
Medical Excuse Slip: (Doctor's Name) (Address) (City, State Zip Code) (Phone Number)
Medical Excuse Slip: (Doctor's Name) (Address) (City, State Zip Code) (Phone Number)
You might also like
- Fake Doctors Note Template For WorkDocument1 pageFake Doctors Note Template For WorkTimNo ratings yet
- Doctors NoteDocument1 pageDoctors NoteJeorme ChyNo ratings yet
- COVID-19 Doctor's NoteDocument1 pageCOVID-19 Doctor's NoteAndrew BarrNo ratings yet
- Free Printable Doctor's Note For Work: 274 Grant Lane Grand Rapids, MI 49503 Phone: 231-234-1587 Fax: 231-234-1588Document2 pagesFree Printable Doctor's Note For Work: 274 Grant Lane Grand Rapids, MI 49503 Phone: 231-234-1587 Fax: 231-234-1588Niya Norwood100% (1)
- Covid-19 Result Positive - Pitshou KafukuDocument2 pagesCovid-19 Result Positive - Pitshou KafukuKeller Brown JnrNo ratings yet
- Doctors Note Example For StudentDocument2 pagesDoctors Note Example For StudentHugo Castillo Gonzalez100% (1)
- Alejadro PCRDocument1 pageAlejadro PCRFirst Level Consulting SACNo ratings yet
- COVID TestDocument1 pageCOVID TestMalinda ShortNo ratings yet
- Proof of Employment Letter 06Document1 pageProof of Employment Letter 06Ali Nawaz0% (1)
- Doctors Note Template 12Document2 pagesDoctors Note Template 12rob radelNo ratings yet
- Medical Excuse NoteDocument1 pageMedical Excuse NoteRosalie Catalan EslabraNo ratings yet
- Doctors Note Template 01Document1 pageDoctors Note Template 01Karen MedinaNo ratings yet
- Doctors Note Excuse FormDocument1 pageDoctors Note Excuse FormJose A. Garcia TorresNo ratings yet
- 3514 Proof of Insurance Letter AutoDocument1 page3514 Proof of Insurance Letter AutoDerek HubbardNo ratings yet
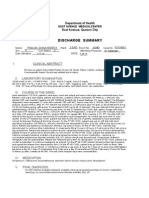
- Discharge Summary: I. Clinical AbstractDocument2 pagesDischarge Summary: I. Clinical AbstracttrialqwNo ratings yet
- Discharge SummaryDocument2 pagesDischarge SummaryRoshan LewisNo ratings yet
- Mark Property Tax ReceiptDocument2 pagesMark Property Tax Receiptpeterson greyNo ratings yet
- EligibilityResultsNotice 4Document11 pagesEligibilityResultsNotice 4Jeremy L. BellerNo ratings yet
- Doctors Notes 10 Good StuffDocument1 pageDoctors Notes 10 Good StuffRichard HindsNo ratings yet
- Ryan Doctor's NoteDocument2 pagesRyan Doctor's NoteCeleste KatzNo ratings yet
- Monetary Determination: Department of Labor and Human ResourcesDocument3 pagesMonetary Determination: Department of Labor and Human ResourcesBradley KirtsNo ratings yet
- r123123663 Elesha Casimir CUR123123663Document1 pager123123663 Elesha Casimir CUR123123663tefNo ratings yet
- Bonus Doctor Notes Template 03Document1 pageBonus Doctor Notes Template 03Charesa Reneé EvansNo ratings yet
- My Class ScheduleDocument1 pageMy Class ScheduleChaszmeque RachelNo ratings yet
- 201 East 4th Street, Suite 800 Cincinnati OH 45202 513.852.4899Document1 page201 East 4th Street, Suite 800 Cincinnati OH 45202 513.852.4899Tera's TarotNo ratings yet
- The Children's Clinic at NAM: Doctor Excuse FormDocument2 pagesThe Children's Clinic at NAM: Doctor Excuse FormRay AhmadNo ratings yet
- Sample Doctors Note Work SchoolDocument2 pagesSample Doctors Note Work SchoolNayeli VazquezNo ratings yet
- Doctors Note OutlineDocument2 pagesDoctors Note OutlineRoohid ParastNo ratings yet
- Real Doctors Note For WorkDocument1 pageReal Doctors Note For WorkAlaska JamesNo ratings yet
- Doctor Notes 01Document2 pagesDoctor Notes 01Richard HindsNo ratings yet
- Sample Doctors Note Work SchoolDocument2 pagesSample Doctors Note Work Schoolhector100% (1)
- Doctors Note Template 1Document2 pagesDoctors Note Template 1nipanipaNo ratings yet
- Doctor Dentist Note TemplateDocument2 pagesDoctor Dentist Note TemplateDënnïïŝ ÄłhëxändërNo ratings yet
- Jill Weber, DO: Illness InjuryDocument1 pageJill Weber, DO: Illness Injurynatalie goodjoinesNo ratings yet
- Adventist GlenOaks Hospital 8110116874Document4 pagesAdventist GlenOaks Hospital 8110116874Mark Richard Hilbert (Rossetti)No ratings yet
- Covid Test 3Document1 pageCovid Test 3Marius MateiNo ratings yet
- Pay Stub Template 2Document1 pagePay Stub Template 2Antwain UtleyNo ratings yet
- Doctors NoteDocument6 pagesDoctors Noteitgivesyouwings9No ratings yet
- Paystub Golden Limousine, Inc 20210906 20210919Document2 pagesPaystub Golden Limousine, Inc 20210906 20210919Alexander Weir-WitmerNo ratings yet
- RegistrationDocument2 pagesRegistrationJanene FergusonNo ratings yet
- Ryan Pay Stub 2Document1 pageRyan Pay Stub 2Ryan Baker100% (1)
- Discharge SummaryDocument2 pagesDischarge SummaryDeepak SharmaNo ratings yet
- Bonus Doctor Notes Template 02Document1 pageBonus Doctor Notes Template 02kimNo ratings yet
- Sample InsuranceDocument4 pagesSample InsuranceShashanth Kumar (CS - OMTP)No ratings yet
- Fay Bellas CK Stub 3Document1 pageFay Bellas CK Stub 3donerightsvcs100% (3)
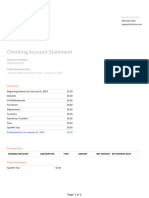
- Chime Checking Statement January 2024Document2 pagesChime Checking Statement January 2024fjpz6vfqktNo ratings yet
- PCR Usa PDFDocument1 pagePCR Usa PDFMA ReNo ratings yet
- 2016 Secured Tax Roll: Important MessagesDocument2 pages2016 Secured Tax Roll: Important Messagesabe lincolnNo ratings yet
- Lever Mcalilly LLC Paystubs 2015 06 30Document4 pagesLever Mcalilly LLC Paystubs 2015 06 30api-289189037No ratings yet
- Nieves 1Document1 pageNieves 1carterNo ratings yet
- Application For Housing Assistance: Use This Form To Apply For Social Housing Assistance in New South WalesDocument18 pagesApplication For Housing Assistance: Use This Form To Apply For Social Housing Assistance in New South WalesVincent HardyNo ratings yet
- Hs TranscriptDocument1 pageHs Transcriptapi-357468148No ratings yet
- Check Ais-3Document1 pageCheck Ais-3JOHNNo ratings yet
- 08 - 05 - 2021 Foods Off Cycle 119644 Supplemental PDFDocument1 page08 - 05 - 2021 Foods Off Cycle 119644 Supplemental PDFVictoria ChevalierNo ratings yet
- Homedepot PaystubDocument1 pageHomedepot PaystubGrantNo ratings yet
- Earnings Current YTD Amount Current Units YTD Units: Town of Guttenberg 6808 Park Avenue Guttenberg, NJ 07093Document1 pageEarnings Current YTD Amount Current Units YTD Units: Town of Guttenberg 6808 Park Avenue Guttenberg, NJ 07093Alfredo MurrugarraNo ratings yet
- TBJ New Patient Registration FormsDocument9 pagesTBJ New Patient Registration FormsSandra RíosNo ratings yet
- Ebook LettersDocument2 pagesEbook Lettersrizalputra1210No ratings yet
- Records Request Form - GenericDocument1 pageRecords Request Form - GenericCarrie AllenNo ratings yet


























































Download as pdf or txt
You might also like
- Fake Doctors Note Template For WorkDocument1 pageFake Doctors Note Template For WorkTimNo ratings yet
- Doctors NoteDocument1 pageDoctors NoteJeorme ChyNo ratings yet
- COVID-19 Doctor's NoteDocument1 pageCOVID-19 Doctor's NoteAndrew BarrNo ratings yet
- Free Printable Doctor's Note For Work: 274 Grant Lane Grand Rapids, MI 49503 Phone: 231-234-1587 Fax: 231-234-1588Document2 pagesFree Printable Doctor's Note For Work: 274 Grant Lane Grand Rapids, MI 49503 Phone: 231-234-1587 Fax: 231-234-1588Niya Norwood100% (1)
- Covid-19 Result Positive - Pitshou KafukuDocument2 pagesCovid-19 Result Positive - Pitshou KafukuKeller Brown JnrNo ratings yet
- Doctors Note Example For StudentDocument2 pagesDoctors Note Example For StudentHugo Castillo Gonzalez100% (1)
- Alejadro PCRDocument1 pageAlejadro PCRFirst Level Consulting SACNo ratings yet
- COVID TestDocument1 pageCOVID TestMalinda ShortNo ratings yet
- Proof of Employment Letter 06Document1 pageProof of Employment Letter 06Ali Nawaz0% (1)
- Doctors Note Template 12Document2 pagesDoctors Note Template 12rob radelNo ratings yet
- Medical Excuse NoteDocument1 pageMedical Excuse NoteRosalie Catalan EslabraNo ratings yet
- Doctors Note Template 01Document1 pageDoctors Note Template 01Karen MedinaNo ratings yet
- Doctors Note Excuse FormDocument1 pageDoctors Note Excuse FormJose A. Garcia TorresNo ratings yet
- 3514 Proof of Insurance Letter AutoDocument1 page3514 Proof of Insurance Letter AutoDerek HubbardNo ratings yet
- Discharge Summary: I. Clinical AbstractDocument2 pagesDischarge Summary: I. Clinical AbstracttrialqwNo ratings yet
- Discharge SummaryDocument2 pagesDischarge SummaryRoshan LewisNo ratings yet
- Mark Property Tax ReceiptDocument2 pagesMark Property Tax Receiptpeterson greyNo ratings yet
- EligibilityResultsNotice 4Document11 pagesEligibilityResultsNotice 4Jeremy L. BellerNo ratings yet
- Doctors Notes 10 Good StuffDocument1 pageDoctors Notes 10 Good StuffRichard HindsNo ratings yet
- Ryan Doctor's NoteDocument2 pagesRyan Doctor's NoteCeleste KatzNo ratings yet
- Monetary Determination: Department of Labor and Human ResourcesDocument3 pagesMonetary Determination: Department of Labor and Human ResourcesBradley KirtsNo ratings yet
- r123123663 Elesha Casimir CUR123123663Document1 pager123123663 Elesha Casimir CUR123123663tefNo ratings yet
- Bonus Doctor Notes Template 03Document1 pageBonus Doctor Notes Template 03Charesa Reneé EvansNo ratings yet
- My Class ScheduleDocument1 pageMy Class ScheduleChaszmeque RachelNo ratings yet
- 201 East 4th Street, Suite 800 Cincinnati OH 45202 513.852.4899Document1 page201 East 4th Street, Suite 800 Cincinnati OH 45202 513.852.4899Tera's TarotNo ratings yet
- The Children's Clinic at NAM: Doctor Excuse FormDocument2 pagesThe Children's Clinic at NAM: Doctor Excuse FormRay AhmadNo ratings yet
- Sample Doctors Note Work SchoolDocument2 pagesSample Doctors Note Work SchoolNayeli VazquezNo ratings yet
- Doctors Note OutlineDocument2 pagesDoctors Note OutlineRoohid ParastNo ratings yet
- Real Doctors Note For WorkDocument1 pageReal Doctors Note For WorkAlaska JamesNo ratings yet
- Doctor Notes 01Document2 pagesDoctor Notes 01Richard HindsNo ratings yet
- Sample Doctors Note Work SchoolDocument2 pagesSample Doctors Note Work Schoolhector100% (1)
- Doctors Note Template 1Document2 pagesDoctors Note Template 1nipanipaNo ratings yet
- Doctor Dentist Note TemplateDocument2 pagesDoctor Dentist Note TemplateDënnïïŝ ÄłhëxändërNo ratings yet
- Jill Weber, DO: Illness InjuryDocument1 pageJill Weber, DO: Illness Injurynatalie goodjoinesNo ratings yet
- Adventist GlenOaks Hospital 8110116874Document4 pagesAdventist GlenOaks Hospital 8110116874Mark Richard Hilbert (Rossetti)No ratings yet
- Covid Test 3Document1 pageCovid Test 3Marius MateiNo ratings yet
- Pay Stub Template 2Document1 pagePay Stub Template 2Antwain UtleyNo ratings yet
- Doctors NoteDocument6 pagesDoctors Noteitgivesyouwings9No ratings yet
- Paystub Golden Limousine, Inc 20210906 20210919Document2 pagesPaystub Golden Limousine, Inc 20210906 20210919Alexander Weir-WitmerNo ratings yet
- RegistrationDocument2 pagesRegistrationJanene FergusonNo ratings yet
- Ryan Pay Stub 2Document1 pageRyan Pay Stub 2Ryan Baker100% (1)
- Discharge SummaryDocument2 pagesDischarge SummaryDeepak SharmaNo ratings yet
- Bonus Doctor Notes Template 02Document1 pageBonus Doctor Notes Template 02kimNo ratings yet
- Sample InsuranceDocument4 pagesSample InsuranceShashanth Kumar (CS - OMTP)No ratings yet
- Fay Bellas CK Stub 3Document1 pageFay Bellas CK Stub 3donerightsvcs100% (3)
- Chime Checking Statement January 2024Document2 pagesChime Checking Statement January 2024fjpz6vfqktNo ratings yet
- PCR Usa PDFDocument1 pagePCR Usa PDFMA ReNo ratings yet
- 2016 Secured Tax Roll: Important MessagesDocument2 pages2016 Secured Tax Roll: Important Messagesabe lincolnNo ratings yet
- Lever Mcalilly LLC Paystubs 2015 06 30Document4 pagesLever Mcalilly LLC Paystubs 2015 06 30api-289189037No ratings yet
- Nieves 1Document1 pageNieves 1carterNo ratings yet
- Application For Housing Assistance: Use This Form To Apply For Social Housing Assistance in New South WalesDocument18 pagesApplication For Housing Assistance: Use This Form To Apply For Social Housing Assistance in New South WalesVincent HardyNo ratings yet
- Hs TranscriptDocument1 pageHs Transcriptapi-357468148No ratings yet
- Check Ais-3Document1 pageCheck Ais-3JOHNNo ratings yet
- 08 - 05 - 2021 Foods Off Cycle 119644 Supplemental PDFDocument1 page08 - 05 - 2021 Foods Off Cycle 119644 Supplemental PDFVictoria ChevalierNo ratings yet
- Homedepot PaystubDocument1 pageHomedepot PaystubGrantNo ratings yet
- Earnings Current YTD Amount Current Units YTD Units: Town of Guttenberg 6808 Park Avenue Guttenberg, NJ 07093Document1 pageEarnings Current YTD Amount Current Units YTD Units: Town of Guttenberg 6808 Park Avenue Guttenberg, NJ 07093Alfredo MurrugarraNo ratings yet
- TBJ New Patient Registration FormsDocument9 pagesTBJ New Patient Registration FormsSandra RíosNo ratings yet
- Ebook LettersDocument2 pagesEbook Lettersrizalputra1210No ratings yet
- Records Request Form - GenericDocument1 pageRecords Request Form - GenericCarrie AllenNo ratings yet