 pagesSudden Sensorineural Hearing Loss by DrtbaluAnish RajNo ratings yet
- Gradenigo SyndromeDocument3 pagesGradenigo SyndromeAnish RajNo ratings yet
- Vestibular NeuronitisDocument3 pagesVestibular NeuronitisAnish RajNo ratings yet
- Alternate Loudness Balance TestDocument4 pagesAlternate Loudness Balance TestAnish RajNo ratings yet
- Perichondritis PinnaDocument2 pagesPerichondritis PinnaAnish RajNo ratings yet
- CholesteatomaDocument4 pagesCholesteatomaAnish RajNo ratings yet
- Non Organic Hearing Loss by DrtbaluDocument3 pagesNon Organic Hearing Loss by DrtbaluAnish RajNo ratings yet
- Tests of Eustachean Tube FunctionDocument3 pagesTests of Eustachean Tube FunctionAnish RajNo ratings yet
- Otoacoustic EmissionsDocument3 pagesOtoacoustic EmissionsAnish RajNo ratings yet
- Vestibular NeuritisDocument2 pagesVestibular NeuritisAnish RajNo ratings yet
- Pnuematization of Temporal BoneDocument4 pagesPnuematization of Temporal BoneAnish RajNo ratings yet
- Keratosis ObturansDocument2 pagesKeratosis ObturansAnish RajNo ratings yet
- Drtbalu'S Otolaryngology Online: StapedectomyDocument3 pagesDrtbalu'S Otolaryngology Online: StapedectomyAnish RajNo ratings yet
- Otitis Media With EffusionDocument3 pagesOtitis Media With EffusionAnish RajNo ratings yet
- Myringitis GranulosaDocument2 pagesMyringitis GranulosaAnish RajNo ratings yet
- Drtbalu'S Otolaryngology Online: MyringoplastyDocument3 pagesDrtbalu'S Otolaryngology Online: MyringoplastyAnish RajNo ratings yet
- Puberphonia and Its ManagementDocument3 pagesPuberphonia and Its ManagementAnish RajNo ratings yet
- Short Increment Sensitivity Index Test (SISI)Document2 pagesShort Increment Sensitivity Index Test (SISI)Anish RajNo ratings yet
- Physiology of External Auditory CanalDocument2 pagesPhysiology of External Auditory CanalAnish RajNo ratings yet
- Drtbalu'S Otolaryngology Online: TracheomalaciaDocument3 pagesDrtbalu'S Otolaryngology Online: TracheomalaciaAnish RajNo ratings yet
- TympanosclerosisDocument2 pagesTympanosclerosisAnish RajNo ratings yet
- Drtbalu'S Otolaryngology Online: Buy NowDocument4 pagesDrtbalu'S Otolaryngology Online: Buy NowAnish RajNo ratings yet
- Physiology of LarynxDocument2 pagesPhysiology of LarynxAnish RajNo ratings yet
- Drtbalu'S Otolaryngology Online: Acute LaryngitisDocument3 pagesDrtbalu'S Otolaryngology Online: Acute LaryngitisAnish RajNo ratings yet
- Drtbalu'S Otolaryngology Online: Vocal NoduleDocument2 pagesDrtbalu'S Otolaryngology Online: Vocal NoduleAnish RajNo ratings yet
- Medication: Expected Pharmacological Action Therapeutic UseDocument1 pageMedication: Expected Pharmacological Action Therapeutic UseclarimerNo ratings yet
- Cermin Dunia Kedokteran, No 151. 2006. P: 14-17: Daftar PustakaDocument2 pagesCermin Dunia Kedokteran, No 151. 2006. P: 14-17: Daftar PustakaLaila Kurnia PramonoNo ratings yet
- 2018 Book NeuroendocrineTumorsInRealLifeDocument348 pages2018 Book NeuroendocrineTumorsInRealLifeMayra AlejandraNo ratings yet
- Noc Emergency and Urgent Care InfographicDocument2 pagesNoc Emergency and Urgent Care InfographicWira LinNo ratings yet
- Pathophysiology, Clinical Features, And... Osis of Tetralogy of Fallot - UpToDateDocument18 pagesPathophysiology, Clinical Features, And... Osis of Tetralogy of Fallot - UpToDateRocco VasquezNo ratings yet
- Treatment Evidence Form: iUBT431 - Facial Electrical TreatmentsDocument5 pagesTreatment Evidence Form: iUBT431 - Facial Electrical TreatmentsVivi AnaNo ratings yet
- Association of TNF-? With Insulin Resistance in Type 2 DiabetesDocument4 pagesAssociation of TNF-? With Insulin Resistance in Type 2 DiabeteswikalydiaNo ratings yet
- DM Assignment 2019Document2 pagesDM Assignment 2019Rudy Roger Zepita CayojaNo ratings yet
- MCN Oral RevalidaDocument11 pagesMCN Oral RevalidaADOLF FRUELAN HIDALGONo ratings yet
- Ginek DasarDocument18 pagesGinek DasarEduward PasangkaNo ratings yet
- Disorders of PigmentationDocument68 pagesDisorders of PigmentationSajin AlexanderNo ratings yet
- Amc Requisitioned Hospital Status 03-05-2021 5.00 PM OnlineDocument7 pagesAmc Requisitioned Hospital Status 03-05-2021 5.00 PM Onlinenaresh shahNo ratings yet
- Drugs in The Neonatal Unit: 1 Julia PettyDocument5 pagesDrugs in The Neonatal Unit: 1 Julia PettyMarjoNo ratings yet
- ACLU Prison Healthcare LawsuitDocument35 pagesACLU Prison Healthcare LawsuitXerxes WilsonNo ratings yet
- Asentar Health Benefits Brochure (En) FinalDocument32 pagesAsentar Health Benefits Brochure (En) FinalarthurNo ratings yet
- Specops Jiacd 200904Document74 pagesSpecops Jiacd 200904Mario Adán100% (1)
- TyhpoidDocument8 pagesTyhpoidTanor YansaNo ratings yet
- Alvarez, Et Al. 2013. Developmental and Comparative ImmunologyDocument5 pagesAlvarez, Et Al. 2013. Developmental and Comparative ImmunologyFernandoNo ratings yet
- Do Not Copy Penalties Apply: The Role of Cutaneous Microbiota Harmony in Maintaining A Functional Skin BarrierDocument7 pagesDo Not Copy Penalties Apply: The Role of Cutaneous Microbiota Harmony in Maintaining A Functional Skin BarriereaudreyliaNo ratings yet
- Share 'Module - Safety and Sanitation 4-5.docx'Document24 pagesShare 'Module - Safety and Sanitation 4-5.docx'ana mejicoNo ratings yet
- Case Study BMC-Surgical WardDocument55 pagesCase Study BMC-Surgical WardVirgilio Reyes ManuelNo ratings yet
- JURNAL BMI PREGNANCY + Crit AppDocument55 pagesJURNAL BMI PREGNANCY + Crit Apppkm rejosariNo ratings yet
- Risk For Disturbed Personal Identity Related To Lows Elf-EsteemDocument3 pagesRisk For Disturbed Personal Identity Related To Lows Elf-EsteemPrince Juzzel BanagNo ratings yet
- Inhaled Corticosteroids Safety and Adverse Effects-DikonversiDocument8 pagesInhaled Corticosteroids Safety and Adverse Effects-DikonversiRachmi MerrinaNo ratings yet
- Poster PresentationDocument1 pagePoster Presentationapi-505989771No ratings yet
- Q&A PriorityDocument7 pagesQ&A Priorityapi-381843850% (2)
- Clinical Teaching Plan Level IV First SemesterDocument12 pagesClinical Teaching Plan Level IV First SemesterMevelle Laranjo Asuncion67% (3)
- Hearing Loss in Adults Assessment and Management PDF 1837761878725 PDFDocument20 pagesHearing Loss in Adults Assessment and Management PDF 1837761878725 PDFxtineNo ratings yet