Download as doc, pdf, or txt
You might also like
- Techniques Grief TherapyDocument24 pagesTechniques Grief TherapyMArko89% (9)
- Emotional Literacy Course Notes: Phase 1Document7 pagesEmotional Literacy Course Notes: Phase 1MArko100% (1)
- Bells Adjustment Inventory FinalDocument17 pagesBells Adjustment Inventory FinalJhilmil GroverNo ratings yet
- Techniques in Writing One Act PlayDocument6 pagesTechniques in Writing One Act Playazu azuNo ratings yet
- BPD Fact SheetDocument2 pagesBPD Fact Sheetsiknobostu50% (4)
- Narcissism and Sadomasochistic RelationshipsDocument9 pagesNarcissism and Sadomasochistic RelationshipsjuaromerNo ratings yet
- Children of Mothers With Borderline Personality Disorder (BPD)Document6 pagesChildren of Mothers With Borderline Personality Disorder (BPD)curiositykillcat100% (1)
- Maladaptive Coping Modes Perfectionistic OvercompensatorDocument2 pagesMaladaptive Coping Modes Perfectionistic OvercompensatorMArko100% (1)
- Graded Exposure WorksheetDocument2 pagesGraded Exposure WorksheetMArkoNo ratings yet
- DBT - Rad S BorderlineomDocument34 pagesDBT - Rad S BorderlineomMArkoNo ratings yet
- Ask Method List Building BlueprintDocument22 pagesAsk Method List Building BlueprintMArko100% (2)
- Lesson Plan Template TemperatureDocument3 pagesLesson Plan Template Temperatureapi-338756826No ratings yet
- 3b. Borderline Personality Disorder 2021Document14 pages3b. Borderline Personality Disorder 2021spartanNo ratings yet
- The Intersectionality of Bipolar Disorder With Borderline Personality DisorderDocument14 pagesThe Intersectionality of Bipolar Disorder With Borderline Personality DisorderMuskaanNo ratings yet
- Borderline Personality Disorder Implications in Family and Pediatric Practice 2161 0487.1000122Document6 pagesBorderline Personality Disorder Implications in Family and Pediatric Practice 2161 0487.1000122Farida DurotulNo ratings yet
- Borderline Personality Disorder: The ultimate guide to borderline personality disorder including signs and symptoms, diagnosis, treatment, and how to improve and manage it!From EverandBorderline Personality Disorder: The ultimate guide to borderline personality disorder including signs and symptoms, diagnosis, treatment, and how to improve and manage it!No ratings yet
- CBT for Borderline Personality Disorder: A Step-by-Step Comprehensive Guide to Emotional Regulation, Mindfulness, and Interpersonal Skills for Lasting RecoveryFrom EverandCBT for Borderline Personality Disorder: A Step-by-Step Comprehensive Guide to Emotional Regulation, Mindfulness, and Interpersonal Skills for Lasting RecoveryNo ratings yet
- Borderline Personality DisorderDocument9 pagesBorderline Personality DisorderSiva Nandhan0% (1)
- Understanding BPD 2012 PDFDocument20 pagesUnderstanding BPD 2012 PDFkei_1808100% (2)
- Attachment and Borderline Personality DisorderDocument18 pagesAttachment and Borderline Personality Disorderme13No ratings yet
- IQ SampleDocument6 pagesIQ SamplenesumaNo ratings yet
- Borderline Personality DisorderDocument16 pagesBorderline Personality DisorderRaissa100% (1)
- Avoidance Personality Disorder #1Document4 pagesAvoidance Personality Disorder #1Angelo ProvidoNo ratings yet
- Personality Disorder - WikipediaDocument36 pagesPersonality Disorder - WikipediaAhmad Tohir Nasution100% (1)
- Borderline Personality DisordersDocument24 pagesBorderline Personality DisordersWan AfwanNo ratings yet
- Borderline Personality Disorder: Raising Questions, Finding AnswersDocument4 pagesBorderline Personality Disorder: Raising Questions, Finding AnswerslalichompyNo ratings yet
- DSM distributed system management Complete Self-Assessment GuideFrom EverandDSM distributed system management Complete Self-Assessment GuideNo ratings yet
- DSM Individual AdultDocument6 pagesDSM Individual AdultAngel J. Combs100% (1)
- Conflict and AttitudeDocument9 pagesConflict and AttitudesheqarayzanNo ratings yet
- BPD in Young PeopleDocument8 pagesBPD in Young PeopleMaria Von ShaftNo ratings yet
- Borderline ScreeningDocument3 pagesBorderline ScreeningAlexandreDuarteGiganteNo ratings yet
- Old Lecture 10b (Rorschach)Document35 pagesOld Lecture 10b (Rorschach)mariaNo ratings yet
- NCM 105 Childhood Developmental DoDocument12 pagesNCM 105 Childhood Developmental DoSandra GabasNo ratings yet
- APA DSM5TR ThePersonalityInventoryForDSM5BriefFormAdultDocument3 pagesAPA DSM5TR ThePersonalityInventoryForDSM5BriefFormAdultUmut DoğanNo ratings yet
- Orderline Ersonality Isorder: Patricia Lam, Ollivia Perea, Nancy Phan & Maribel Ocampo Period 4Document13 pagesOrderline Ersonality Isorder: Patricia Lam, Ollivia Perea, Nancy Phan & Maribel Ocampo Period 4api-277488150100% (1)
- Co-Parenting With Someone With Borderline Personality Disorder - FatherResourceDocument1 pageCo-Parenting With Someone With Borderline Personality Disorder - FatherResourcechumbucketNo ratings yet
- MCMI-III Victor LalhmangaihkimaDocument12 pagesMCMI-III Victor LalhmangaihkimaVictor YanafNo ratings yet
- Psychotherapy For Borderline Personality Disorder: PsychiatryDocument4 pagesPsychotherapy For Borderline Personality Disorder: PsychiatryAnonymous 75M6uB3OwNo ratings yet
- Exploring The Relationship Between Non Suicidal Self-Injury and Borderline Personality Traits in Young AdultsDocument9 pagesExploring The Relationship Between Non Suicidal Self-Injury and Borderline Personality Traits in Young Adultsme13No ratings yet
- The Psychiatric Assessment NotebookDocument4 pagesThe Psychiatric Assessment NotebookSean Goddard NPNo ratings yet
- Psy Health, Insel & Roth, Core Concepts in Health 2008, Chap PDFDocument21 pagesPsy Health, Insel & Roth, Core Concepts in Health 2008, Chap PDFMarcelo Vial RoeheNo ratings yet
- Borderline Personality Disorder - Wikipedia The Free Encyclope PDFDocument34 pagesBorderline Personality Disorder - Wikipedia The Free Encyclope PDFstephNo ratings yet
- Shared Psychotic Disorder - NCBIDocument8 pagesShared Psychotic Disorder - NCBI5KevNo ratings yet
- Counselling Pschology UNIT-1Document7 pagesCounselling Pschology UNIT-1NehaNo ratings yet
- Psychiatric Disorders: Dr. Adelene L. YanoDocument56 pagesPsychiatric Disorders: Dr. Adelene L. YanoMarhama MagarangNo ratings yet
- QIDS SR16 DepressionDocument3 pagesQIDS SR16 DepressionSergioMSaraivaNo ratings yet
- APA - DSM5 - The Personality Inventory For DSM 5 Full Version InformantDocument9 pagesAPA - DSM5 - The Personality Inventory For DSM 5 Full Version InformantJacques SavariauNo ratings yet
- Understanding: Schizoaffective DisorderDocument24 pagesUnderstanding: Schizoaffective DisorderGemma GarciaNo ratings yet
- BORDERLINE - PERSONALITY - DISORDER Good PDFDocument29 pagesBORDERLINE - PERSONALITY - DISORDER Good PDFZsoldos Marianna100% (3)
- Early Identification Psychosis: PrimerDocument16 pagesEarly Identification Psychosis: PrimerGrace LNo ratings yet
- Borderline Personality Disorder, Complex Trauma, and ProblemsDocument18 pagesBorderline Personality Disorder, Complex Trauma, and ProblemsGeymy Natali Castiblanco QuevedoNo ratings yet
- Assessment and Diagnosis of Personality Disorders by Armand W. Loranger PDFDocument239 pagesAssessment and Diagnosis of Personality Disorders by Armand W. Loranger PDFAndrew Wongkar100% (4)
- Borderline Personality Disorder (BPD)Document13 pagesBorderline Personality Disorder (BPD)Hari BabooNo ratings yet
- Personality DisordersDocument125 pagesPersonality DisordersDevendra Singh Baryah100% (3)
- Aggression QuestionnaireDocument2 pagesAggression QuestionnaireMichelle LanguianNo ratings yet
- Behavioral Guide To Personality Disorders - (DSM-5) (2015) by Douglas H. RubenDocument275 pagesBehavioral Guide To Personality Disorders - (DSM-5) (2015) by Douglas H. RubenCristianBale100% (9)
- Psychiatric Rating Scales-RRFINALDocument45 pagesPsychiatric Rating Scales-RRFINALnkivc100% (1)
- APA - (2011) DSM-5 Development. Personality and Personality DisordersDocument16 pagesAPA - (2011) DSM-5 Development. Personality and Personality DisordersRodrigo Middleton InfanteNo ratings yet
- Signs and Symptoms May Include:: Cluster B Anti Social Personality DisorderDocument2 pagesSigns and Symptoms May Include:: Cluster B Anti Social Personality DisorderCake Man100% (1)
- EmotionalDocument7 pagesEmotionalapi-367611011No ratings yet
- CEG - The Values Exercise - Free GuideDocument2 pagesCEG - The Values Exercise - Free GuideHa Uyen NguyenNo ratings yet
- Handout GuidanceDocument2 pagesHandout GuidanceKhrycys Olairez RNNo ratings yet
- Pathological Narcissism and Narcissistic Personality DisorderDocument26 pagesPathological Narcissism and Narcissistic Personality DisorderAlex RodriguesNo ratings yet
- Psychosis ObjectivesDocument14 pagesPsychosis ObjectivesfatenNo ratings yet
- BPD MagazineDocument92 pagesBPD Magazinetan hangNo ratings yet
- DSM 5 Adhd Fact SheetDocument2 pagesDSM 5 Adhd Fact SheetMario MendozaNo ratings yet
- The Emotional Pain and Distress of Borderline Personality DisorderDocument9 pagesThe Emotional Pain and Distress of Borderline Personality Disorderme13No ratings yet
- The Columbia Suicide Severity Rating Scale PDFDocument21 pagesThe Columbia Suicide Severity Rating Scale PDFTri Anny Rakhmawati0% (1)
- Dabrowski 201Document686 pagesDabrowski 201MArkoNo ratings yet
- The Importance of The Vulnerable Child Mode Vulnerable Child ModeDocument2 pagesThe Importance of The Vulnerable Child Mode Vulnerable Child ModeMArkoNo ratings yet
- Behavioral Experiments To Test Beliefs WorksheetDocument2 pagesBehavioral Experiments To Test Beliefs WorksheetMArkoNo ratings yet
- Transactional Analysis 100 Key Points and TechniquDocument9 pagesTransactional Analysis 100 Key Points and TechniquMArko0% (1)
- Dependacny Issues 3Document1 pageDependacny Issues 3MArkoNo ratings yet
- How To Control People: Biderman's Chart On Penal Coercion (Amnesty International Report On Torture, 1983)Document1 pageHow To Control People: Biderman's Chart On Penal Coercion (Amnesty International Report On Torture, 1983)MArkoNo ratings yet
- My Own Authority QuestionDocument1 pageMy Own Authority QuestionMArkoNo ratings yet
- Imagery Based Exposure WorksheetDocument3 pagesImagery Based Exposure WorksheetMArkoNo ratings yet
- Imagery For Self Help: Start Each Visualisation With Relaxation by Getting Comfortable in A Quiet PlaceDocument3 pagesImagery For Self Help: Start Each Visualisation With Relaxation by Getting Comfortable in A Quiet PlaceMArkoNo ratings yet
- Grounding and Self Soothing Techniques PDFDocument2 pagesGrounding and Self Soothing Techniques PDFMArkoNo ratings yet
- A Diagram of The Schema Therapy Modes ConceptualisationDocument1 pageA Diagram of The Schema Therapy Modes ConceptualisationMArkoNo ratings yet
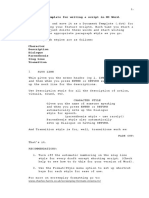
- This Is A Template For Writing A Script in MS Word.: WWW - Charles-Harris - Co.uk/screenplay-Formats-Cinema-TvDocument2 pagesThis Is A Template For Writing A Script in MS Word.: WWW - Charles-Harris - Co.uk/screenplay-Formats-Cinema-TvMArkoNo ratings yet
- Sample Soil ReportDocument64 pagesSample Soil Reportসন্দীপ চন্দ্রNo ratings yet
- Test - Present - Perfect - Review 9th 1Document3 pagesTest - Present - Perfect - Review 9th 1greidy nicolay cucaita moralesNo ratings yet
- The Effect of Information Technology, Digital Transformation, and Job Satisfaction On Employee Performance in Regional Office The National Land AgencyDocument12 pagesThe Effect of Information Technology, Digital Transformation, and Job Satisfaction On Employee Performance in Regional Office The National Land AgencyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- MC 10148034 9999Document2 pagesMC 10148034 9999Fawlus AydinNo ratings yet
- IELTS2021-Listening-Section 2Document5 pagesIELTS2021-Listening-Section 2Asuna NguyễnNo ratings yet
- Biggles Does Some HomeworkDocument6 pagesBiggles Does Some Homeworkaxhwefzod100% (1)
- Tài Liệu Livestream: Hạ Gục Câu Hỏi Từ Vựng Mức 9+ Trong Đề Thi (Buổi 4)Document2 pagesTài Liệu Livestream: Hạ Gục Câu Hỏi Từ Vựng Mức 9+ Trong Đề Thi (Buổi 4)Phương Ngọc LạiNo ratings yet
- Culture As Colloquy: Flann O'Brien's Post Modern Dialogue With Irish TraditionDocument24 pagesCulture As Colloquy: Flann O'Brien's Post Modern Dialogue With Irish Traditionbooksgirl12No ratings yet
- Chords John-Lennon Happy-ChristmasDocument3 pagesChords John-Lennon Happy-ChristmasCristian CalzoneNo ratings yet
- The New York Times Magazine - 16-06-2019Document56 pagesThe New York Times Magazine - 16-06-2019Ferran Roig100% (2)
- State Sovereign Immunity and The False Claims ActDocument38 pagesState Sovereign Immunity and The False Claims ActDex DexNo ratings yet
- King O' The Cats: Told by Aaron ShepardDocument19 pagesKing O' The Cats: Told by Aaron ShepardIra BerunioNo ratings yet
- Sentences ProjectDocument27 pagesSentences ProjectArpit SinghalNo ratings yet
- Wish WorksheetDocument4 pagesWish WorksheetelvicoNo ratings yet
- Ratio Analysis For Central Bank of IndiaDocument3 pagesRatio Analysis For Central Bank of IndiaGopal BiyaniNo ratings yet
- Western Mindanao State University College of Nursing: Zamboanga CityDocument11 pagesWestern Mindanao State University College of Nursing: Zamboanga CitySHAINA ALIH. JUMAANINo ratings yet
- USSH - Writing B1 - TopicsDocument2 pagesUSSH - Writing B1 - TopicsMu MiNo ratings yet
- Victimology at The Transition From The 20th To The 21st Century PDFDocument19 pagesVictimology at The Transition From The 20th To The 21st Century PDFatjoerossNo ratings yet
- MI6 Chief Alex Younger Full SpeechDocument13 pagesMI6 Chief Alex Younger Full SpeechLatika M BourkeNo ratings yet
- Urine Formation. PDF My NoteDocument11 pagesUrine Formation. PDF My NoteSurya JoyNo ratings yet
- Allahabad Bank: Engagement of Chief Customer Service Officer (CCSO) On Contract BasisDocument2 pagesAllahabad Bank: Engagement of Chief Customer Service Officer (CCSO) On Contract BasisHari PrasadNo ratings yet
- Ch.3 Catalase Worksheet AnswerDocument2 pagesCh.3 Catalase Worksheet AnswerJoe GuNo ratings yet
- COT Watch MaterialDocument6 pagesCOT Watch MaterialRay PatriarcaNo ratings yet
- Cambridge International A Level: Mathematics 9709/32 May/June 2021Document19 pagesCambridge International A Level: Mathematics 9709/32 May/June 2021HADFINA DAMIA BINTI SHAHIDINNo ratings yet
- Python VS KotlinDocument4 pagesPython VS KotlinAravind Naveen gamesNo ratings yet
- Balsa DataDocument13 pagesBalsa DataPaul RodgersNo ratings yet
- Components of CurriculumDocument32 pagesComponents of CurriculumMaslog Es75% (4)
- 24 Seaoil V AutocorpDocument1 page24 Seaoil V AutocorpAleli Joyce BucuNo ratings yet