
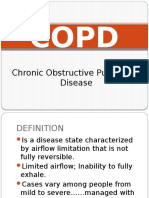
EMPHYSEMA
EMPHYSEMA
You might also like
- Renaissance Woman: Fat Loss, Muscle Growth & Performance Through Scientific EatingDocument20 pagesRenaissance Woman: Fat Loss, Muscle Growth & Performance Through Scientific EatingBenedict Ray Andhika33% (3)
- Obstructive Disease of Lung and Physiotherapy ManagementDocument76 pagesObstructive Disease of Lung and Physiotherapy Managementphysio43100% (1)
- List of Documents NBA PfilesDocument48 pagesList of Documents NBA PfilesDr. A. Pathanjali Sastri100% (1)
- Remembering, Bartlett (1932)Document11 pagesRemembering, Bartlett (1932)andreea4etc100% (1)
- Emphysema Is A LongDocument54 pagesEmphysema Is A LongryemoralesNo ratings yet
- CopdDocument4 pagesCopdapi-3739910100% (2)
- CR Patho SummaryDocument22 pagesCR Patho SummaryDNAANo ratings yet
- EmphysemaDocument27 pagesEmphysemaDiana Laura LeiNo ratings yet
- COPDDocument18 pagesCOPDMae CalicaNo ratings yet
- Emphysema Fall 2019Document3 pagesEmphysema Fall 2019Mary MarshNo ratings yet
- Asthma and The COPDsDocument133 pagesAsthma and The COPDsShania robertsNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument12 pagesChronic Obstructive Pulmonary Diseasejisoo100% (1)
- Chronic Obstructive Pulmonary DiseaseDocument10 pagesChronic Obstructive Pulmonary DiseaseZinya RobinsonNo ratings yet
- Emphysema A D A7Document13 pagesEmphysema A D A7Ahmed DsoukiNo ratings yet
- Textbuk DiscussionDocument5 pagesTextbuk Discussionapi-3717941No ratings yet
- Oxygenation NotesDocument23 pagesOxygenation NoteschikaycNo ratings yet
- Copd 200412082048Document139 pagesCopd 200412082048Richard ArceNo ratings yet
- EmphysemaDocument2 pagesEmphysemaapi-322389115No ratings yet
- Breathlessness EdittedDocument2 pagesBreathlessness EdittedSalwani MohamedNo ratings yet
- Resp Objectives Adn 253Document4 pagesResp Objectives Adn 253christian_zarate_2No ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument12 pagesChronic Obstructive Pulmonary DiseaseibegbunamchinemeremNo ratings yet
- Obstructive DisordersDocument23 pagesObstructive DisordersMartha ChaseNo ratings yet
- COPDDocument7 pagesCOPDarminmercado7406No ratings yet
- Patholpgic Change in EmphysemiaDocument16 pagesPatholpgic Change in Emphysemiafenil1194No ratings yet
- Onchi & CopdDocument8 pagesOnchi & CopdAngellene GraceNo ratings yet
- CopdDocument30 pagesCopdsalmanhabeebekNo ratings yet
- Normal Changes of AgingDocument9 pagesNormal Changes of AgingGiselle EstoquiaNo ratings yet
- Nursing Care Management - 112Document67 pagesNursing Care Management - 112Ong KarlNo ratings yet
- Copd CaseDocument36 pagesCopd Casejho_No ratings yet
- Dyspnea Is An Uncomfortable Abnormal Awareness of Breathing. A Number of DifferentDocument4 pagesDyspnea Is An Uncomfortable Abnormal Awareness of Breathing. A Number of DifferentSita SifanaNo ratings yet
- Pathophysiology of EmphysemaDocument3 pagesPathophysiology of EmphysemaApple Maiquez Garcia100% (1)
- Pathophysiology of COPD: Heart Failure Respiratory DisordersDocument5 pagesPathophysiology of COPD: Heart Failure Respiratory DisordersKath DeguzmanNo ratings yet
- The Respiratory SystemDocument8 pagesThe Respiratory SystemJane Rose SuperadaNo ratings yet
- NCLEX Review NotesDocument36 pagesNCLEX Review NotesKyla Patricia RibanoNo ratings yet
- Obstructive Airway DiseasesDocument56 pagesObstructive Airway Diseaseskalanakariyawasam99No ratings yet
- Respiratory SystemDocument85 pagesRespiratory SystemDr:-Ustaad Aakass Ahmed Junejo SahabNo ratings yet
- Case Study For EmphysemaDocument5 pagesCase Study For EmphysemaGabbii CincoNo ratings yet
- (Respi) Lo Week 2 Tutorial 1Document10 pages(Respi) Lo Week 2 Tutorial 1KintanNo ratings yet
- Oxygenation and Airway Management: Quick LookDocument24 pagesOxygenation and Airway Management: Quick LookNining Komala SariNo ratings yet
- Emphysema Chronic Obstructive Pulmonary Disease (COPD) : Call Dasco Today For More Information 855-442-7912Document6 pagesEmphysema Chronic Obstructive Pulmonary Disease (COPD) : Call Dasco Today For More Information 855-442-7912Nazif Aiman IsmailNo ratings yet
- Acute Respiratory Failure-PRINTDocument5 pagesAcute Respiratory Failure-PRINTJan SicatNo ratings yet
- Adult - RespiratoryDocument14 pagesAdult - RespiratoryahmeddorostyNo ratings yet
- Systems Plus College Foundation Macarthur Highway, Balibago, Angeles CityDocument13 pagesSystems Plus College Foundation Macarthur Highway, Balibago, Angeles CityLeanne Princess GamboaNo ratings yet
- Bronchial Obstruction: Presenter Andrea Fagan 3 Year Student NurseDocument27 pagesBronchial Obstruction: Presenter Andrea Fagan 3 Year Student NurseAndrea FaganNo ratings yet
- COPD Treatment and ManagementDocument3 pagesCOPD Treatment and ManagementHydie Mae AlcabedosNo ratings yet
- Patho Exam 3: Deficiency in Alpha-1-Antitrypsin-Unchecked Elastase Destruction of The AlveoliDocument5 pagesPatho Exam 3: Deficiency in Alpha-1-Antitrypsin-Unchecked Elastase Destruction of The AlveoliTaran LuthraNo ratings yet
- Reviewer For Management of Common IllnessDocument27 pagesReviewer For Management of Common Illnessmarie vennis hamchawanNo ratings yet
- Epidemiology: Several Diseases Airflow ObstructionDocument11 pagesEpidemiology: Several Diseases Airflow ObstructionBharat Singh BanshiwalNo ratings yet
- Dr. Kamran - S PBLDocument12 pagesDr. Kamran - S PBLTaimoor Ul HassanNo ratings yet
- CopdDocument60 pagesCopdRizqy Shofianingrum100% (1)
- COPDDocument30 pagesCOPDAmila SirisingheNo ratings yet
- Pulmonary PathologyDocument46 pagesPulmonary PathologyMuostafa KamelNo ratings yet
- Day 5 Respiratory DiseaseDocument71 pagesDay 5 Respiratory DiseaseRamzen Raphael DomingoNo ratings yet
- COPD & RLDDocument17 pagesCOPD & RLDhis.thunder122No ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument4 pagesChronic Obstructive Pulmonary DiseaseSeraphina SolanNo ratings yet
- LP Dyspnea RevisiDocument12 pagesLP Dyspnea RevisiInsaniNo ratings yet
- EmphysemaDocument3 pagesEmphysemaKhalid Mahmud ArifinNo ratings yet
- Essay EmphysemaDocument6 pagesEssay EmphysemaChristopher EstevezNo ratings yet
- DR Ambreen Shams NephrologistDocument58 pagesDR Ambreen Shams NephrologistAamer NaeemNo ratings yet
- Interstitial Lung DiseaseDocument14 pagesInterstitial Lung DiseaseAzkaZulfiqarNo ratings yet
- Physical Rehabilitation For Asthmatic PatientsDocument54 pagesPhysical Rehabilitation For Asthmatic PatientsIjeoma Okpalla60% (5)
- Atelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesFrom EverandAtelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesNo ratings yet
- The Entrepreneurial and Entrepreneurial Mind: Week #2Document20 pagesThe Entrepreneurial and Entrepreneurial Mind: Week #2Mr.BaiGNo ratings yet
- Logging Best Practices Guide PDFDocument12 pagesLogging Best Practices Guide PDFbnanduriNo ratings yet
- Karriem Provet,: Background of This CaseDocument11 pagesKarriem Provet,: Background of This CaseJustia.comNo ratings yet
- APPLICATION FOR REGISTRATION/ACCREDITATION AS AN ECOZONE SERVICE ENTERPRISE (For Customs Broker, Freight Forwarder/Trucker and Security Agency)Document7 pagesAPPLICATION FOR REGISTRATION/ACCREDITATION AS AN ECOZONE SERVICE ENTERPRISE (For Customs Broker, Freight Forwarder/Trucker and Security Agency)Albert YsegNo ratings yet
- Worksheet 1: The Terms of An AgreementDocument2 pagesWorksheet 1: The Terms of An AgreementJulieta ImbaquingoNo ratings yet
- Grade 2 - 1ST Periodical TestDocument5 pagesGrade 2 - 1ST Periodical TestGAY IBANEZ100% (1)
- Unusual Ways Usual DestinationDocument3 pagesUnusual Ways Usual DestinationLina Saad0% (1)
- LEARNING THEORIES Ausubel's Learning TheoryDocument17 pagesLEARNING THEORIES Ausubel's Learning TheoryCleoNo ratings yet
- International Law: Savarkar CaseDocument15 pagesInternational Law: Savarkar CaseArunesh Chandra100% (1)
- New Microsoft Office Word DocumentDocument12 pagesNew Microsoft Office Word DocumentRamana VaralaNo ratings yet
- Care of Terminally IllDocument34 pagesCare of Terminally Illbemina jaNo ratings yet
- State of The Handloom Industry of BangladeshDocument8 pagesState of The Handloom Industry of BangladeshNoshin NawarNo ratings yet
- SOPDocument3 pagesSOPShreya BonteNo ratings yet
- Invoice: Qrt. No - : Cc-15, Civil Township Rourkela, Dist - (Sundargarh (Odisha) - 769012 GSTIN - 21ACWFS2234G1Z4Document2 pagesInvoice: Qrt. No - : Cc-15, Civil Township Rourkela, Dist - (Sundargarh (Odisha) - 769012 GSTIN - 21ACWFS2234G1Z4PUNYASHLOK PANDANo ratings yet
- Greece Education Foundation Courses and Gces 10 2010Document6 pagesGreece Education Foundation Courses and Gces 10 2010Stamatios KarapournosNo ratings yet
- Pengkarya Muda - Aliah BiDocument7 pagesPengkarya Muda - Aliah BiNORHASLIZA BINTI MOHAMAD MoeNo ratings yet
- Data Sheets Ecc I On AdoraDocument23 pagesData Sheets Ecc I On AdoraAlanAvtoNo ratings yet
- Proposal (Objective Jpurpose Jscope)Document3 pagesProposal (Objective Jpurpose Jscope)Lee ChloeNo ratings yet
- Index: Monthly Bulletin-Dec 2022Document46 pagesIndex: Monthly Bulletin-Dec 2022Sanif KhanNo ratings yet
- If ملخص قواعدDocument2 pagesIf ملخص قواعدAhmed GaninyNo ratings yet
- English Curriculum Reforminthe PhilippinesDocument18 pagesEnglish Curriculum Reforminthe PhilippinesLanping FuNo ratings yet
- Stacey Dunlap ResumeDocument3 pagesStacey Dunlap ResumestaceysdunlapNo ratings yet
- M HealthDocument81 pagesM HealthAbebe ChekolNo ratings yet
- Babst Vs CA PDFDocument17 pagesBabst Vs CA PDFJustin YañezNo ratings yet
- Ie 2e Level 4 Unit 9-4Document4 pagesIe 2e Level 4 Unit 9-4Stasya EgorovaNo ratings yet
- Dual-Band Wearable Rectenna For Low-Power RF Energy HarvestingDocument10 pagesDual-Band Wearable Rectenna For Low-Power RF Energy HarvestingbabuNo ratings yet
- Referee Report TemplateDocument2 pagesReferee Report TemplateAna Jufriani100% (1)
























































































Download as docx, pdf, or txt
You might also like
- Renaissance Woman: Fat Loss, Muscle Growth & Performance Through Scientific EatingDocument20 pagesRenaissance Woman: Fat Loss, Muscle Growth & Performance Through Scientific EatingBenedict Ray Andhika33% (3)
- Obstructive Disease of Lung and Physiotherapy ManagementDocument76 pagesObstructive Disease of Lung and Physiotherapy Managementphysio43100% (1)
- List of Documents NBA PfilesDocument48 pagesList of Documents NBA PfilesDr. A. Pathanjali Sastri100% (1)
- Remembering, Bartlett (1932)Document11 pagesRemembering, Bartlett (1932)andreea4etc100% (1)
- Emphysema Is A LongDocument54 pagesEmphysema Is A LongryemoralesNo ratings yet
- CopdDocument4 pagesCopdapi-3739910100% (2)
- CR Patho SummaryDocument22 pagesCR Patho SummaryDNAANo ratings yet
- EmphysemaDocument27 pagesEmphysemaDiana Laura LeiNo ratings yet
- COPDDocument18 pagesCOPDMae CalicaNo ratings yet
- Emphysema Fall 2019Document3 pagesEmphysema Fall 2019Mary MarshNo ratings yet
- Asthma and The COPDsDocument133 pagesAsthma and The COPDsShania robertsNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument12 pagesChronic Obstructive Pulmonary Diseasejisoo100% (1)
- Chronic Obstructive Pulmonary DiseaseDocument10 pagesChronic Obstructive Pulmonary DiseaseZinya RobinsonNo ratings yet
- Emphysema A D A7Document13 pagesEmphysema A D A7Ahmed DsoukiNo ratings yet
- Textbuk DiscussionDocument5 pagesTextbuk Discussionapi-3717941No ratings yet
- Oxygenation NotesDocument23 pagesOxygenation NoteschikaycNo ratings yet
- Copd 200412082048Document139 pagesCopd 200412082048Richard ArceNo ratings yet
- EmphysemaDocument2 pagesEmphysemaapi-322389115No ratings yet
- Breathlessness EdittedDocument2 pagesBreathlessness EdittedSalwani MohamedNo ratings yet
- Resp Objectives Adn 253Document4 pagesResp Objectives Adn 253christian_zarate_2No ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument12 pagesChronic Obstructive Pulmonary DiseaseibegbunamchinemeremNo ratings yet
- Obstructive DisordersDocument23 pagesObstructive DisordersMartha ChaseNo ratings yet
- COPDDocument7 pagesCOPDarminmercado7406No ratings yet
- Patholpgic Change in EmphysemiaDocument16 pagesPatholpgic Change in Emphysemiafenil1194No ratings yet
- Onchi & CopdDocument8 pagesOnchi & CopdAngellene GraceNo ratings yet
- CopdDocument30 pagesCopdsalmanhabeebekNo ratings yet
- Normal Changes of AgingDocument9 pagesNormal Changes of AgingGiselle EstoquiaNo ratings yet
- Nursing Care Management - 112Document67 pagesNursing Care Management - 112Ong KarlNo ratings yet
- Copd CaseDocument36 pagesCopd Casejho_No ratings yet
- Dyspnea Is An Uncomfortable Abnormal Awareness of Breathing. A Number of DifferentDocument4 pagesDyspnea Is An Uncomfortable Abnormal Awareness of Breathing. A Number of DifferentSita SifanaNo ratings yet
- Pathophysiology of EmphysemaDocument3 pagesPathophysiology of EmphysemaApple Maiquez Garcia100% (1)
- Pathophysiology of COPD: Heart Failure Respiratory DisordersDocument5 pagesPathophysiology of COPD: Heart Failure Respiratory DisordersKath DeguzmanNo ratings yet
- The Respiratory SystemDocument8 pagesThe Respiratory SystemJane Rose SuperadaNo ratings yet
- NCLEX Review NotesDocument36 pagesNCLEX Review NotesKyla Patricia RibanoNo ratings yet
- Obstructive Airway DiseasesDocument56 pagesObstructive Airway Diseaseskalanakariyawasam99No ratings yet
- Respiratory SystemDocument85 pagesRespiratory SystemDr:-Ustaad Aakass Ahmed Junejo SahabNo ratings yet
- Case Study For EmphysemaDocument5 pagesCase Study For EmphysemaGabbii CincoNo ratings yet
- (Respi) Lo Week 2 Tutorial 1Document10 pages(Respi) Lo Week 2 Tutorial 1KintanNo ratings yet
- Oxygenation and Airway Management: Quick LookDocument24 pagesOxygenation and Airway Management: Quick LookNining Komala SariNo ratings yet
- Emphysema Chronic Obstructive Pulmonary Disease (COPD) : Call Dasco Today For More Information 855-442-7912Document6 pagesEmphysema Chronic Obstructive Pulmonary Disease (COPD) : Call Dasco Today For More Information 855-442-7912Nazif Aiman IsmailNo ratings yet
- Acute Respiratory Failure-PRINTDocument5 pagesAcute Respiratory Failure-PRINTJan SicatNo ratings yet
- Adult - RespiratoryDocument14 pagesAdult - RespiratoryahmeddorostyNo ratings yet
- Systems Plus College Foundation Macarthur Highway, Balibago, Angeles CityDocument13 pagesSystems Plus College Foundation Macarthur Highway, Balibago, Angeles CityLeanne Princess GamboaNo ratings yet
- Bronchial Obstruction: Presenter Andrea Fagan 3 Year Student NurseDocument27 pagesBronchial Obstruction: Presenter Andrea Fagan 3 Year Student NurseAndrea FaganNo ratings yet
- COPD Treatment and ManagementDocument3 pagesCOPD Treatment and ManagementHydie Mae AlcabedosNo ratings yet
- Patho Exam 3: Deficiency in Alpha-1-Antitrypsin-Unchecked Elastase Destruction of The AlveoliDocument5 pagesPatho Exam 3: Deficiency in Alpha-1-Antitrypsin-Unchecked Elastase Destruction of The AlveoliTaran LuthraNo ratings yet
- Reviewer For Management of Common IllnessDocument27 pagesReviewer For Management of Common Illnessmarie vennis hamchawanNo ratings yet
- Epidemiology: Several Diseases Airflow ObstructionDocument11 pagesEpidemiology: Several Diseases Airflow ObstructionBharat Singh BanshiwalNo ratings yet
- Dr. Kamran - S PBLDocument12 pagesDr. Kamran - S PBLTaimoor Ul HassanNo ratings yet
- CopdDocument60 pagesCopdRizqy Shofianingrum100% (1)
- COPDDocument30 pagesCOPDAmila SirisingheNo ratings yet
- Pulmonary PathologyDocument46 pagesPulmonary PathologyMuostafa KamelNo ratings yet
- Day 5 Respiratory DiseaseDocument71 pagesDay 5 Respiratory DiseaseRamzen Raphael DomingoNo ratings yet
- COPD & RLDDocument17 pagesCOPD & RLDhis.thunder122No ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument4 pagesChronic Obstructive Pulmonary DiseaseSeraphina SolanNo ratings yet
- LP Dyspnea RevisiDocument12 pagesLP Dyspnea RevisiInsaniNo ratings yet
- EmphysemaDocument3 pagesEmphysemaKhalid Mahmud ArifinNo ratings yet
- Essay EmphysemaDocument6 pagesEssay EmphysemaChristopher EstevezNo ratings yet
- DR Ambreen Shams NephrologistDocument58 pagesDR Ambreen Shams NephrologistAamer NaeemNo ratings yet
- Interstitial Lung DiseaseDocument14 pagesInterstitial Lung DiseaseAzkaZulfiqarNo ratings yet
- Physical Rehabilitation For Asthmatic PatientsDocument54 pagesPhysical Rehabilitation For Asthmatic PatientsIjeoma Okpalla60% (5)
- Atelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesFrom EverandAtelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesNo ratings yet
- The Entrepreneurial and Entrepreneurial Mind: Week #2Document20 pagesThe Entrepreneurial and Entrepreneurial Mind: Week #2Mr.BaiGNo ratings yet
- Logging Best Practices Guide PDFDocument12 pagesLogging Best Practices Guide PDFbnanduriNo ratings yet
- Karriem Provet,: Background of This CaseDocument11 pagesKarriem Provet,: Background of This CaseJustia.comNo ratings yet
- APPLICATION FOR REGISTRATION/ACCREDITATION AS AN ECOZONE SERVICE ENTERPRISE (For Customs Broker, Freight Forwarder/Trucker and Security Agency)Document7 pagesAPPLICATION FOR REGISTRATION/ACCREDITATION AS AN ECOZONE SERVICE ENTERPRISE (For Customs Broker, Freight Forwarder/Trucker and Security Agency)Albert YsegNo ratings yet
- Worksheet 1: The Terms of An AgreementDocument2 pagesWorksheet 1: The Terms of An AgreementJulieta ImbaquingoNo ratings yet
- Grade 2 - 1ST Periodical TestDocument5 pagesGrade 2 - 1ST Periodical TestGAY IBANEZ100% (1)
- Unusual Ways Usual DestinationDocument3 pagesUnusual Ways Usual DestinationLina Saad0% (1)
- LEARNING THEORIES Ausubel's Learning TheoryDocument17 pagesLEARNING THEORIES Ausubel's Learning TheoryCleoNo ratings yet
- International Law: Savarkar CaseDocument15 pagesInternational Law: Savarkar CaseArunesh Chandra100% (1)
- New Microsoft Office Word DocumentDocument12 pagesNew Microsoft Office Word DocumentRamana VaralaNo ratings yet
- Care of Terminally IllDocument34 pagesCare of Terminally Illbemina jaNo ratings yet
- State of The Handloom Industry of BangladeshDocument8 pagesState of The Handloom Industry of BangladeshNoshin NawarNo ratings yet
- SOPDocument3 pagesSOPShreya BonteNo ratings yet
- Invoice: Qrt. No - : Cc-15, Civil Township Rourkela, Dist - (Sundargarh (Odisha) - 769012 GSTIN - 21ACWFS2234G1Z4Document2 pagesInvoice: Qrt. No - : Cc-15, Civil Township Rourkela, Dist - (Sundargarh (Odisha) - 769012 GSTIN - 21ACWFS2234G1Z4PUNYASHLOK PANDANo ratings yet
- Greece Education Foundation Courses and Gces 10 2010Document6 pagesGreece Education Foundation Courses and Gces 10 2010Stamatios KarapournosNo ratings yet
- Pengkarya Muda - Aliah BiDocument7 pagesPengkarya Muda - Aliah BiNORHASLIZA BINTI MOHAMAD MoeNo ratings yet
- Data Sheets Ecc I On AdoraDocument23 pagesData Sheets Ecc I On AdoraAlanAvtoNo ratings yet
- Proposal (Objective Jpurpose Jscope)Document3 pagesProposal (Objective Jpurpose Jscope)Lee ChloeNo ratings yet
- Index: Monthly Bulletin-Dec 2022Document46 pagesIndex: Monthly Bulletin-Dec 2022Sanif KhanNo ratings yet
- If ملخص قواعدDocument2 pagesIf ملخص قواعدAhmed GaninyNo ratings yet
- English Curriculum Reforminthe PhilippinesDocument18 pagesEnglish Curriculum Reforminthe PhilippinesLanping FuNo ratings yet
- Stacey Dunlap ResumeDocument3 pagesStacey Dunlap ResumestaceysdunlapNo ratings yet
- M HealthDocument81 pagesM HealthAbebe ChekolNo ratings yet
- Babst Vs CA PDFDocument17 pagesBabst Vs CA PDFJustin YañezNo ratings yet
- Ie 2e Level 4 Unit 9-4Document4 pagesIe 2e Level 4 Unit 9-4Stasya EgorovaNo ratings yet
- Dual-Band Wearable Rectenna For Low-Power RF Energy HarvestingDocument10 pagesDual-Band Wearable Rectenna For Low-Power RF Energy HarvestingbabuNo ratings yet
- Referee Report TemplateDocument2 pagesReferee Report TemplateAna Jufriani100% (1)