Download as pdf or txt
You might also like
- Mercruiser Service Manual #14 Alpha I Gen II Outdrives 1991-NewerDocument715 pagesMercruiser Service Manual #14 Alpha I Gen II Outdrives 1991-NewerM5Melo100% (10)
- GplistDocument10 pagesGplistDean Fanning50% (2)
- Detailed Lesson Plan in TLE VIIDocument3 pagesDetailed Lesson Plan in TLE VIIJose Nilo Pastorall70% (10)
- Spotify Strategig Possining and Product Life Cycle Four Basic Stages.Document5 pagesSpotify Strategig Possining and Product Life Cycle Four Basic Stages.Jorge YeshayahuNo ratings yet
- The Current State of CoughDocument7 pagesThe Current State of CoughTatag PrimiawanNo ratings yet
- Diagnosis and Treatment of Chronic CoughFrom EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNo ratings yet
- CAP - PrinaDocument12 pagesCAP - PrinaSalNo ratings yet
- 2018 Article 50Document10 pages2018 Article 50miss betawiNo ratings yet
- Utility of The Sputum Cytology Applying MGG and Pap Stains in Monitoring Sudanese Patients Complaining of Bronchial AsthmaDocument6 pagesUtility of The Sputum Cytology Applying MGG and Pap Stains in Monitoring Sudanese Patients Complaining of Bronchial AsthmaDr. Asaad Mohammed Ahmed BabkerNo ratings yet
- Allergic Rhinitis and Chronic Suppurative Otitis Media: Archives of Oto-Rhino-Laryngology January 2011Document6 pagesAllergic Rhinitis and Chronic Suppurative Otitis Media: Archives of Oto-Rhino-Laryngology January 2011tiaNo ratings yet
- Comment: See Page E218Document2 pagesComment: See Page E218BBD BBDNo ratings yet
- Slide THTDocument15 pagesSlide THTmenthariNo ratings yet
- A Systematic Review On The Development of Asthma and Allergic Diseases in Relation To International Immigration: The Leading Role of The Environment ConfirmedDocument16 pagesA Systematic Review On The Development of Asthma and Allergic Diseases in Relation To International Immigration: The Leading Role of The Environment ConfirmedHow ToNo ratings yet
- Cap AsmaDocument10 pagesCap AsmaAuliaNo ratings yet
- E013796 FullDocument13 pagesE013796 FullRenny HusnulNo ratings yet
- The International Survey On The Management of Allergic Rhinitis by Physicians and Patients (Ismar)Document11 pagesThe International Survey On The Management of Allergic Rhinitis by Physicians and Patients (Ismar)danaagus81No ratings yet
- s12890 019 0946 ZDocument9 pagess12890 019 0946 ZABHINABA GUPTANo ratings yet
- Treatment Trends in Allergic Rhinitis and Asthma: A British ENT SurveyDocument5 pagesTreatment Trends in Allergic Rhinitis and Asthma: A British ENT SurveymenthariNo ratings yet
- The Aetiology and Antibiotic Management of Community-Acquired Pneumonia in Adults in Europe: A Literature ReviewDocument15 pagesThe Aetiology and Antibiotic Management of Community-Acquired Pneumonia in Adults in Europe: A Literature ReviewPutu Sukma RadhanaNo ratings yet
- Artificial Intelligence Techniques in Chronic Condition Lung DiseaseDocument14 pagesArtificial Intelligence Techniques in Chronic Condition Lung DiseaseNexgen TechnologyNo ratings yet
- Print 1Document8 pagesPrint 1Zaura Meliana MulyadiNo ratings yet
- Sputum Gram Stain For Diagnosing Causative Bacterial Pathogens and Guiding Antimicrobial Therapies in Community-Acquired Pneumonia: A Systematic Review and Meta-Analysis ProtocolDocument6 pagesSputum Gram Stain For Diagnosing Causative Bacterial Pathogens and Guiding Antimicrobial Therapies in Community-Acquired Pneumonia: A Systematic Review and Meta-Analysis ProtocolR2 Nursing '18No ratings yet
- CH 2Document17 pagesCH 2Kuleshwar SahuNo ratings yet
- Tuberculosis Recurrence After Completion Treatment in A European City - Reinfection or Relapse?Document8 pagesTuberculosis Recurrence After Completion Treatment in A European City - Reinfection or Relapse?tishaNo ratings yet
- Impact of Immunoglobulin E and Airway Obstruction On BronchiectasisDocument7 pagesImpact of Immunoglobulin E and Airway Obstruction On BronchiectasisRichie Irvanto CiandraNo ratings yet
- E013796 FullDocument12 pagesE013796 FullNabilatur rodiyahNo ratings yet
- Association Between Smoking Habit and Pulmonary Tuberculosis at Dr. Soetomo General Academic HospitalDocument5 pagesAssociation Between Smoking Habit and Pulmonary Tuberculosis at Dr. Soetomo General Academic HospitalairwanNo ratings yet
- Prediction of Post-Tuberculosis Lung Function ImpairmentDocument12 pagesPrediction of Post-Tuberculosis Lung Function ImpairmentputriargathyaNo ratings yet
- Epidemiological Risk Factors For Adult Dengue in Singapore: An 8-Year Nested Test Negative Case Control StudyDocument9 pagesEpidemiological Risk Factors For Adult Dengue in Singapore: An 8-Year Nested Test Negative Case Control StudydouwesdNo ratings yet
- QA, Module Module 2 Methods and Epidemiology of DiseasesDocument12 pagesQA, Module Module 2 Methods and Epidemiology of DiseasesPriyank LashkariNo ratings yet
- Impact of Self-Reported Gastroesophageal Reflux Disease in Subjects From Copdgene CohortDocument9 pagesImpact of Self-Reported Gastroesophageal Reflux Disease in Subjects From Copdgene CohortkasabeNo ratings yet
- Phytotherapy in Acute Bronchitis: What Is The Evidence?: Originalcontribution Open AccessDocument6 pagesPhytotherapy in Acute Bronchitis: What Is The Evidence?: Originalcontribution Open AccessShari' Si WahyuNo ratings yet
- Allergy - 2022 - Farraia - Allergen Immunotherapy For Asthma Prevention A Systematic Review and Meta Analysis ofDocument17 pagesAllergy - 2022 - Farraia - Allergen Immunotherapy For Asthma Prevention A Systematic Review and Meta Analysis ofpedrotiagosilvaNo ratings yet
- 1750 1164 8 3 PDFDocument7 pages1750 1164 8 3 PDFRiley RilanNo ratings yet
- I. Epidemiology and Genetics of AsthmaDocument7 pagesI. Epidemiology and Genetics of AsthmaVasincuAlexandruNo ratings yet
- ENg 101Document8 pagesENg 101BiniamNo ratings yet
- Copd 14 2219Document9 pagesCopd 14 2219Ruby FirdausNo ratings yet
- The Clinical Impact of Drug-Induced HepatotoxicityDocument9 pagesThe Clinical Impact of Drug-Induced HepatotoxicityDi LaNo ratings yet
- Common Cold and Acute Rhinosinusitis: Up-to-Date Management in 2020Document10 pagesCommon Cold and Acute Rhinosinusitis: Up-to-Date Management in 2020Shanaz KanandaNo ratings yet
- Content ServerDocument11 pagesContent ServerVerónica Duménez JofréNo ratings yet
- Management of Rhinosinusitis in Dutch General Practice: Society UKDocument15 pagesManagement of Rhinosinusitis in Dutch General Practice: Society UKMohamed Rikarz Ahamed RikarzNo ratings yet
- Enova ConventionDocument8 pagesEnova ConventionKazi Mazharul Islam ShajibNo ratings yet
- Acute Sinusitis and Sore Throat in Primary Care: Chris Del MarDocument3 pagesAcute Sinusitis and Sore Throat in Primary Care: Chris Del MarRhahima SyafrilNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument18 pagesChronic Obstructive Pulmonary DiseaseMaryam BajwaNo ratings yet
- Jurnal Widi GadarDocument5 pagesJurnal Widi GadarwidiaNo ratings yet
- Relationshipbetween Physical Conditionof House Environmentandthe Incidenceof Pulmonary Tuberculosis Aceh IndonesiaDocument5 pagesRelationshipbetween Physical Conditionof House Environmentandthe Incidenceof Pulmonary Tuberculosis Aceh IndonesiaLusyi AnnisaNo ratings yet
- Relationship Between Physical Condition of House Environment and The Incidence of Pulmonary Tuberculosis, Aceh, IndonesiaDocument5 pagesRelationship Between Physical Condition of House Environment and The Incidence of Pulmonary Tuberculosis, Aceh, IndonesiaFrans Yosep SitepuNo ratings yet
- PHD Thesis Samuel Coenen PDFDocument172 pagesPHD Thesis Samuel Coenen PDFsamuel_coenenNo ratings yet
- Literature Review of Pneumonia Under Five YearDocument6 pagesLiterature Review of Pneumonia Under Five Yeare9xy1xsv100% (1)
- Jurnal Respirology ASPRDocument55 pagesJurnal Respirology ASPRyosukexxNo ratings yet
- Infection Control & Hospital EpidemiologyDocument9 pagesInfection Control & Hospital EpidemiologyRianNo ratings yet
- SpringerDocument7 pagesSpringerEman SwaidanNo ratings yet
- Smoking Increases Risk of Recurrence After Successful Anti-Tuberculosis TreatmentDocument8 pagesSmoking Increases Risk of Recurrence After Successful Anti-Tuberculosis TreatmentRaditya Imam PratanaNo ratings yet
- Epidemiology of Asthma and in Uence of EthnicityDocument9 pagesEpidemiology of Asthma and in Uence of EthnicitySyahrialNo ratings yet
- Efficacy and Safety of Acupoint Autohemotherapy in PDFDocument5 pagesEfficacy and Safety of Acupoint Autohemotherapy in PDFtizziana carollaNo ratings yet
- tmp7CB6 TMPDocument3 pagestmp7CB6 TMPFrontiersNo ratings yet
- Mdi Technique On Ashtma PTDocument6 pagesMdi Technique On Ashtma PTNor Faizah Nurul AkmaNo ratings yet
- Sumber Faktor GenetikDocument10 pagesSumber Faktor GenetikKiociNo ratings yet
- BMI As A Risk Factor For The Development of Chronic Rhinosinusitis: A Prospective Population Based StudyDocument7 pagesBMI As A Risk Factor For The Development of Chronic Rhinosinusitis: A Prospective Population Based Studymudarisfaris1No ratings yet
- HCW Vs Adult Influenza IncidenceDocument9 pagesHCW Vs Adult Influenza Incidencereza_adrian_2No ratings yet
- KanervistoDocument7 pagesKanervistoDewi Aini ZulfahNo ratings yet
- Analysis of Age-Related Prevalence and Risk Factors of Chronic Rhinosinusitis With AsthmaDocument7 pagesAnalysis of Age-Related Prevalence and Risk Factors of Chronic Rhinosinusitis With AsthmaAnnisa Dhiya UlhaqNo ratings yet
- Effectiveness of 3 Generation Cephalosporin Compare To 3 Generation Cephalosporin - Macrolides For Community Acquired Pneumonia PatientsDocument10 pagesEffectiveness of 3 Generation Cephalosporin Compare To 3 Generation Cephalosporin - Macrolides For Community Acquired Pneumonia PatientslalaNo ratings yet
- Clinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareFrom EverandClinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareNo ratings yet
- Effect of Oral Cryotherapy in Preventing Chemotherapy Induced Oral Stomatitis Among Childhood Acute Lymphoblastic LeukemiaDocument10 pagesEffect of Oral Cryotherapy in Preventing Chemotherapy Induced Oral Stomatitis Among Childhood Acute Lymphoblastic LeukemiaIjahss JournalNo ratings yet
- Workbook For Developmental Communications 1 UNIT 6Document14 pagesWorkbook For Developmental Communications 1 UNIT 6soldadodeslealNo ratings yet
- Dance Like A ManDocument4 pagesDance Like A ManShubhadip aichNo ratings yet
- ASD PEDS Administration GuidelinesDocument5 pagesASD PEDS Administration GuidelinesInes Arias PazNo ratings yet
- Amyand's HerniaDocument5 pagesAmyand's HerniamonoarulNo ratings yet
- Ecosystem Services From Biodiversity To Society Part 2 1St Edition Bohan Full ChapterDocument67 pagesEcosystem Services From Biodiversity To Society Part 2 1St Edition Bohan Full Chapterharold.eychaner940100% (14)
- Collection of Windows 10 Hidden Secret Registry TweaksDocument9 pagesCollection of Windows 10 Hidden Secret Registry TweaksLiyoNo ratings yet
- Canastilla of Banana LlaneraDocument4 pagesCanastilla of Banana LlaneraValentina AcostaNo ratings yet
- The Dark Eye - Adv - One Death in GrangorDocument68 pagesThe Dark Eye - Adv - One Death in GrangorBo Poston100% (2)
- Annexure-10b) MA5620 & MA5626 Product Description PDFDocument52 pagesAnnexure-10b) MA5620 & MA5626 Product Description PDFFares DamNo ratings yet
- For StatDocument47 pagesFor StatLyn VeaNo ratings yet
- 5e Lesson Plan Format StemDocument7 pages5e Lesson Plan Format Stemapi-251803338No ratings yet
- Dial Plan Implementation: Introducing Call RoutingDocument180 pagesDial Plan Implementation: Introducing Call RoutingGuillermo Ex TottiNo ratings yet
- Pertemuan 2 - EXERCISES Entity Relationship ModelingDocument10 pagesPertemuan 2 - EXERCISES Entity Relationship Modelingjensen wangNo ratings yet
- Pemanfaatan Aplikasi Whatsapp Pada Pembelajaran Berbasis Masalah Untuk Mata Kuliah Akuntansi Internasional Di Universitas Pgri MadiunDocument13 pagesPemanfaatan Aplikasi Whatsapp Pada Pembelajaran Berbasis Masalah Untuk Mata Kuliah Akuntansi Internasional Di Universitas Pgri MadiunJurnal KwangsanNo ratings yet
- Invented EdensDocument201 pagesInvented EdensLeslie López100% (3)
- Brake Valves: Z279180 Z101197 Z289395 Z102626 (ZRL3518JC02)Document5 pagesBrake Valves: Z279180 Z101197 Z289395 Z102626 (ZRL3518JC02)houssem houssemNo ratings yet
- English Activity 1Document13 pagesEnglish Activity 1Mika ValenciaNo ratings yet
- Where Have All The Peasants Gone Susana NarotskyDocument21 pagesWhere Have All The Peasants Gone Susana NarotskyHoward Steven Rojas DivantoqueNo ratings yet
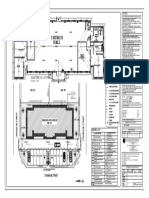
- Kakhisong Church A2-ModelDocument1 pageKakhisong Church A2-ModelanzaniNo ratings yet
- Answer: The Measure of The Central Angles of An Equilateral TriangleDocument4 pagesAnswer: The Measure of The Central Angles of An Equilateral Trianglesunil_ibmNo ratings yet
- The Future of Talent Management: Four Stages of Evolution: An Oracle White Paper June 2012Document19 pagesThe Future of Talent Management: Four Stages of Evolution: An Oracle White Paper June 2012aini amanNo ratings yet
- Entrepreneurial Lessons From The Bhagavad GitaDocument13 pagesEntrepreneurial Lessons From The Bhagavad GitaMahima FamousNo ratings yet
- Light Sport Aircraft: Standard Terminology ForDocument6 pagesLight Sport Aircraft: Standard Terminology ForAhmad Zubair RasulyNo ratings yet
- MSDS Gel Sanitizer 280720-01.es - enDocument11 pagesMSDS Gel Sanitizer 280720-01.es - enCristian GomezNo ratings yet
- Time Clauses - That Vs Which-Relative ClausesDocument8 pagesTime Clauses - That Vs Which-Relative ClausesZuza AlexandrinaNo ratings yet