Download as pdf or txt
You might also like
- Multiscale Dissociation Inventory (MDI)Document2 pagesMultiscale Dissociation Inventory (MDI)Gabriela Marc20% (5)
- The Central Mechanisms of Resistance Training and Its Effects On Cognitive FunctionDocument24 pagesThe Central Mechanisms of Resistance Training and Its Effects On Cognitive FunctionCarolina Ormaza GiraldoNo ratings yet
- 12 Jazz Patterns For Chromatic HarmonicaDocument5 pages12 Jazz Patterns For Chromatic HarmonicaGustavo Javier Caraballo PeñaNo ratings yet
- 2004 Mcclure PTDocument17 pages2004 Mcclure PTBruno FellipeNo ratings yet
- Rehabilitation in Spinal Cord InjuryDocument2 pagesRehabilitation in Spinal Cord InjuryAudry ArifinNo ratings yet
- Nandini KadabiDocument6 pagesNandini KadabiNandiniNo ratings yet
- The Impact of Whole Body Vibration Therapy On Spasticity and Disability of The Patients With Poststroke HemiplegiaDocument6 pagesThe Impact of Whole Body Vibration Therapy On Spasticity and Disability of The Patients With Poststroke HemiplegialabsoneducationNo ratings yet
- DONEDocument7 pagesDONEpashaNo ratings yet
- Annals of Medicine and SurgeryDocument4 pagesAnnals of Medicine and SurgeryRita SilvestreNo ratings yet
- 79b6 PDFDocument5 pages79b6 PDFcnsatishNo ratings yet
- To Compare The Effect of Core Stability Exercises and Muscle Energy Techniques On Low Back Pain PatientsDocument7 pagesTo Compare The Effect of Core Stability Exercises and Muscle Energy Techniques On Low Back Pain PatientsDr Ahmed NabilNo ratings yet
- Rehabilitation of The Ankle After Acute Sprain or Chronic Instability - PMCDocument1 pageRehabilitation of The Ankle After Acute Sprain or Chronic Instability - PMCkabirpandit1617No ratings yet
- Sullivan Et Al 2007 STEPS-CR 5Document23 pagesSullivan Et Al 2007 STEPS-CR 5Karen PohlNo ratings yet
- 2011-Khayambashi (1) 201201DD 023514Document8 pages2011-Khayambashi (1) 201201DD 023514Justine RamosNo ratings yet
- Rehabilitasi Post Op Spine Surgery: Kobal Sangaji Dokter Spesialis Rehabilitasi Medik RS Awalbros PekanbaruDocument27 pagesRehabilitasi Post Op Spine Surgery: Kobal Sangaji Dokter Spesialis Rehabilitasi Medik RS Awalbros PekanbarukurniaNo ratings yet
- Neuromuscular Training Improves Single-Limb Stability in Young Female AthletesDocument12 pagesNeuromuscular Training Improves Single-Limb Stability in Young Female AthletesyarnlarbizimdirNo ratings yet
- 10 1097TGR 0000000000000165Document10 pages10 1097TGR 0000000000000165cderosasNo ratings yet
- Schenkman: Exercise To Improve Spinal Flexibility and Function For People With Parkinson's Disease: A Randomized, Controlled TrialDocument10 pagesSchenkman: Exercise To Improve Spinal Flexibility and Function For People With Parkinson's Disease: A Randomized, Controlled TrialGerman BuyattiNo ratings yet
- The Effect of Spinal Exercises On H-Reflex in Subjects With Lumbosacral RadiculopathyDocument5 pagesThe Effect of Spinal Exercises On H-Reflex in Subjects With Lumbosacral RadiculopathyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1001Document12 pages1001Edo Orlando Galicia PinazoNo ratings yet
- Vikranth .G .R Lawrence Mathias Mohd Meraj Ghori: BackgroundDocument8 pagesVikranth .G .R Lawrence Mathias Mohd Meraj Ghori: BackgroundSekar AyuNo ratings yet
- Brainsci 11 00676 v2Document17 pagesBrainsci 11 00676 v2Rajender BishtNo ratings yet
- Comparison Gym Ball Breathing ExercisesDocument11 pagesComparison Gym Ball Breathing ExerciseseugloprecNo ratings yet
- Advances in Functional Electrical Stimulation For Lower Limb Rehabilitation Instroke: A Review On Physiologic and Therapeutic PerspectiveDocument6 pagesAdvances in Functional Electrical Stimulation For Lower Limb Rehabilitation Instroke: A Review On Physiologic and Therapeutic PerspectiveIJAR JOURNALNo ratings yet
- Contemporary Perspectives of Core StabilityDocument10 pagesContemporary Perspectives of Core StabilityRogério Bulhões CorvinoNo ratings yet
- Physical Education Ma KrishaDocument4 pagesPhysical Education Ma KrishaErica ShayeNo ratings yet
- Rehabilitation of The Ankle After Acute Sprain or Chronic InstabilityDocument17 pagesRehabilitation of The Ankle After Acute Sprain or Chronic InstabilityAndres Ignacio Lastra MillanNo ratings yet
- The Long-Term Effect of 2 PostoperativeDocument9 pagesThe Long-Term Effect of 2 Postoperativeahmed K.Abd el SaterNo ratings yet
- Core Keseimbangan DudukDocument6 pagesCore Keseimbangan DudukKadar KadarrrNo ratings yet
- The Effect of Early Progressive Resistive Exercise Therapy On Balance Control of Patients With Total Knee ArthroplastyDocument10 pagesThe Effect of Early Progressive Resistive Exercise Therapy On Balance Control of Patients With Total Knee ArthroplastyCarolina Drummond Rocha MoraisNo ratings yet
- To Explore The Effect of Exergames For Increasing The Ranges of The Shoulder Joint in Incomplete Spinal Cord Injury Patients: A Case StudyDocument5 pagesTo Explore The Effect of Exergames For Increasing The Ranges of The Shoulder Joint in Incomplete Spinal Cord Injury Patients: A Case StudyIJAR JOURNALNo ratings yet
- A Backward Walking Training Program To ImproveDocument10 pagesA Backward Walking Training Program To ImproveRadhiatul AdillahNo ratings yet
- Research in Sports Medicine: An International JournalDocument18 pagesResearch in Sports Medicine: An International JournalCleber PimentaNo ratings yet
- Effectiveness of Manual Perturbation Exercises inDocument7 pagesEffectiveness of Manual Perturbation Exercises inSabarie PNo ratings yet
- Intensive, Progressive Exercise Improves Quality of Life Following Lumbar Microdiskectomy: A Randomized Controlled TrialDocument10 pagesIntensive, Progressive Exercise Improves Quality of Life Following Lumbar Microdiskectomy: A Randomized Controlled TrialChloe DerrenbackerNo ratings yet
- Pilates RandomizadoDocument13 pagesPilates RandomizadorodrigueuresNo ratings yet
- Spenceretal 2016Document17 pagesSpenceretal 2016wladjaNo ratings yet
- Research Article Prevention of Physical Risk and Rehabilitation of Muscle Injury in Sanda CompetitionDocument9 pagesResearch Article Prevention of Physical Risk and Rehabilitation of Muscle Injury in Sanda Competition壮No ratings yet
- 72-Article Text-135-1-10-20190522 PDFDocument7 pages72-Article Text-135-1-10-20190522 PDFestherNo ratings yet
- Cugliari 2017Document11 pagesCugliari 2017Eduardo CastilloNo ratings yet
- 72-Article Text-135-1-10-20190522 PDFDocument7 pages72-Article Text-135-1-10-20190522 PDFestherNo ratings yet
- Effect of Lumbar Stabilization and Dynamic LumbarDocument9 pagesEffect of Lumbar Stabilization and Dynamic LumbarwladjaNo ratings yet
- Sandesh Rayamajhi Dipika Khanal Mallikarjunaiah H S: BackgroundDocument6 pagesSandesh Rayamajhi Dipika Khanal Mallikarjunaiah H S: BackgroundArdhyan ArdhyanNo ratings yet
- Anterior Knee PainDocument12 pagesAnterior Knee PainaaroncfisioNo ratings yet
- The Effect of Manual Therapy and Stabilizing Exercises On Forward Head and Rounded Shoulder Postures: A Six-Week Intervention With A One-Month Follow-Up StudyDocument8 pagesThe Effect of Manual Therapy and Stabilizing Exercises On Forward Head and Rounded Shoulder Postures: A Six-Week Intervention With A One-Month Follow-Up StudyAlef dos SantosNo ratings yet
- Exercise Therapy For Physical Therapist: Naruemon LeelayuwatDocument20 pagesExercise Therapy For Physical Therapist: Naruemon LeelayuwatAron NavarroNo ratings yet
- Core Stabilisation Training For Middleand Long-Distance RunnersDocument13 pagesCore Stabilisation Training For Middleand Long-Distance RunnersGonzalo Sebastian Bravo Rojas100% (2)
- PQ Art 47262-10Document6 pagesPQ Art 47262-10tayfunertebelNo ratings yet
- 0269215511423557Document10 pages0269215511423557Jose Maria DominguezNo ratings yet
- Asj 2020 0146Document6 pagesAsj 2020 0146Mandeep JangraNo ratings yet
- Psychological Predictors of Anterior Cruciate Ligament Reconstruction Outcomes: A Systematic ReviewDocument11 pagesPsychological Predictors of Anterior Cruciate Ligament Reconstruction Outcomes: A Systematic ReviewjavierNo ratings yet
- Relationship Between The Lower Quarter Y-Balance Test Scores and Isokinetic Strength Testing in Patients Status Post Acl ReconstructionDocument8 pagesRelationship Between The Lower Quarter Y-Balance Test Scores and Isokinetic Strength Testing in Patients Status Post Acl ReconstructionNovfran Adi ArtaNo ratings yet
- Adding Electrical Stimulation During Standard Rehabilitation After Stroke To Improve Motor Function. A Systematic Review and Meta-AnalysisDocument8 pagesAdding Electrical Stimulation During Standard Rehabilitation After Stroke To Improve Motor Function. A Systematic Review and Meta-AnalysisDiilNo ratings yet
- A Study of Core Muscle Electromyographic Activity During Physical ConditionsDocument7 pagesA Study of Core Muscle Electromyographic Activity During Physical ConditionsEsteban AmayaNo ratings yet
- Brain: Altering Spinal Cord Excitability Enables Voluntary Movements After Chronic Complete Paralysis in HumansDocument16 pagesBrain: Altering Spinal Cord Excitability Enables Voluntary Movements After Chronic Complete Paralysis in HumansSebastián GallegosNo ratings yet
- Back SquatDocument37 pagesBack SquatDusica DjordjevicNo ratings yet
- Kabat 4Document19 pagesKabat 4Nathalia Gutierrez RestrepoNo ratings yet
- Isokinetic Testing Why It Is More Important TodayDocument7 pagesIsokinetic Testing Why It Is More Important TodayChristina LushchynskaNo ratings yet
- Effect of Isokinetic Training On Strength, Functionality and Proprioception in Athletes With Functional Ankle InstabilityDocument11 pagesEffect of Isokinetic Training On Strength, Functionality and Proprioception in Athletes With Functional Ankle InstabilityJuan David Arenas MendozaNo ratings yet
- Extension LagDocument5 pagesExtension LagjeremyjlNo ratings yet
- IAP PaperDocument9 pagesIAP PaperGustavo Javier Caraballo PeñaNo ratings yet
- A Test Battery For Return To Play in FootballDocument11 pagesA Test Battery For Return To Play in FootballGustavo Javier Caraballo PeñaNo ratings yet
- Hui Jing 1999Document17 pagesHui Jing 1999Gustavo Javier Caraballo PeñaNo ratings yet
- Movement Exercises Study 2 - Essential Scales Support MaterialDocument2 pagesMovement Exercises Study 2 - Essential Scales Support MaterialGustavo Javier Caraballo PeñaNo ratings yet
- Please Support Our Guest Artists by Donating To Paypal - Me/harpinbytheseaDocument1 pagePlease Support Our Guest Artists by Donating To Paypal - Me/harpinbytheseaGustavo Javier Caraballo PeñaNo ratings yet
- Rapid Focused Neurological Assessment in The Emergency Department and ICUDocument16 pagesRapid Focused Neurological Assessment in The Emergency Department and ICUAnnie RicoNo ratings yet
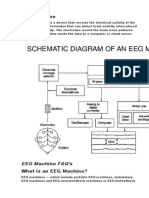
- EEG MachineDocument3 pagesEEG MachineOlea ScorpanNo ratings yet
- The Man and The Madness PDFDocument8 pagesThe Man and The Madness PDFJason JuliesNo ratings yet
- 13 Areas of Assessment 2DD PEDIADocument3 pages13 Areas of Assessment 2DD PEDIAChristiany Racho SalduaNo ratings yet
- Chapter 6. Touch, ProprioceptiDocument23 pagesChapter 6. Touch, ProprioceptisushantgandhiNo ratings yet
- Quick Stress ReliefDocument2 pagesQuick Stress ReliefKannanNo ratings yet
- Senses - WorksheetDocument3 pagesSenses - WorksheetRyan NegadNo ratings yet
- Neuroscience AssignmentDocument7 pagesNeuroscience AssignmentAubrey Unique EvangelistaNo ratings yet
- Alien Hand SyndromeDocument2 pagesAlien Hand SyndromeJhonnathan RodriguezNo ratings yet
- Stroke Dan Sepsis: Pembimbing: Dr. Bambang Supriadi, SP.SDocument24 pagesStroke Dan Sepsis: Pembimbing: Dr. Bambang Supriadi, SP.SIcha NathaliaNo ratings yet
- Diaphragm Sparing Brachial Plexus Blocks A.12Document7 pagesDiaphragm Sparing Brachial Plexus Blocks A.12FIA SlotNo ratings yet
- ML - Chapter 5 - Neural NetworkDocument64 pagesML - Chapter 5 - Neural NetworkYohannes DerejeNo ratings yet
- Types of Ques-McqDocument8 pagesTypes of Ques-Mcqsheetal taneja100% (2)
- Auditory PerceptionDocument9 pagesAuditory PerceptionFrancis Raymundo TabernillaNo ratings yet
- Hydrocephalus PresentationDocument49 pagesHydrocephalus PresentationSourina BeraNo ratings yet
- Educ-3 Chapter-3.1 TypesCharacteristicsIdentificationDocument34 pagesEduc-3 Chapter-3.1 TypesCharacteristicsIdentificationMYLE MANAYONNo ratings yet
- How Fear WorksDocument15 pagesHow Fear WorksIchsant Sopian100% (4)
- RPT SC Year 6 (DLP)Document28 pagesRPT SC Year 6 (DLP)Mariayee PerumalNo ratings yet
- 07 - Chapter 2 PDFDocument25 pages07 - Chapter 2 PDFGerick Dave Monencillo VenderNo ratings yet
- Daftar Pustaka: Ahmad B.2015. Gejala Non Motorik Penyakirt Parkinson. in Penyakit Parkinson DanDocument4 pagesDaftar Pustaka: Ahmad B.2015. Gejala Non Motorik Penyakirt Parkinson. in Penyakit Parkinson Danchica_asNo ratings yet
- Activity (Laboratory) No. 6 Special Senses: Fill in The Correct Terms Missing On Each StatementDocument9 pagesActivity (Laboratory) No. 6 Special Senses: Fill in The Correct Terms Missing On Each StatementPaulynne PaulynneNo ratings yet
- Psychology Cherryl Calades - Copy (Autosaved)Document184 pagesPsychology Cherryl Calades - Copy (Autosaved)carlo john balleta100% (1)
- Homeostasis and Feedback Loops AjarDocument34 pagesHomeostasis and Feedback Loops AjarPyrectic WilliamsNo ratings yet
- Biology ProjectDocument11 pagesBiology Projectshiv shankar100% (2)
- WHO List of Conditions Treated by Acupuncture - Healthy Family AcupunctureDocument3 pagesWHO List of Conditions Treated by Acupuncture - Healthy Family AcupunctureSreekanth KrishnamurthyNo ratings yet
- New Microsoft Word Document 1Document1 pageNew Microsoft Word Document 1api-385694647No ratings yet
- 2nd Group-Language DisordersDocument9 pages2nd Group-Language Disordersazizahikhsan09122002No ratings yet
- Impaired Urinary EliminationDocument2 pagesImpaired Urinary EliminationMatty-b AskalaniNo ratings yet
- Perception and Perceptual ProcessDocument17 pagesPerception and Perceptual ProcessDhrub Arka DekaNo ratings yet