
Surviving Sepsis Compaign: International Guidelines For Management of Sepsis and Septic Shock 2016
Surviving Sepsis Compaign: International Guidelines For Management of Sepsis and Septic Shock 2016
You might also like
- Pediatrics - Question Bank - RGUHSDocument51 pagesPediatrics - Question Bank - RGUHSArun Kumar88% (8)
- Topnotch Emergency Medicine For MoonlightersDocument129 pagesTopnotch Emergency Medicine For MoonlightersTEAM K 1920100% (1)
- Icu GuidebookDocument43 pagesIcu Guidebookdrimran570100% (5)
- MRCP Part 2 Written Exam Slides (Medicos Republic)Document530 pagesMRCP Part 2 Written Exam Slides (Medicos Republic)Fate ChanNo ratings yet
- Mini VET GuideDocument186 pagesMini VET GuideemitibiNo ratings yet
- Pediatric Advanced Life Support: I. PALS System Approach AlgorithmDocument19 pagesPediatric Advanced Life Support: I. PALS System Approach AlgorithmIsabel Castillo100% (1)
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- Medical MnemonicsDocument256 pagesMedical MnemonicssitalcoolkNo ratings yet
- Pediatric Assessment Triangle EditDocument31 pagesPediatric Assessment Triangle EditAlbert Gunawan100% (1)
- Surviving Sepsis Campaign: International Guidelines For Management of Sepsis and Septic Shock: 2016Document41 pagesSurviving Sepsis Campaign: International Guidelines For Management of Sepsis and Septic Shock: 2016Sarah OctavianiNo ratings yet
- Surviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedDocument32 pagesSurviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedAdli Wafi Jabbar100% (1)
- Surviving Sepsis Campaign 2016 Guidelines PresentationDocument30 pagesSurviving Sepsis Campaign 2016 Guidelines PresentationwisnusigitpratamaNo ratings yet
- Symposium 2. Detection and Management of Distributive Shock (DR Yunita Widyastuti SpAn)Document80 pagesSymposium 2. Detection and Management of Distributive Shock (DR Yunita Widyastuti SpAn)Rafela Agatha ChristyNo ratings yet
- Day 1 Biomedis UAP Sepsis - MontoyaDocument45 pagesDay 1 Biomedis UAP Sepsis - MontoyaRye CalderonNo ratings yet
- Sepsis and Septic Shock GuidelinesfinalDocument51 pagesSepsis and Septic Shock GuidelinesfinalElteyb Nor eldaimNo ratings yet
- Appendix 1: Recommendations and Best Practice StatementsDocument13 pagesAppendix 1: Recommendations and Best Practice StatementsWalter Manuel Yañez CamachoNo ratings yet
- Manejo Del Choque Séptico: Jesús Nicolás Hidalgo DelgadoDocument40 pagesManejo Del Choque Séptico: Jesús Nicolás Hidalgo DelgadoNicko HidalgoNo ratings yet
- Guideline For Septic Shock: AHMAD RAMADHAN (17777022)Document11 pagesGuideline For Septic Shock: AHMAD RAMADHAN (17777022)aby mayuNo ratings yet
- UntitledDocument21 pagesUntitledAg Paing PhyoNo ratings yet
- Harrison's Hour - Sepsis Bundle 2016Document5 pagesHarrison's Hour - Sepsis Bundle 2016Bobet Reña100% (1)
- Superviv Campaine Sepsis Shock Septico 2013Document12 pagesSuperviv Campaine Sepsis Shock Septico 2013LauraNo ratings yet
- International Guidelines For ManagementDocument24 pagesInternational Guidelines For ManagementSiti Novita KumanNo ratings yet
- Survivng Sepsis 2012 SummaryDocument34 pagesSurvivng Sepsis 2012 Summarygillian102290No ratings yet
- Tugas DR Yoma AncaDocument30 pagesTugas DR Yoma Ancaaby mayuNo ratings yet
- Surviving Sepsis GuidelinesDocument17 pagesSurviving Sepsis GuidelinesNabil RohaizatNo ratings yet
- Surviving Sepsis Campaign Bundle by ACTDocument58 pagesSurviving Sepsis Campaign Bundle by ACTchanthar4390No ratings yet
- International Guidelines For Management of Severe Sepsis and Septic ShockDocument8 pagesInternational Guidelines For Management of Severe Sepsis and Septic ShockFathoni AfifNo ratings yet
- TreatmentDocument55 pagesTreatmentderarataye6No ratings yet
- Management of SepsisDocument34 pagesManagement of SepsisTamim IshtiaqueNo ratings yet
- Sepsis: Nirav Mistry, MD and Adel Bassily-Marcus, MD, FCCP, FCCMDocument3 pagesSepsis: Nirav Mistry, MD and Adel Bassily-Marcus, MD, FCCP, FCCMAli AftabNo ratings yet
- SSC 2021 GuidelinesDocument59 pagesSSC 2021 GuidelinesPrasannakumar P CNo ratings yet
- Surviving Sepsis Campaign: International Guidelines For Management of Severe Sepsis and Septic Shock: 2016Document36 pagesSurviving Sepsis Campaign: International Guidelines For Management of Severe Sepsis and Septic Shock: 2016IvanRaykaNo ratings yet
- Initial Resuscitation and Infection IssuesDocument9 pagesInitial Resuscitation and Infection Issuesdanang bayuaji pratamaNo ratings yet
- Infeksi Bedah & Surviving Sepsis ChampaignDocument22 pagesInfeksi Bedah & Surviving Sepsis ChampaignHafiz AlfarizieNo ratings yet
- UGITherapyTsai Reg Training Day VersionDocument73 pagesUGITherapyTsai Reg Training Day Versionnhanchaoxin234No ratings yet
- Refractory Septic ShockDocument5 pagesRefractory Septic ShockBrian Antonio Veramatos LopezNo ratings yet
- Module 8 SepsisDocument44 pagesModule 8 SepsisEstefania Cuta HernandezNo ratings yet
- Groupcase PresentationDocument18 pagesGroupcase PresentationRiin IrasustaNo ratings yet
- Implement Poster (Surviving Sepsis Campaign)Document1 pageImplement Poster (Surviving Sepsis Campaign)agiev2000100% (1)
- Massive Blood Transfusion Protocols: Dr. N. Satyanarayana Dr. Shahzeb Zaman Dr. Juveria MahjabeenDocument46 pagesMassive Blood Transfusion Protocols: Dr. N. Satyanarayana Dr. Shahzeb Zaman Dr. Juveria MahjabeenshahzebzamanNo ratings yet
- Journal 2Document2 pagesJournal 2gythrieNo ratings yet
- Clinical Practice From Bench To Bedside - Is There A Great Divide by DR Marceliano T Aquino JRDocument25 pagesClinical Practice From Bench To Bedside - Is There A Great Divide by DR Marceliano T Aquino JRChristian ErelNo ratings yet
- Surviving Sepsis Campaign - NewDocument21 pagesSurviving Sepsis Campaign - NewIrfan SyakirNo ratings yet
- Management of Acute PancreatitisDocument31 pagesManagement of Acute PancreatitisLance sorianoNo ratings yet
- Severe Sepsis and Septic ShockDocument47 pagesSevere Sepsis and Septic Shocksembakarani thevagumaranNo ratings yet
- Warfarin Vs Rivaroxaban in APLSDocument26 pagesWarfarin Vs Rivaroxaban in APLSToheed AshrafNo ratings yet
- Hypertension in Dialysis PatientsDocument16 pagesHypertension in Dialysis PatientsSaad Anwar GujjarNo ratings yet
- 4 Phases of IV Fluid Therapy FinalDocument29 pages4 Phases of IV Fluid Therapy FinalLuqmanul Hakim Junaidden100% (1)
- Paper Telaah Jurnal Evidence Based Practice Keperawatan Kritis Dengan Judul Treatment of Patients With Severe Sepsis and Septic ShockDocument11 pagesPaper Telaah Jurnal Evidence Based Practice Keperawatan Kritis Dengan Judul Treatment of Patients With Severe Sepsis and Septic ShockTheresia AvilaNo ratings yet
- Anesthesia For Emergency AppendectomyDocument44 pagesAnesthesia For Emergency AppendectomyPrincess Lorenzo MiguelNo ratings yet
- Tumour Lysis Syndrome & Fe Brile Neutropenia: Supervisor: DR Asmidar Prepared By: Nizwan, Hajar, DorothyDocument38 pagesTumour Lysis Syndrome & Fe Brile Neutropenia: Supervisor: DR Asmidar Prepared By: Nizwan, Hajar, DorothyNizwan ShamNo ratings yet
- Syok - Anzak Akbar Andin PangeDocument34 pagesSyok - Anzak Akbar Andin PangeannisazakirohNo ratings yet
- Resusitasi Syok SepsisDocument23 pagesResusitasi Syok Sepsisfarisa14No ratings yet
- Management of Bleeding Peptic Ulcer: Alankar GuptaDocument72 pagesManagement of Bleeding Peptic Ulcer: Alankar Guptadalesantiago08No ratings yet
- HPB Adverse Transfusion ReactionDocument26 pagesHPB Adverse Transfusion ReactionFransiscus RivaldyNo ratings yet
- Diagnostics DiagnosticsDocument1 pageDiagnostics DiagnosticsAna Delia LabianoNo ratings yet
- Acute Pancreatitis: ManagementDocument11 pagesAcute Pancreatitis: ManagementKakhaNo ratings yet
- Habits Are Some of The Strategies RecommendedDocument30 pagesHabits Are Some of The Strategies Recommendedmd.dascalescu2486No ratings yet
- Current Recommendations For The Management of Severe Sepsis & Septic ShockDocument34 pagesCurrent Recommendations For The Management of Severe Sepsis & Septic ShockAmit KochetaNo ratings yet
- Jurnal 1 XDocument31 pagesJurnal 1 XFarilsah HakimNo ratings yet
- Kontras Dalam RadiologiDocument110 pagesKontras Dalam RadiologiKevin SNo ratings yet
- Sepsis and Rational Use of Rational Use of AntibioticDocument13 pagesSepsis and Rational Use of Rational Use of Antibioticvivien kate perixNo ratings yet
- Iv Fluids: SQN LDR Manoj Surg LT CDR Su Singh Maj IkjotDocument16 pagesIv Fluids: SQN LDR Manoj Surg LT CDR Su Singh Maj IkjotDebashish PaulNo ratings yet
- Sepsis Guidelines PocketDocument2 pagesSepsis Guidelines Pocket陳悅生No ratings yet
- DR. DR Umar Zein, SP - PD DTM&H - New Generation Antibiotic in SepsisDocument27 pagesDR. DR Umar Zein, SP - PD DTM&H - New Generation Antibiotic in SepsisOlivia DwimaswastiNo ratings yet
- Surviving Sepsis CampaignDocument15 pagesSurviving Sepsis CampaignsandhayaNo ratings yet
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYFrom EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYNo ratings yet
- Cardiovascular Exam (12 Minute) : Examiner - Student InteractionDocument6 pagesCardiovascular Exam (12 Minute) : Examiner - Student InteractionFate ChanNo ratings yet
- - المنقولة جنسياًDocument20 pages- المنقولة جنسياًFate ChanNo ratings yet
- General Writing Study MaterialsDocument1 pageGeneral Writing Study MaterialsFate ChanNo ratings yet
- Basic Concepts of Disease in PopulationsDocument60 pagesBasic Concepts of Disease in PopulationsFate ChanNo ratings yet
- CURRENT Diagnosis & Treatment: Nephrology & Hypertension, 2009 Chapter 46. Cystic Diseases of TH e KidneyDocument1 pageCURRENT Diagnosis & Treatment: Nephrology & Hypertension, 2009 Chapter 46. Cystic Diseases of TH e KidneyFate ChanNo ratings yet
- Sheet Abeer PDFDocument96 pagesSheet Abeer PDFFate ChanNo ratings yet
- Com&mis&cli&med&pad&1st PDFDocument294 pagesCom&mis&cli&med&pad&1st PDFJeevan Raj ShresthaNo ratings yet
- NAC OSCE - A Comprehensive Review 1E (2011)Document174 pagesNAC OSCE - A Comprehensive Review 1E (2011)D M Shawkot Hossain100% (2)
- Clinical Guideline For Vancomycin Prescribing and Therapeutic Drug MonitoringDocument11 pagesClinical Guideline For Vancomycin Prescribing and Therapeutic Drug MonitoringFate ChanNo ratings yet
- CalderMM Rounds Guide 2012Document17 pagesCalderMM Rounds Guide 2012Fate ChanNo ratings yet
- PCP in A Box - Module 1Document43 pagesPCP in A Box - Module 1Fate ChanNo ratings yet
- Cystic Diseases of The KidneyDocument65 pagesCystic Diseases of The KidneyFate ChanNo ratings yet
- 10 11648 J Ajim 20150303 13Document8 pages10 11648 J Ajim 20150303 13Fate ChanNo ratings yet
- Cystic Diseases of The Kidney. Renal NeoplasmsDocument31 pagesCystic Diseases of The Kidney. Renal NeoplasmsFate ChanNo ratings yet
- Adult Polycystic Kidney Disease: Gerald Schulman, MD, Fasn Vanderbilt University School of MedicineDocument58 pagesAdult Polycystic Kidney Disease: Gerald Schulman, MD, Fasn Vanderbilt University School of MedicineFate ChanNo ratings yet
- Choosing Low Glycemic Index Foods: W:/SCIM/Nutrition/Handouts/Heart Program/Glycemic IndexDocument4 pagesChoosing Low Glycemic Index Foods: W:/SCIM/Nutrition/Handouts/Heart Program/Glycemic IndexFate ChanNo ratings yet
- What Is The Glycemic Index of Food?Document2 pagesWhat Is The Glycemic Index of Food?Robert StevenNo ratings yet
- Cystic Diseases of The Kidney. Renal NeoplasmsDocument31 pagesCystic Diseases of The Kidney. Renal NeoplasmsFate ChanNo ratings yet
- Necrotizing Enterocolitis: Janice Nicklay Catalan M.DDocument27 pagesNecrotizing Enterocolitis: Janice Nicklay Catalan M.DrianurjanahNo ratings yet
- Emergency and Critical Care NursingDocument6 pagesEmergency and Critical Care NursingPINKY CUARESMANo ratings yet
- BTLS PENGKAJIAN KELAS MALEO GadarDocument24 pagesBTLS PENGKAJIAN KELAS MALEO GadarJecky CazorhaNo ratings yet
- Septic Shock: Ask The ExpertDocument4 pagesSeptic Shock: Ask The ExpertIvy Dianne PascualNo ratings yet
- Sepsis-Syok Septik 5-12-15Document36 pagesSepsis-Syok Septik 5-12-15Titi Nur IndrawatiNo ratings yet
- Pediatric EmergencyDocument98 pagesPediatric Emergencyian ismail100% (5)
- Ed Nutnicha E240002 - MergedDocument7 pagesEd Nutnicha E240002 - Mergedmaria arenas de itaNo ratings yet
- Haemodynamic MonitoringDocument128 pagesHaemodynamic MonitoringDr. KNo ratings yet
- PediatrictraumaDocument41 pagesPediatrictraumaPriyaNo ratings yet
- Critical CareDocument25 pagesCritical Carejassen karylle IbanezNo ratings yet
- Dengue: Who Guidelines For Diagnosis and Treatment: Jimmy Mendigo, MD Infectious Disease SpecialistDocument48 pagesDengue: Who Guidelines For Diagnosis and Treatment: Jimmy Mendigo, MD Infectious Disease Specialistkristianus yantoNo ratings yet
- Pre and Post Operative ManagementDocument3 pagesPre and Post Operative Managementdrsb54No ratings yet
- This Study Resource Was Shared ViaDocument6 pagesThis Study Resource Was Shared ViaMelinda Cariño BallonNo ratings yet
- Posttest UrinaryDocument7 pagesPosttest UrinaryAilatiLiamNo ratings yet
- (Surgery) 3.03 General Principles of Trauma - Dr. LicupDocument12 pages(Surgery) 3.03 General Principles of Trauma - Dr. LicupKim DeeNo ratings yet
- Surgery RemediationDocument14 pagesSurgery RemediationDrbee10No ratings yet
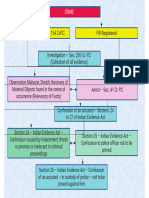
- Criminal Procedure Flow ChartDocument55 pagesCriminal Procedure Flow ChartsumeetppinNo ratings yet
- Burns - Fluid Volume, Risk For DeficientDocument3 pagesBurns - Fluid Volume, Risk For Deficientmakyofrancis20No ratings yet
- Septic Shock: Dr. Dr. Hori Hariyanto, Span, Kic, KMNDocument89 pagesSeptic Shock: Dr. Dr. Hori Hariyanto, Span, Kic, KMNPander MadonNo ratings yet
- Critical Care NursingDocument17 pagesCritical Care Nursingsanish4u100% (1)
- SirsDocument29 pagesSirsfatimaNo ratings yet
- ITLC Questions 2019Document9 pagesITLC Questions 2019Neil ThomasNo ratings yet
- (EXCELENT - Excelente) Survival Guide (AKA DOOM) 2.1 - Guia e Manual de Sobrevivência - A5Document311 pages(EXCELENT - Excelente) Survival Guide (AKA DOOM) 2.1 - Guia e Manual de Sobrevivência - A5jhongaNo ratings yet
- Protocol Final 2014 Last PDFDocument222 pagesProtocol Final 2014 Last PDFAbdelrahman MamdouhNo ratings yet










































































































Download as pdf or txt
You might also like
- Pediatrics - Question Bank - RGUHSDocument51 pagesPediatrics - Question Bank - RGUHSArun Kumar88% (8)
- Topnotch Emergency Medicine For MoonlightersDocument129 pagesTopnotch Emergency Medicine For MoonlightersTEAM K 1920100% (1)
- Icu GuidebookDocument43 pagesIcu Guidebookdrimran570100% (5)
- MRCP Part 2 Written Exam Slides (Medicos Republic)Document530 pagesMRCP Part 2 Written Exam Slides (Medicos Republic)Fate ChanNo ratings yet
- Mini VET GuideDocument186 pagesMini VET GuideemitibiNo ratings yet
- Pediatric Advanced Life Support: I. PALS System Approach AlgorithmDocument19 pagesPediatric Advanced Life Support: I. PALS System Approach AlgorithmIsabel Castillo100% (1)
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- Medical MnemonicsDocument256 pagesMedical MnemonicssitalcoolkNo ratings yet
- Pediatric Assessment Triangle EditDocument31 pagesPediatric Assessment Triangle EditAlbert Gunawan100% (1)
- Surviving Sepsis Campaign: International Guidelines For Management of Sepsis and Septic Shock: 2016Document41 pagesSurviving Sepsis Campaign: International Guidelines For Management of Sepsis and Septic Shock: 2016Sarah OctavianiNo ratings yet
- Surviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedDocument32 pagesSurviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedAdli Wafi Jabbar100% (1)
- Surviving Sepsis Campaign 2016 Guidelines PresentationDocument30 pagesSurviving Sepsis Campaign 2016 Guidelines PresentationwisnusigitpratamaNo ratings yet
- Symposium 2. Detection and Management of Distributive Shock (DR Yunita Widyastuti SpAn)Document80 pagesSymposium 2. Detection and Management of Distributive Shock (DR Yunita Widyastuti SpAn)Rafela Agatha ChristyNo ratings yet
- Day 1 Biomedis UAP Sepsis - MontoyaDocument45 pagesDay 1 Biomedis UAP Sepsis - MontoyaRye CalderonNo ratings yet
- Sepsis and Septic Shock GuidelinesfinalDocument51 pagesSepsis and Septic Shock GuidelinesfinalElteyb Nor eldaimNo ratings yet
- Appendix 1: Recommendations and Best Practice StatementsDocument13 pagesAppendix 1: Recommendations and Best Practice StatementsWalter Manuel Yañez CamachoNo ratings yet
- Manejo Del Choque Séptico: Jesús Nicolás Hidalgo DelgadoDocument40 pagesManejo Del Choque Séptico: Jesús Nicolás Hidalgo DelgadoNicko HidalgoNo ratings yet
- Guideline For Septic Shock: AHMAD RAMADHAN (17777022)Document11 pagesGuideline For Septic Shock: AHMAD RAMADHAN (17777022)aby mayuNo ratings yet
- UntitledDocument21 pagesUntitledAg Paing PhyoNo ratings yet
- Harrison's Hour - Sepsis Bundle 2016Document5 pagesHarrison's Hour - Sepsis Bundle 2016Bobet Reña100% (1)
- Superviv Campaine Sepsis Shock Septico 2013Document12 pagesSuperviv Campaine Sepsis Shock Septico 2013LauraNo ratings yet
- International Guidelines For ManagementDocument24 pagesInternational Guidelines For ManagementSiti Novita KumanNo ratings yet
- Survivng Sepsis 2012 SummaryDocument34 pagesSurvivng Sepsis 2012 Summarygillian102290No ratings yet
- Tugas DR Yoma AncaDocument30 pagesTugas DR Yoma Ancaaby mayuNo ratings yet
- Surviving Sepsis GuidelinesDocument17 pagesSurviving Sepsis GuidelinesNabil RohaizatNo ratings yet
- Surviving Sepsis Campaign Bundle by ACTDocument58 pagesSurviving Sepsis Campaign Bundle by ACTchanthar4390No ratings yet
- International Guidelines For Management of Severe Sepsis and Septic ShockDocument8 pagesInternational Guidelines For Management of Severe Sepsis and Septic ShockFathoni AfifNo ratings yet
- TreatmentDocument55 pagesTreatmentderarataye6No ratings yet
- Management of SepsisDocument34 pagesManagement of SepsisTamim IshtiaqueNo ratings yet
- Sepsis: Nirav Mistry, MD and Adel Bassily-Marcus, MD, FCCP, FCCMDocument3 pagesSepsis: Nirav Mistry, MD and Adel Bassily-Marcus, MD, FCCP, FCCMAli AftabNo ratings yet
- SSC 2021 GuidelinesDocument59 pagesSSC 2021 GuidelinesPrasannakumar P CNo ratings yet
- Surviving Sepsis Campaign: International Guidelines For Management of Severe Sepsis and Septic Shock: 2016Document36 pagesSurviving Sepsis Campaign: International Guidelines For Management of Severe Sepsis and Septic Shock: 2016IvanRaykaNo ratings yet
- Initial Resuscitation and Infection IssuesDocument9 pagesInitial Resuscitation and Infection Issuesdanang bayuaji pratamaNo ratings yet
- Infeksi Bedah & Surviving Sepsis ChampaignDocument22 pagesInfeksi Bedah & Surviving Sepsis ChampaignHafiz AlfarizieNo ratings yet
- UGITherapyTsai Reg Training Day VersionDocument73 pagesUGITherapyTsai Reg Training Day Versionnhanchaoxin234No ratings yet
- Refractory Septic ShockDocument5 pagesRefractory Septic ShockBrian Antonio Veramatos LopezNo ratings yet
- Module 8 SepsisDocument44 pagesModule 8 SepsisEstefania Cuta HernandezNo ratings yet
- Groupcase PresentationDocument18 pagesGroupcase PresentationRiin IrasustaNo ratings yet
- Implement Poster (Surviving Sepsis Campaign)Document1 pageImplement Poster (Surviving Sepsis Campaign)agiev2000100% (1)
- Massive Blood Transfusion Protocols: Dr. N. Satyanarayana Dr. Shahzeb Zaman Dr. Juveria MahjabeenDocument46 pagesMassive Blood Transfusion Protocols: Dr. N. Satyanarayana Dr. Shahzeb Zaman Dr. Juveria MahjabeenshahzebzamanNo ratings yet
- Journal 2Document2 pagesJournal 2gythrieNo ratings yet
- Clinical Practice From Bench To Bedside - Is There A Great Divide by DR Marceliano T Aquino JRDocument25 pagesClinical Practice From Bench To Bedside - Is There A Great Divide by DR Marceliano T Aquino JRChristian ErelNo ratings yet
- Surviving Sepsis Campaign - NewDocument21 pagesSurviving Sepsis Campaign - NewIrfan SyakirNo ratings yet
- Management of Acute PancreatitisDocument31 pagesManagement of Acute PancreatitisLance sorianoNo ratings yet
- Severe Sepsis and Septic ShockDocument47 pagesSevere Sepsis and Septic Shocksembakarani thevagumaranNo ratings yet
- Warfarin Vs Rivaroxaban in APLSDocument26 pagesWarfarin Vs Rivaroxaban in APLSToheed AshrafNo ratings yet
- Hypertension in Dialysis PatientsDocument16 pagesHypertension in Dialysis PatientsSaad Anwar GujjarNo ratings yet
- 4 Phases of IV Fluid Therapy FinalDocument29 pages4 Phases of IV Fluid Therapy FinalLuqmanul Hakim Junaidden100% (1)
- Paper Telaah Jurnal Evidence Based Practice Keperawatan Kritis Dengan Judul Treatment of Patients With Severe Sepsis and Septic ShockDocument11 pagesPaper Telaah Jurnal Evidence Based Practice Keperawatan Kritis Dengan Judul Treatment of Patients With Severe Sepsis and Septic ShockTheresia AvilaNo ratings yet
- Anesthesia For Emergency AppendectomyDocument44 pagesAnesthesia For Emergency AppendectomyPrincess Lorenzo MiguelNo ratings yet
- Tumour Lysis Syndrome & Fe Brile Neutropenia: Supervisor: DR Asmidar Prepared By: Nizwan, Hajar, DorothyDocument38 pagesTumour Lysis Syndrome & Fe Brile Neutropenia: Supervisor: DR Asmidar Prepared By: Nizwan, Hajar, DorothyNizwan ShamNo ratings yet
- Syok - Anzak Akbar Andin PangeDocument34 pagesSyok - Anzak Akbar Andin PangeannisazakirohNo ratings yet
- Resusitasi Syok SepsisDocument23 pagesResusitasi Syok Sepsisfarisa14No ratings yet
- Management of Bleeding Peptic Ulcer: Alankar GuptaDocument72 pagesManagement of Bleeding Peptic Ulcer: Alankar Guptadalesantiago08No ratings yet
- HPB Adverse Transfusion ReactionDocument26 pagesHPB Adverse Transfusion ReactionFransiscus RivaldyNo ratings yet
- Diagnostics DiagnosticsDocument1 pageDiagnostics DiagnosticsAna Delia LabianoNo ratings yet
- Acute Pancreatitis: ManagementDocument11 pagesAcute Pancreatitis: ManagementKakhaNo ratings yet
- Habits Are Some of The Strategies RecommendedDocument30 pagesHabits Are Some of The Strategies Recommendedmd.dascalescu2486No ratings yet
- Current Recommendations For The Management of Severe Sepsis & Septic ShockDocument34 pagesCurrent Recommendations For The Management of Severe Sepsis & Septic ShockAmit KochetaNo ratings yet
- Jurnal 1 XDocument31 pagesJurnal 1 XFarilsah HakimNo ratings yet
- Kontras Dalam RadiologiDocument110 pagesKontras Dalam RadiologiKevin SNo ratings yet
- Sepsis and Rational Use of Rational Use of AntibioticDocument13 pagesSepsis and Rational Use of Rational Use of Antibioticvivien kate perixNo ratings yet
- Iv Fluids: SQN LDR Manoj Surg LT CDR Su Singh Maj IkjotDocument16 pagesIv Fluids: SQN LDR Manoj Surg LT CDR Su Singh Maj IkjotDebashish PaulNo ratings yet
- Sepsis Guidelines PocketDocument2 pagesSepsis Guidelines Pocket陳悅生No ratings yet
- DR. DR Umar Zein, SP - PD DTM&H - New Generation Antibiotic in SepsisDocument27 pagesDR. DR Umar Zein, SP - PD DTM&H - New Generation Antibiotic in SepsisOlivia DwimaswastiNo ratings yet
- Surviving Sepsis CampaignDocument15 pagesSurviving Sepsis CampaignsandhayaNo ratings yet
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYFrom EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYNo ratings yet
- Cardiovascular Exam (12 Minute) : Examiner - Student InteractionDocument6 pagesCardiovascular Exam (12 Minute) : Examiner - Student InteractionFate ChanNo ratings yet
- - المنقولة جنسياًDocument20 pages- المنقولة جنسياًFate ChanNo ratings yet
- General Writing Study MaterialsDocument1 pageGeneral Writing Study MaterialsFate ChanNo ratings yet
- Basic Concepts of Disease in PopulationsDocument60 pagesBasic Concepts of Disease in PopulationsFate ChanNo ratings yet
- CURRENT Diagnosis & Treatment: Nephrology & Hypertension, 2009 Chapter 46. Cystic Diseases of TH e KidneyDocument1 pageCURRENT Diagnosis & Treatment: Nephrology & Hypertension, 2009 Chapter 46. Cystic Diseases of TH e KidneyFate ChanNo ratings yet
- Sheet Abeer PDFDocument96 pagesSheet Abeer PDFFate ChanNo ratings yet
- Com&mis&cli&med&pad&1st PDFDocument294 pagesCom&mis&cli&med&pad&1st PDFJeevan Raj ShresthaNo ratings yet
- NAC OSCE - A Comprehensive Review 1E (2011)Document174 pagesNAC OSCE - A Comprehensive Review 1E (2011)D M Shawkot Hossain100% (2)
- Clinical Guideline For Vancomycin Prescribing and Therapeutic Drug MonitoringDocument11 pagesClinical Guideline For Vancomycin Prescribing and Therapeutic Drug MonitoringFate ChanNo ratings yet
- CalderMM Rounds Guide 2012Document17 pagesCalderMM Rounds Guide 2012Fate ChanNo ratings yet
- PCP in A Box - Module 1Document43 pagesPCP in A Box - Module 1Fate ChanNo ratings yet
- Cystic Diseases of The KidneyDocument65 pagesCystic Diseases of The KidneyFate ChanNo ratings yet
- 10 11648 J Ajim 20150303 13Document8 pages10 11648 J Ajim 20150303 13Fate ChanNo ratings yet
- Cystic Diseases of The Kidney. Renal NeoplasmsDocument31 pagesCystic Diseases of The Kidney. Renal NeoplasmsFate ChanNo ratings yet
- Adult Polycystic Kidney Disease: Gerald Schulman, MD, Fasn Vanderbilt University School of MedicineDocument58 pagesAdult Polycystic Kidney Disease: Gerald Schulman, MD, Fasn Vanderbilt University School of MedicineFate ChanNo ratings yet
- Choosing Low Glycemic Index Foods: W:/SCIM/Nutrition/Handouts/Heart Program/Glycemic IndexDocument4 pagesChoosing Low Glycemic Index Foods: W:/SCIM/Nutrition/Handouts/Heart Program/Glycemic IndexFate ChanNo ratings yet
- What Is The Glycemic Index of Food?Document2 pagesWhat Is The Glycemic Index of Food?Robert StevenNo ratings yet
- Cystic Diseases of The Kidney. Renal NeoplasmsDocument31 pagesCystic Diseases of The Kidney. Renal NeoplasmsFate ChanNo ratings yet
- Necrotizing Enterocolitis: Janice Nicklay Catalan M.DDocument27 pagesNecrotizing Enterocolitis: Janice Nicklay Catalan M.DrianurjanahNo ratings yet
- Emergency and Critical Care NursingDocument6 pagesEmergency and Critical Care NursingPINKY CUARESMANo ratings yet
- BTLS PENGKAJIAN KELAS MALEO GadarDocument24 pagesBTLS PENGKAJIAN KELAS MALEO GadarJecky CazorhaNo ratings yet
- Septic Shock: Ask The ExpertDocument4 pagesSeptic Shock: Ask The ExpertIvy Dianne PascualNo ratings yet
- Sepsis-Syok Septik 5-12-15Document36 pagesSepsis-Syok Septik 5-12-15Titi Nur IndrawatiNo ratings yet
- Pediatric EmergencyDocument98 pagesPediatric Emergencyian ismail100% (5)
- Ed Nutnicha E240002 - MergedDocument7 pagesEd Nutnicha E240002 - Mergedmaria arenas de itaNo ratings yet
- Haemodynamic MonitoringDocument128 pagesHaemodynamic MonitoringDr. KNo ratings yet
- PediatrictraumaDocument41 pagesPediatrictraumaPriyaNo ratings yet
- Critical CareDocument25 pagesCritical Carejassen karylle IbanezNo ratings yet
- Dengue: Who Guidelines For Diagnosis and Treatment: Jimmy Mendigo, MD Infectious Disease SpecialistDocument48 pagesDengue: Who Guidelines For Diagnosis and Treatment: Jimmy Mendigo, MD Infectious Disease Specialistkristianus yantoNo ratings yet
- Pre and Post Operative ManagementDocument3 pagesPre and Post Operative Managementdrsb54No ratings yet
- This Study Resource Was Shared ViaDocument6 pagesThis Study Resource Was Shared ViaMelinda Cariño BallonNo ratings yet
- Posttest UrinaryDocument7 pagesPosttest UrinaryAilatiLiamNo ratings yet
- (Surgery) 3.03 General Principles of Trauma - Dr. LicupDocument12 pages(Surgery) 3.03 General Principles of Trauma - Dr. LicupKim DeeNo ratings yet
- Surgery RemediationDocument14 pagesSurgery RemediationDrbee10No ratings yet
- Criminal Procedure Flow ChartDocument55 pagesCriminal Procedure Flow ChartsumeetppinNo ratings yet
- Burns - Fluid Volume, Risk For DeficientDocument3 pagesBurns - Fluid Volume, Risk For Deficientmakyofrancis20No ratings yet
- Septic Shock: Dr. Dr. Hori Hariyanto, Span, Kic, KMNDocument89 pagesSeptic Shock: Dr. Dr. Hori Hariyanto, Span, Kic, KMNPander MadonNo ratings yet
- Critical Care NursingDocument17 pagesCritical Care Nursingsanish4u100% (1)
- SirsDocument29 pagesSirsfatimaNo ratings yet
- ITLC Questions 2019Document9 pagesITLC Questions 2019Neil ThomasNo ratings yet
- (EXCELENT - Excelente) Survival Guide (AKA DOOM) 2.1 - Guia e Manual de Sobrevivência - A5Document311 pages(EXCELENT - Excelente) Survival Guide (AKA DOOM) 2.1 - Guia e Manual de Sobrevivência - A5jhongaNo ratings yet
- Protocol Final 2014 Last PDFDocument222 pagesProtocol Final 2014 Last PDFAbdelrahman MamdouhNo ratings yet