
Circumcision
Circumcision
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Odors of Santity Distinctions of The Holy in Early Christianity and IslamDocument13 pagesOdors of Santity Distinctions of The Holy in Early Christianity and Islamkiedd_04100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Cell PhysiologyDocument61 pagesCell Physiologykiedd_04100% (4)
- Oral and Nasal Suctioning Procedure GuidelinesDocument4 pagesOral and Nasal Suctioning Procedure GuidelinesKimberly Ann Santos100% (1)
- Cephalocaudal Assessment (Cen)Document4 pagesCephalocaudal Assessment (Cen)Kristine Young100% (1)
- Notes On Blood BankingDocument99 pagesNotes On Blood Bankingapi-30646820490% (20)
- Iklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012Document2 pagesIklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012kiedd_04No ratings yet
- Fadhilat Surah at TakwirDocument1 pageFadhilat Surah at Takwirkiedd_04No ratings yet
- "Traditional" Exegeses of Q 4:34Document15 pages"Traditional" Exegeses of Q 4:34kiedd_04No ratings yet
- From The Bodies of Bees Classical and Christian Echoes in Surah Al-NahlDocument25 pagesFrom The Bodies of Bees Classical and Christian Echoes in Surah Al-Nahlkiedd_04No ratings yet
- Refleks ArcsDocument34 pagesRefleks Arcskiedd_04100% (1)
- The Place For Others in IslamDocument27 pagesThe Place For Others in Islamkiedd_04No ratings yet
- SYNAPSEDocument35 pagesSYNAPSEkiedd_04100% (3)
- Microbiology Colour Plate No.7Document1 pageMicrobiology Colour Plate No.7kiedd_04No ratings yet
- Microbiology Colour Plate No.8Document1 pageMicrobiology Colour Plate No.8kiedd_04No ratings yet
- Microbiology Colour Plate No.5Document1 pageMicrobiology Colour Plate No.5kiedd_04No ratings yet
- Microbiology Colour Plate No.9Document1 pageMicrobiology Colour Plate No.9kiedd_04No ratings yet
- Microbiology Colour Plate No.4Document1 pageMicrobiology Colour Plate No.4kiedd_04No ratings yet
- Microbiology Colour Plate No.6Document1 pageMicrobiology Colour Plate No.6kiedd_04No ratings yet
- Microbiology Colour Plate No.2Document1 pageMicrobiology Colour Plate No.2kiedd_04No ratings yet
- Microbiology Colour Plate No.3Document1 pageMicrobiology Colour Plate No.3kiedd_04No ratings yet
- API® CoryneDocument4 pagesAPI® Corynekiedd_04No ratings yet
- Microbiology Colour Plate No.1Document1 pageMicrobiology Colour Plate No.1kiedd_04No ratings yet
- Philosophical Consolation in Christianity and Islam Boethious and Al-KindiDocument10 pagesPhilosophical Consolation in Christianity and Islam Boethious and Al-Kindikiedd_04No ratings yet
- Mitigation of Climate ChangeDocument41 pagesMitigation of Climate Changekiedd_04No ratings yet
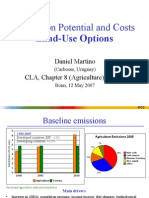
- Mitigation Potential and Costs Land-Use OptionsDocument9 pagesMitigation Potential and Costs Land-Use Optionskiedd_04No ratings yet
- Diagram of Classification of EnterobacteriaDocument1 pageDiagram of Classification of Enterobacteriakiedd_04100% (1)
- Carnitine DeficiencyDocument21 pagesCarnitine Deficiencykiedd_04100% (1)
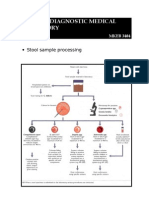
- Advance Diagnostic Medical Laboratory: The AP 20E® For Identification of BacteriaDocument1 pageAdvance Diagnostic Medical Laboratory: The AP 20E® For Identification of Bacteriakiedd_04100% (1)
- Mitigation of Climate ChangeDocument25 pagesMitigation of Climate Changekiedd_04No ratings yet
- Stool Sample ProcessingDocument1 pageStool Sample Processingkiedd_04No ratings yet
- Oxidase TestDocument1 pageOxidase Testkiedd_04100% (1)
- Introduction Basic GeneticsDocument6 pagesIntroduction Basic GeneticscsamarinaNo ratings yet
- Initial Assessment of The NeonateDocument27 pagesInitial Assessment of The NeonateRed WilliamsNo ratings yet
- Lecture Module #7: Articulation Part-II: Maureen Costello MS CCC/SLPDocument48 pagesLecture Module #7: Articulation Part-II: Maureen Costello MS CCC/SLPChristina DoughertyNo ratings yet
- Ovarian Cyst Treatment 1Document5 pagesOvarian Cyst Treatment 1Helcio FerreiraNo ratings yet
- Module 2 PPT NOTES HematopoiesisDocument8 pagesModule 2 PPT NOTES HematopoiesisMohammad MasacalNo ratings yet
- 04 CIN and Cervical Cancer UNEDITEDDocument120 pages04 CIN and Cervical Cancer UNEDITEDRalph JuicoNo ratings yet
- NHV Tripsy Supplement For Pets 100mlDocument1 pageNHV Tripsy Supplement For Pets 100mljjes86No ratings yet
- Group 4 c1 Abo IncompatibilityDocument64 pagesGroup 4 c1 Abo IncompatibilityAbhugz Marcelo100% (1)
- Jurnal Katak PDFDocument5 pagesJurnal Katak PDF31122007No ratings yet
- NBDE Dental Boards Oral Surgery-27Document27 pagesNBDE Dental Boards Oral Surgery-27amitdineshp100% (11)
- Ethiopia - GHSP - WP Narrative - 09 JuneDocument19 pagesEthiopia - GHSP - WP Narrative - 09 JuneNega TewoldeNo ratings yet
- Anatomy Practical Exam 2003Document7 pagesAnatomy Practical Exam 2003mohamedNo ratings yet
- Classification of MalocclusionDocument51 pagesClassification of MalocclusionYuvashreeNo ratings yet
- Indian National Biology Olympiad 2015Document50 pagesIndian National Biology Olympiad 2015Science Olympiad BlogNo ratings yet
- Word Part ReviewDocument6 pagesWord Part ReviewRanee ToNo ratings yet
- Presentation JaundiceDocument49 pagesPresentation JaundiceVinoth KumarNo ratings yet
- Austin AndrologyDocument4 pagesAustin AndrologyAustin Publishing GroupNo ratings yet
- Sialorrea PDFDocument6 pagesSialorrea PDFVerónica RuizNo ratings yet
- Hydroponic FourrageDocument12 pagesHydroponic FourrageSalman LabiadhNo ratings yet
- Marma Points of Ayurveda Vasant Lad.09673Document18 pagesMarma Points of Ayurveda Vasant Lad.09673prasadmvk50% (2)
- GalateaDocument21 pagesGalateaLexi RobertsNo ratings yet
- Chimaphila Pipsissewa Materia Medica HerbsDocument3 pagesChimaphila Pipsissewa Materia Medica HerbsAlejandra Guerrero100% (1)
- CFJ Anatomy Physiology PrimerDocument46 pagesCFJ Anatomy Physiology PrimerMarcelo MoralesNo ratings yet
- 1991 Bookmatter BiochemistryOfTheEyeDocument14 pages1991 Bookmatter BiochemistryOfTheEyeAndre C100% (1)
- Journal Reading: Hepatitis A: Epidemiology and Prevention in Developing CountriesDocument12 pagesJournal Reading: Hepatitis A: Epidemiology and Prevention in Developing CountriesDyah ArdaniNo ratings yet
- Respiratory SystemDocument4 pagesRespiratory SystemAlloiza CaguiclaNo ratings yet
- Krok 1 Anatomy 5Document1 pageKrok 1 Anatomy 5Sandeep KumarNo ratings yet

































































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Odors of Santity Distinctions of The Holy in Early Christianity and IslamDocument13 pagesOdors of Santity Distinctions of The Holy in Early Christianity and Islamkiedd_04100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Cell PhysiologyDocument61 pagesCell Physiologykiedd_04100% (4)
- Oral and Nasal Suctioning Procedure GuidelinesDocument4 pagesOral and Nasal Suctioning Procedure GuidelinesKimberly Ann Santos100% (1)
- Cephalocaudal Assessment (Cen)Document4 pagesCephalocaudal Assessment (Cen)Kristine Young100% (1)
- Notes On Blood BankingDocument99 pagesNotes On Blood Bankingapi-30646820490% (20)
- Iklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012Document2 pagesIklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012kiedd_04No ratings yet
- Fadhilat Surah at TakwirDocument1 pageFadhilat Surah at Takwirkiedd_04No ratings yet
- "Traditional" Exegeses of Q 4:34Document15 pages"Traditional" Exegeses of Q 4:34kiedd_04No ratings yet
- From The Bodies of Bees Classical and Christian Echoes in Surah Al-NahlDocument25 pagesFrom The Bodies of Bees Classical and Christian Echoes in Surah Al-Nahlkiedd_04No ratings yet
- Refleks ArcsDocument34 pagesRefleks Arcskiedd_04100% (1)
- The Place For Others in IslamDocument27 pagesThe Place For Others in Islamkiedd_04No ratings yet
- SYNAPSEDocument35 pagesSYNAPSEkiedd_04100% (3)
- Microbiology Colour Plate No.7Document1 pageMicrobiology Colour Plate No.7kiedd_04No ratings yet
- Microbiology Colour Plate No.8Document1 pageMicrobiology Colour Plate No.8kiedd_04No ratings yet
- Microbiology Colour Plate No.5Document1 pageMicrobiology Colour Plate No.5kiedd_04No ratings yet
- Microbiology Colour Plate No.9Document1 pageMicrobiology Colour Plate No.9kiedd_04No ratings yet
- Microbiology Colour Plate No.4Document1 pageMicrobiology Colour Plate No.4kiedd_04No ratings yet
- Microbiology Colour Plate No.6Document1 pageMicrobiology Colour Plate No.6kiedd_04No ratings yet
- Microbiology Colour Plate No.2Document1 pageMicrobiology Colour Plate No.2kiedd_04No ratings yet
- Microbiology Colour Plate No.3Document1 pageMicrobiology Colour Plate No.3kiedd_04No ratings yet
- API® CoryneDocument4 pagesAPI® Corynekiedd_04No ratings yet
- Microbiology Colour Plate No.1Document1 pageMicrobiology Colour Plate No.1kiedd_04No ratings yet
- Philosophical Consolation in Christianity and Islam Boethious and Al-KindiDocument10 pagesPhilosophical Consolation in Christianity and Islam Boethious and Al-Kindikiedd_04No ratings yet
- Mitigation of Climate ChangeDocument41 pagesMitigation of Climate Changekiedd_04No ratings yet
- Mitigation Potential and Costs Land-Use OptionsDocument9 pagesMitigation Potential and Costs Land-Use Optionskiedd_04No ratings yet
- Diagram of Classification of EnterobacteriaDocument1 pageDiagram of Classification of Enterobacteriakiedd_04100% (1)
- Carnitine DeficiencyDocument21 pagesCarnitine Deficiencykiedd_04100% (1)
- Advance Diagnostic Medical Laboratory: The AP 20E® For Identification of BacteriaDocument1 pageAdvance Diagnostic Medical Laboratory: The AP 20E® For Identification of Bacteriakiedd_04100% (1)
- Mitigation of Climate ChangeDocument25 pagesMitigation of Climate Changekiedd_04No ratings yet
- Stool Sample ProcessingDocument1 pageStool Sample Processingkiedd_04No ratings yet
- Oxidase TestDocument1 pageOxidase Testkiedd_04100% (1)
- Introduction Basic GeneticsDocument6 pagesIntroduction Basic GeneticscsamarinaNo ratings yet
- Initial Assessment of The NeonateDocument27 pagesInitial Assessment of The NeonateRed WilliamsNo ratings yet
- Lecture Module #7: Articulation Part-II: Maureen Costello MS CCC/SLPDocument48 pagesLecture Module #7: Articulation Part-II: Maureen Costello MS CCC/SLPChristina DoughertyNo ratings yet
- Ovarian Cyst Treatment 1Document5 pagesOvarian Cyst Treatment 1Helcio FerreiraNo ratings yet
- Module 2 PPT NOTES HematopoiesisDocument8 pagesModule 2 PPT NOTES HematopoiesisMohammad MasacalNo ratings yet
- 04 CIN and Cervical Cancer UNEDITEDDocument120 pages04 CIN and Cervical Cancer UNEDITEDRalph JuicoNo ratings yet
- NHV Tripsy Supplement For Pets 100mlDocument1 pageNHV Tripsy Supplement For Pets 100mljjes86No ratings yet
- Group 4 c1 Abo IncompatibilityDocument64 pagesGroup 4 c1 Abo IncompatibilityAbhugz Marcelo100% (1)
- Jurnal Katak PDFDocument5 pagesJurnal Katak PDF31122007No ratings yet
- NBDE Dental Boards Oral Surgery-27Document27 pagesNBDE Dental Boards Oral Surgery-27amitdineshp100% (11)
- Ethiopia - GHSP - WP Narrative - 09 JuneDocument19 pagesEthiopia - GHSP - WP Narrative - 09 JuneNega TewoldeNo ratings yet
- Anatomy Practical Exam 2003Document7 pagesAnatomy Practical Exam 2003mohamedNo ratings yet
- Classification of MalocclusionDocument51 pagesClassification of MalocclusionYuvashreeNo ratings yet
- Indian National Biology Olympiad 2015Document50 pagesIndian National Biology Olympiad 2015Science Olympiad BlogNo ratings yet
- Word Part ReviewDocument6 pagesWord Part ReviewRanee ToNo ratings yet
- Presentation JaundiceDocument49 pagesPresentation JaundiceVinoth KumarNo ratings yet
- Austin AndrologyDocument4 pagesAustin AndrologyAustin Publishing GroupNo ratings yet
- Sialorrea PDFDocument6 pagesSialorrea PDFVerónica RuizNo ratings yet
- Hydroponic FourrageDocument12 pagesHydroponic FourrageSalman LabiadhNo ratings yet
- Marma Points of Ayurveda Vasant Lad.09673Document18 pagesMarma Points of Ayurveda Vasant Lad.09673prasadmvk50% (2)
- GalateaDocument21 pagesGalateaLexi RobertsNo ratings yet
- Chimaphila Pipsissewa Materia Medica HerbsDocument3 pagesChimaphila Pipsissewa Materia Medica HerbsAlejandra Guerrero100% (1)
- CFJ Anatomy Physiology PrimerDocument46 pagesCFJ Anatomy Physiology PrimerMarcelo MoralesNo ratings yet
- 1991 Bookmatter BiochemistryOfTheEyeDocument14 pages1991 Bookmatter BiochemistryOfTheEyeAndre C100% (1)
- Journal Reading: Hepatitis A: Epidemiology and Prevention in Developing CountriesDocument12 pagesJournal Reading: Hepatitis A: Epidemiology and Prevention in Developing CountriesDyah ArdaniNo ratings yet
- Respiratory SystemDocument4 pagesRespiratory SystemAlloiza CaguiclaNo ratings yet
- Krok 1 Anatomy 5Document1 pageKrok 1 Anatomy 5Sandeep KumarNo ratings yet