Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- MSC Nursing QN PaperDocument9 pagesMSC Nursing QN Papersanthyakunjumon100% (1)
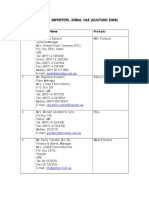
- Gulf Importer List Dubai UAEDocument5 pagesGulf Importer List Dubai UAEKharisma Rizky Nugraha100% (1)
- Assignment Speech Disorder - I Topic Cluttering (Symptoms, Eitology, and Treatment Apporaches)Document8 pagesAssignment Speech Disorder - I Topic Cluttering (Symptoms, Eitology, and Treatment Apporaches)adeeba ramzan100% (1)
- Medical Necessity Physician LetterDocument1 pageMedical Necessity Physician LetterMichael_Lee_RobertsNo ratings yet
- 5 X 5 Rmnch+aDocument2 pages5 X 5 Rmnch+aManish Chandra Prabhakar0% (1)
- Guidelines For Maternal Death Surveillance & ResponseDocument148 pagesGuidelines For Maternal Death Surveillance & ResponseManish Chandra Prabhakar100% (3)
- IMA - Rules and Bye-Laws, 2019 PDFDocument100 pagesIMA - Rules and Bye-Laws, 2019 PDFManish Chandra PrabhakarNo ratings yet
- Concept Origin Development of Social SecuritiesDocument48 pagesConcept Origin Development of Social SecuritiesManish Chandra PrabhakarNo ratings yet
- Social Security in India - Historical Development and Labour PolicyDocument29 pagesSocial Security in India - Historical Development and Labour PolicyManish Chandra Prabhakar100% (1)
- National Guidelines For Screening of Hypothyroidism During PregnancyDocument48 pagesNational Guidelines For Screening of Hypothyroidism During PregnancyManish Chandra PrabhakarNo ratings yet
- Manish Chandra Prabhakar Mgims: 1 Reference-Harrison's Internal Medicine 18th EditionDocument79 pagesManish Chandra Prabhakar Mgims: 1 Reference-Harrison's Internal Medicine 18th EditionManish Chandra PrabhakarNo ratings yet
- Mhcet 2015 v44 KeyDocument2 pagesMhcet 2015 v44 KeyChemudupati BharaniNo ratings yet
- Maharashtra Medical PG Entrance 2014 QuestionDocument32 pagesMaharashtra Medical PG Entrance 2014 QuestionManish Chandra PrabhakarNo ratings yet
- Diabetes Care Guidelines - ADA 2014Document9 pagesDiabetes Care Guidelines - ADA 2014Manish Chandra PrabhakarNo ratings yet
- Stipend Increased For Intern Doctors at MUHS NashikDocument2 pagesStipend Increased For Intern Doctors at MUHS NashikManish Chandra Prabhakar100% (1)
- A Small Truth To Make Life 100%Document9 pagesA Small Truth To Make Life 100%qistina16No ratings yet
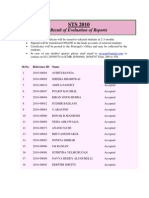
- ICMR STS 2010 Report Submission ResultsDocument27 pagesICMR STS 2010 Report Submission ResultsManish Chandra PrabhakarNo ratings yet
- Sri Sri Durga Saptshati (Sanskrit - Hindi)Document241 pagesSri Sri Durga Saptshati (Sanskrit - Hindi)Mukesh K. Agrawal62% (13)
- Research Article Published in Plose One - Manish Chandra PrabhakarDocument6 pagesResearch Article Published in Plose One - Manish Chandra PrabhakarManish Chandra Prabhakar100% (1)
- NEET PG 2012 Entrance Examination and PatternDocument4 pagesNEET PG 2012 Entrance Examination and PatternManish Chandra Prabhakar100% (1)
- Icmr Sts Result 2011Document32 pagesIcmr Sts Result 2011Manish Chandra PrabhakarNo ratings yet
- NEET PG 2013 Information Booklet FINALDocument88 pagesNEET PG 2013 Information Booklet FINALManish Chandra PrabhakarNo ratings yet
- Dizziness in The Elderly: Steven Zweig, MD Family and Community Medicine MU School of MedicineDocument34 pagesDizziness in The Elderly: Steven Zweig, MD Family and Community Medicine MU School of MedicineManish Chandra PrabhakarNo ratings yet
- How To WriteDocument13 pagesHow To WriteSebastian Quiroz FloresNo ratings yet
- QU EHSMS Training - Contractor Management Training PresenstationDocument44 pagesQU EHSMS Training - Contractor Management Training PresenstationAlizamin SyedNo ratings yet
- Lactulose DrugDocument3 pagesLactulose DrugjangzieNo ratings yet
- Course Syllabus For NSTP-Cwts/Lts 2: 2 SemesterDocument16 pagesCourse Syllabus For NSTP-Cwts/Lts 2: 2 SemesterEugene A. EstacioNo ratings yet
- Dayton Letter To IBMDocument5 pagesDayton Letter To IBMMinnesota Public RadioNo ratings yet
- PgsgaDocument2 pagesPgsgaArsela Rindang AzhariNo ratings yet
- Labconco ManualDocument69 pagesLabconco ManualFredy Fernando Huarhua GarciaNo ratings yet
- Exercise Labels and Procedure TextDocument3 pagesExercise Labels and Procedure TextivhaNo ratings yet
- FACT SHEET Modern Beef Production 26-01-11Document1 pageFACT SHEET Modern Beef Production 26-01-11Livestock Managementist IubNo ratings yet
- Ismenore: You Should Also DoDocument2 pagesIsmenore: You Should Also DoNurul Ilmi UtamiNo ratings yet
- Medicina 58 01758Document8 pagesMedicina 58 01758charlaayasyafefiNo ratings yet
- Breast Imaging Review - A Quick Guide To Essential Diagnoses (2nd Edition) PDFDocument264 pagesBreast Imaging Review - A Quick Guide To Essential Diagnoses (2nd Edition) PDFGregorio Parra100% (3)
- Santrock 0072990597 ch04Document29 pagesSantrock 0072990597 ch04Desi Purnamasari YanwarNo ratings yet
- Learning Library PDFDocument65 pagesLearning Library PDFBayu SaksonoNo ratings yet
- E-Prescription Across Europe: Health and Technology September 2013Document16 pagesE-Prescription Across Europe: Health and Technology September 2013ifrahNo ratings yet
- Potential For Excessive GriefDocument7 pagesPotential For Excessive GriefKarl ZweinertNo ratings yet
- YL NeneDocument10 pagesYL NeneHarindra DunuwilaNo ratings yet
- Human Rights Policy Poster English UsDocument1 pageHuman Rights Policy Poster English UsLahiruNo ratings yet
- Trojan: Power Station 600Document32 pagesTrojan: Power Station 600MfaneloNo ratings yet
- Document 5 LayoutDocument124 pagesDocument 5 LayoutAlejandro Moro HigelmoNo ratings yet
- Persiapan UN SMKDocument5 pagesPersiapan UN SMKBryce SchmidtNo ratings yet
- Wasynczuk CV May 2018Document6 pagesWasynczuk CV May 2018api-403363741No ratings yet
- Slide Template HSE CTR Forum - JDCDocument20 pagesSlide Template HSE CTR Forum - JDCNebinsonNo ratings yet
- Meat or Wheat For The Next Millennium?: D. Joe MillwardDocument2 pagesMeat or Wheat For The Next Millennium?: D. Joe MillwardYago FerreiraNo ratings yet
- Noiseless PavementsDocument26 pagesNoiseless PavementsachsahNo ratings yet
- Evidence-Based Case Report: Kartiwa Hadi NuryantoDocument20 pagesEvidence-Based Case Report: Kartiwa Hadi NuryantohfathiardiNo ratings yet
- Ebs429 Assignment1Document1 pageEbs429 Assignment1NNadiah IsaNo ratings yet