Download as pdf or txt
You might also like
- Twelve-Month Evaluation of A Novel Mineral-Organic Adhesive Material Used To Stabilize Dental Implants Placed in Oversized Osteotomies in Vivo in An Animal ModelDocument14 pagesTwelve-Month Evaluation of A Novel Mineral-Organic Adhesive Material Used To Stabilize Dental Implants Placed in Oversized Osteotomies in Vivo in An Animal ModelAlan PollackNo ratings yet
- ABO AnalysisDocument38 pagesABO AnalysisMa Lyn Gabayeron75% (4)
- Sensodyne Marketing Strategy (PowerPoint)Document28 pagesSensodyne Marketing Strategy (PowerPoint)Thái Hữu Anh TuấnNo ratings yet
- Coronectomy: Indications, Outcomes, and Description of TechniqueDocument6 pagesCoronectomy: Indications, Outcomes, and Description of TechniqueHélio FonteneleNo ratings yet
- Oral Wound Healing: Cell Biology and Clinical ManagementFrom EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaNo ratings yet
- Gnatus SyncrusDocument36 pagesGnatus SyncrusFill100% (1)
- Dam-It, It's Easy: Handbook of Basic Dental Dam ProceduresDocument32 pagesDam-It, It's Easy: Handbook of Basic Dental Dam ProceduresNonoNo ratings yet
- Surgical Management of A Large Periapical Lesion With PRF and Xenograft - A Case ReportDocument3 pagesSurgical Management of A Large Periapical Lesion With PRF and Xenograft - A Case ReportJohn SmithNo ratings yet
- Cairo Clasificaion ResecionDocument7 pagesCairo Clasificaion ResecionMartty BaNo ratings yet
- Inferior Alveolar Nerve Block Anesthesia Via The Retromolar Triangle, An Alternative For Patients With Blood DyscrasiasDocument5 pagesInferior Alveolar Nerve Block Anesthesia Via The Retromolar Triangle, An Alternative For Patients With Blood DyscrasiasGina CastilloNo ratings yet
- The Periodontal Pocket: Pathogenesis, Histopathology and ConsequencesDocument8 pagesThe Periodontal Pocket: Pathogenesis, Histopathology and ConsequencesChaudhari Sonali100% (1)
- Endodontic-Periodontal Lesion: A Two-Way Traffic: Dr. Anindya Priya Saha, Dr. Anindya Chakraborty and Dr. Sananda SahaDocument6 pagesEndodontic-Periodontal Lesion: A Two-Way Traffic: Dr. Anindya Priya Saha, Dr. Anindya Chakraborty and Dr. Sananda Sahanovia chantikaNo ratings yet
- Klasifikasi Impaksi Caninus Rahang Atas Pada Pemeriksaan Radiograf Panoramik Dan CBCT Sebagai Penunjang OdontomyDocument8 pagesKlasifikasi Impaksi Caninus Rahang Atas Pada Pemeriksaan Radiograf Panoramik Dan CBCT Sebagai Penunjang OdontomyRahmi WastriNo ratings yet
- Endo-Perio ArticleDocument7 pagesEndo-Perio ArticleHajra FarooqNo ratings yet
- AAP Parameters of Care Periodontics 9Document3 pagesAAP Parameters of Care Periodontics 9Tanmay JhulkaNo ratings yet
- JIAP October 2019 - Association Between Traumatic Occlusal Forces and Periodontitis - A Systematic ReviewDocument11 pagesJIAP October 2019 - Association Between Traumatic Occlusal Forces and Periodontitis - A Systematic ReviewGusnia IraNo ratings yet
- Surgical Periodontal TherapyDocument11 pagesSurgical Periodontal TherapyGonzalo Becerra LeonartNo ratings yet
- Jurnal Scalling Dan Root PlaningDocument17 pagesJurnal Scalling Dan Root PlaningJesicaNo ratings yet
- The Key To Profound Local Anesthesia: NeuroanatomyDocument8 pagesThe Key To Profound Local Anesthesia: NeuroanatomyRavik FidayatikaNo ratings yet
- Catherine A. Hebert, D.D.S .: Internal Vs External ResorptionDocument2 pagesCatherine A. Hebert, D.D.S .: Internal Vs External ResorptionJames OnealNo ratings yet
- ResearchDocument4 pagesResearchEmmanuel Isaac GohNo ratings yet
- Effect of Gingival Biotype On Orthodontic TreatmenDocument8 pagesEffect of Gingival Biotype On Orthodontic Treatmensolodont1No ratings yet
- Keratocystic Odontogenic Tumor A Case ReportDocument3 pagesKeratocystic Odontogenic Tumor A Case ReportDr.Anand Pratap SinghNo ratings yet
- Implant-Supported Overdentures: Part 2: ClinicalDocument7 pagesImplant-Supported Overdentures: Part 2: ClinicalDhanasriNo ratings yet
- ADA Chairside Guide Periodontitis PDFDocument2 pagesADA Chairside Guide Periodontitis PDFАнна Шаповалова100% (1)
- White Sponge NevusDocument2 pagesWhite Sponge Nevusbundahara zoomNo ratings yet
- Practice: Failures in Implant DentistryDocument7 pagesPractice: Failures in Implant DentistryhmsatNo ratings yet
- Acute Periapical AbscessDocument12 pagesAcute Periapical AbscessDarshilNo ratings yet
- Practical ApplicationsDocument9 pagesPractical ApplicationsCristian OneaNo ratings yet
- IndianJDentSci92126-1778286 045622Document8 pagesIndianJDentSci92126-1778286 045622Debora NatalynaNo ratings yet
- 2022 @dentolib Antigoni Delantoni, Kaan Orhan Atlas of DentomaxillofacialDocument229 pages2022 @dentolib Antigoni Delantoni, Kaan Orhan Atlas of Dentomaxillofacialc8dqt289hfNo ratings yet
- The Relation of Canine Guidance With Laterotrusive Movements at The Incisal Point and The Working Side CondyleDocument7 pagesThe Relation of Canine Guidance With Laterotrusive Movements at The Incisal Point and The Working Side Condyleandutzu_euNo ratings yet
- Periodontitis Classification and Staging PDFDocument9 pagesPeriodontitis Classification and Staging PDFAnonymous 7YkiHucQlONo ratings yet
- Periodontal Plastic SurgeryDocument5 pagesPeriodontal Plastic Surgeryudhai170819No ratings yet
- Splinting Journal PDFDocument7 pagesSplinting Journal PDFhanataniarNo ratings yet
- Guideline On Dental Management of Pediatric Patients Receiving Chemotherapy, Hematopoietic Cell Transplantation, And/or RadiationDocument7 pagesGuideline On Dental Management of Pediatric Patients Receiving Chemotherapy, Hematopoietic Cell Transplantation, And/or RadiationMariele Pototski AmenabarNo ratings yet
- IRTDocument2 pagesIRTIgnacioNo ratings yet
- Dentistry EmergenciesDocument5 pagesDentistry EmergenciesSofia PereiraNo ratings yet
- Implant-Related Complications and FailuresDocument91 pagesImplant-Related Complications and FailuresSaman MohammadzadehNo ratings yet
- T-Cap 10091Document9 pagesT-Cap 10091Joshua Diaz QuiquijanaNo ratings yet
- Endodontic Treatment of Dens InvaginatusDocument7 pagesEndodontic Treatment of Dens InvaginatusParidhi GargNo ratings yet
- Altered Active and Passive Eruption A Modified ClassificationDocument7 pagesAltered Active and Passive Eruption A Modified ClassificationMara CondorNo ratings yet
- Endo Perio2Document9 pagesEndo Perio2Fernando CordovaNo ratings yet
- Inter-Proximal Enamel Reduction in Contemporary OrthodonticsDocument7 pagesInter-Proximal Enamel Reduction in Contemporary OrthodonticsAly OsmanNo ratings yet
- Midline Diastema Treatment OptionsDocument6 pagesMidline Diastema Treatment OptionsnandaNo ratings yet
- Computerized Occlusal Analysis As An Alternative Occlusal IndicatorDocument6 pagesComputerized Occlusal Analysis As An Alternative Occlusal IndicatorMariana RaduNo ratings yet
- The Zygoma Anatomy Guided Approach For Placement of Zygomatic ImplantsDocument29 pagesThe Zygoma Anatomy Guided Approach For Placement of Zygomatic ImplantsLê Minh KhôiNo ratings yet
- Periodontal Osseous Defects A Review PDFDocument8 pagesPeriodontal Osseous Defects A Review PDFLorenaCastanoGarzonNo ratings yet
- JIAP July 2011 - Guided Tissue Regeneration - A Decision-Making ModelDocument8 pagesJIAP July 2011 - Guided Tissue Regeneration - A Decision-Making ModelLouis HutahaeanNo ratings yet
- Black Triangle PDFDocument4 pagesBlack Triangle PDFzinniaNo ratings yet
- Orthognatic Surgery:: 1. Slide 1 DefinitionDocument8 pagesOrthognatic Surgery:: 1. Slide 1 Definitionammarstein89No ratings yet
- The Socket Shield Technique Case ReportDocument5 pagesThe Socket Shield Technique Case ReportAhmed Mohammed Saaduddin SapriNo ratings yet
- Etiology and Pathogenesis of Aggressive Periodontitis: A Mini ReviewDocument5 pagesEtiology and Pathogenesis of Aggressive Periodontitis: A Mini ReviewBagas SuryonegoroNo ratings yet
- Case Selection in Dental Implant TherapyDocument4 pagesCase Selection in Dental Implant Therapymichealraj rousseauNo ratings yet
- Extraction Socket Presenvation Using A Collagen Plug Combined With Platelet Rich Plasma (PRP) RADIOGRAPIHICDocument7 pagesExtraction Socket Presenvation Using A Collagen Plug Combined With Platelet Rich Plasma (PRP) RADIOGRAPIHICrachmadyNo ratings yet
- PEAK Success or Failure of Dental Implants A Literature Review With Treatment ConsiderationsDocument10 pagesPEAK Success or Failure of Dental Implants A Literature Review With Treatment ConsiderationsJani MehulNo ratings yet
- Bone Regeneration in DentistryDocument5 pagesBone Regeneration in Dentistryclaudia360No ratings yet
- Dentoalveolar Injuries and Wiring TechniquesDocument60 pagesDentoalveolar Injuries and Wiring Techniquessamys2ndemailNo ratings yet
- Injectable Platelet Rich Fibrin (i-PRF) : Opportunities in Regenerative Dentistry?Document9 pagesInjectable Platelet Rich Fibrin (i-PRF) : Opportunities in Regenerative Dentistry?RENATO SUDATINo ratings yet
- Gingiva in Health and DiseaseDocument39 pagesGingiva in Health and Diseaseaichayehdih booksNo ratings yet
- A Cavernous Sinus Infection A Root Canal CaseDocument4 pagesA Cavernous Sinus Infection A Root Canal CaseCarmen-BadeaNo ratings yet
- 08 - Salivary Biomarkers A Periodontal OverviewDocument6 pages08 - Salivary Biomarkers A Periodontal OverviewFisaNo ratings yet
- AAE Position Statement On Vital Pulp Therapy 2021Document10 pagesAAE Position Statement On Vital Pulp Therapy 2021Abhishek Isaac Mathew100% (1)
- Review Article: Hypodontia: An Update On Its Etiology, Classification, and Clinical ManagementDocument9 pagesReview Article: Hypodontia: An Update On Its Etiology, Classification, and Clinical Managementionut1ilie-1No ratings yet
- Artigo TainahDocument9 pagesArtigo TainahManuela TimbóNo ratings yet
- Sticky Bone For Space Maintenance in The Treatment of Miller's Class I Gingival Recession Defects With VISTA Technique A Case SeriesDocument4 pagesSticky Bone For Space Maintenance in The Treatment of Miller's Class I Gingival Recession Defects With VISTA Technique A Case SeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hyaluronic Acid: Perspectives in Dentistry. A Systematic ReviewDocument11 pagesHyaluronic Acid: Perspectives in Dentistry. A Systematic Reviewjeimmy dulceyNo ratings yet
- Malocclusion Classification PDFDocument115 pagesMalocclusion Classification PDFDr.khalandar khatibNo ratings yet
- Mclaurin 2020Document9 pagesMclaurin 2020magus davilaNo ratings yet
- ARTICLE 2 - Experience of Dental Among Aboriginal Children in Selangor, MsiaDocument6 pagesARTICLE 2 - Experience of Dental Among Aboriginal Children in Selangor, MsiaCak IzaTyNo ratings yet
- The Retention Characteristics of Hawley and Vacuum-FormedDocument8 pagesThe Retention Characteristics of Hawley and Vacuum-FormedYayis LondoñoNo ratings yet
- Dental X-Ray Identifications: Prepared By: Houssam Ali Submitted To: DR - Nayer El SaadDocument31 pagesDental X-Ray Identifications: Prepared By: Houssam Ali Submitted To: DR - Nayer El SaadreemNo ratings yet
- Program Curs RestorativeDocument7 pagesProgram Curs Restorativeflorin serafinNo ratings yet
- National Board Dental Examination I Answer KEY Anatomic Sciences JULY 1978Document1 pageNational Board Dental Examination I Answer KEY Anatomic Sciences JULY 1978Arif ShaikhNo ratings yet
- Anatomical Landmarks and Primary ImpressionDocument67 pagesAnatomical Landmarks and Primary ImpressionAswitha GanapathyNo ratings yet
- Effective Protocol For Daily High-Quality Direct Posterior Composite Restorations. The Interdental Anatomy of The Class-2 Composite RestorationDocument14 pagesEffective Protocol For Daily High-Quality Direct Posterior Composite Restorations. The Interdental Anatomy of The Class-2 Composite RestorationjonvargasNo ratings yet
- Skeletal Maturity IndicatorsDocument55 pagesSkeletal Maturity IndicatorsChetan ShankarNo ratings yet
- Journal Homepage: - : IntroductionDocument9 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Modern Endodontic Part 4 IrrigationDocument9 pagesModern Endodontic Part 4 IrrigationKaterine RiquelmeNo ratings yet
- 18-2Document110 pages18-2RendiPratamaIINo ratings yet
- Bingo Parts of The Body PDFDocument19 pagesBingo Parts of The Body PDFPao PerezNo ratings yet
- Fujita 2009Document6 pagesFujita 2009Naji Z. ArandiNo ratings yet
- Alveolar Bone GraftingDocument13 pagesAlveolar Bone GraftingDayal SharanNo ratings yet
- BIOFLXDocument22 pagesBIOFLXShameena KnNo ratings yet
- Dr. Karam Abu Shakra 42-10Document8 pagesDr. Karam Abu Shakra 42-10Herpika DianaNo ratings yet
- Lingual-Keys For SuccessDocument8 pagesLingual-Keys For SuccessGoutam NookalaNo ratings yet
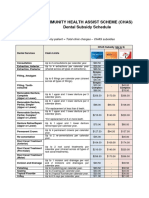
- CHAS Dental Subsidy ScheduleDocument1 pageCHAS Dental Subsidy ScheduleEugeneNo ratings yet
- Beautifil Flow Plus: Injectable Hybrid Restorative Material For Anterior and Posterior TeethDocument6 pagesBeautifil Flow Plus: Injectable Hybrid Restorative Material For Anterior and Posterior TeethIrina CebotaruNo ratings yet
- Ijcmr - 1761Document2 pagesIjcmr - 1761Mukarram FaridiNo ratings yet