Download as pdf or txt
You might also like
- Code Examples For dsPIC30F4011Document28 pagesCode Examples For dsPIC30F4011Minh VuNo ratings yet
- 1.2 Points, Lines, PlanesDocument24 pages1.2 Points, Lines, PlanesDeo Di Lyn100% (1)
- ChakraMoneyMeditation PDFDocument11 pagesChakraMoneyMeditation PDFΚωνσταντίνος Γιαμαλής100% (5)
- Katek HubunganDocument4 pagesKatek HubungankarinagitakNo ratings yet
- Archive of SID: Oral Cancer Knowledge Among Patients Referred To Mashhad Dental School, IranDocument6 pagesArchive of SID: Oral Cancer Knowledge Among Patients Referred To Mashhad Dental School, Iranhajer hNo ratings yet
- 1957-63 2.19 Wan Maria Nabillah GhaniDocument7 pages1957-63 2.19 Wan Maria Nabillah GhaniNursyafiq Ali ShibramulisiNo ratings yet
- Knowledge On Oral Cancer in A Group of Undergraduate Dentistry Students Conhecimento Sobre Câncer Oral em Um Grupo de Acadêmicos de OdontologiaDocument7 pagesKnowledge On Oral Cancer in A Group of Undergraduate Dentistry Students Conhecimento Sobre Câncer Oral em Um Grupo de Acadêmicos de OdontologiaGuilherme VinhandelliNo ratings yet
- 30.D18 788 Winny Yohana Indonesia-3-1Document4 pages30.D18 788 Winny Yohana Indonesia-3-1Yaumil FauziahNo ratings yet
- Wi Mar Dhani 2018Document8 pagesWi Mar Dhani 2018gabyNo ratings yet
- Clinico-Pathological Study of Oral CancersDocument4 pagesClinico-Pathological Study of Oral CancersIOSRjournalNo ratings yet
- Sangle Ameya Et AlDocument5 pagesSangle Ameya Et AlInternational Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- JCDR 9 XC05Document4 pagesJCDR 9 XC05hajer hNo ratings yet
- Oral Cancer Knowledge Among A Sample of Elderly People in Depok City, West Java, IndonesiaDocument9 pagesOral Cancer Knowledge Among A Sample of Elderly People in Depok City, West Java, IndonesiakarinagitakNo ratings yet
- NeuroQuantology Publication June 2022 Vol 20 Issue 6 AU Category B JournalDocument7 pagesNeuroQuantology Publication June 2022 Vol 20 Issue 6 AU Category B JournalNARESHNo ratings yet
- BrazilDocument7 pagesBrazilkarinagitakNo ratings yet
- Riginal Research: Journal of Advanced Medical and Dental Sciences ResearchDocument3 pagesRiginal Research: Journal of Advanced Medical and Dental Sciences Researchshivam sethiNo ratings yet
- Lesões Malignas - Med OralDocument8 pagesLesões Malignas - Med OralCaio GonçalvesNo ratings yet
- JIAP April 2019 - Prevalence of Severe Periodontitis in a Colombian Adult PopulationDocument10 pagesJIAP April 2019 - Prevalence of Severe Periodontitis in a Colombian Adult Populationaleja.b7815No ratings yet
- Assessing Oral Cancer Awareness Among Undergraduate Student in Higher Education Institution Using Multiple Linear RegressionDocument8 pagesAssessing Oral Cancer Awareness Among Undergraduate Student in Higher Education Institution Using Multiple Linear RegressionSteve GannabanNo ratings yet
- RUTKOSKI Et Al. (2017)Document8 pagesRUTKOSKI Et Al. (2017)Antonio CésarNo ratings yet
- RUTKOSKI Et Al. (2019)Document9 pagesRUTKOSKI Et Al. (2019)Antonio CésarNo ratings yet
- Profile and Survival of Tongue Cancer Patients in "Dharmais" Cancer Hospital, JakartaDocument5 pagesProfile and Survival of Tongue Cancer Patients in "Dharmais" Cancer Hospital, JakartaAlyani Akramah BasarNo ratings yet
- Prognostic JournalDocument6 pagesPrognostic JournalElpida WNo ratings yet
- TMJ 2016 0101Document7 pagesTMJ 2016 0101nadyaNo ratings yet
- Throat Cancer Psychosocial FactorsDocument8 pagesThroat Cancer Psychosocial FactorsPriyanka ParikhNo ratings yet
- JCT 2013102511342874Document8 pagesJCT 2013102511342874RiestaKierantiNo ratings yet
- Screening For Oral Cancer - Future Prospects, Research and Policy Development For AsiaDocument7 pagesScreening For Oral Cancer - Future Prospects, Research and Policy Development For AsiaCytha Nilam ChairaniNo ratings yet
- Risk Factors of Oral Cancer-A Hospital Based Case Control StudyDocument6 pagesRisk Factors of Oral Cancer-A Hospital Based Case Control StudyDevica DR PutriNo ratings yet
- Oral Cancer PDFDocument7 pagesOral Cancer PDFDaryAntoNo ratings yet
- Healthcare 11 01005 v2Document11 pagesHealthcare 11 01005 v2na huNo ratings yet
- Knowledge of Cancer Risk Factors, Symptoms, and Barriers To Seeking Medical Help Among Omani AdolescentsDocument12 pagesKnowledge of Cancer Risk Factors, Symptoms, and Barriers To Seeking Medical Help Among Omani AdolescentsAnak Agung Bagus WirayudaNo ratings yet
- Oral Cancer and Dentists: Knowledge, Attitudes and Practices in A South Colombian ContextDocument8 pagesOral Cancer and Dentists: Knowledge, Attitudes and Practices in A South Colombian Contexthajer hNo ratings yet
- Knowledge, Attitude and Practices of Students Enrolled in Health Related Courses at Saint Louis University Towards Human Papillomavirus (Philippines)Document8 pagesKnowledge, Attitude and Practices of Students Enrolled in Health Related Courses at Saint Louis University Towards Human Papillomavirus (Philippines)Alexander DeckerNo ratings yet
- JHeadNeckPhysiciansSurg4129-194289 052348Document6 pagesJHeadNeckPhysiciansSurg4129-194289 052348Javeria MNo ratings yet
- International Journal of Health Sciences and Research: ISSN: 2249-9571Document6 pagesInternational Journal of Health Sciences and Research: ISSN: 2249-9571GOUTAM MONDALNo ratings yet
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document8 pagesInternational Journal of Trend in Scientific Research and Development (IJTSRD)Research ParkNo ratings yet
- Awareness and Practice of Breast Cancer and Breast-Self Examination Among University Students in YemenDocument6 pagesAwareness and Practice of Breast Cancer and Breast-Self Examination Among University Students in YemenCaptain NarongNo ratings yet
- Application of Machine Learning For Diagnostic Prediction of Root CariesDocument10 pagesApplication of Machine Learning For Diagnostic Prediction of Root CariesHarisankar BNo ratings yet
- Oral Oncology: Adalberto Miranda-Filho, Freddie Bray TDocument8 pagesOral Oncology: Adalberto Miranda-Filho, Freddie Bray TAndressa A.No ratings yet
- Determinants of Cancer Screening Awareness and Participation Among Indonesian WomenDocument11 pagesDeterminants of Cancer Screening Awareness and Participation Among Indonesian WomenVilla Sekar citaNo ratings yet
- 2011 Article 195Document6 pages2011 Article 195Rashmeeta ThadhaniNo ratings yet
- Project Proposal Charera CPDocument27 pagesProject Proposal Charera CPClifford ChareraNo ratings yet
- Improvement of Oral Cancer Screening Quality and Reach: The Promise of Artificial IntelligenceDocument4 pagesImprovement of Oral Cancer Screening Quality and Reach: The Promise of Artificial IntelligenceHarisankar BNo ratings yet
- Early Diagnosis of Oral Cancer: TB, HH Y, Ü A, Ma A, MÇ A DYDocument13 pagesEarly Diagnosis of Oral Cancer: TB, HH Y, Ü A, Ma A, MÇ A DYAyimisaNo ratings yet
- Tobacco and Oral CancerDocument43 pagesTobacco and Oral CancerAl RawdhaNo ratings yet
- Jurnal 1Document8 pagesJurnal 1Anonymous Mi37eFiq4No ratings yet
- TSWJ2020 2146160Document8 pagesTSWJ2020 2146160William CorderoNo ratings yet
- Periodontal Diseases and Risk of Oral Cancer in Southern India: Results From The Hence Life StudyDocument8 pagesPeriodontal Diseases and Risk of Oral Cancer in Southern India: Results From The Hence Life Studyمحمد العراقيNo ratings yet
- Stunting and Soil-Transmitted-Helminth Infections Among School-Age Pupils in Rural Areas of Southern ChinaDocument6 pagesStunting and Soil-Transmitted-Helminth Infections Among School-Age Pupils in Rural Areas of Southern ChinaRohit GehiNo ratings yet
- 19-XD20 1266 Mranali K Shetty - IndiaDocument4 pages19-XD20 1266 Mranali K Shetty - IndiakhamilatusyNo ratings yet
- Artigo 1 ParacococcidiodomicoseDocument9 pagesArtigo 1 Paracococcidiodomicoseandre.jaccoud2No ratings yet
- The Intraoral and Extraoral Exam: Nancy W. Burkhart, BSDH, Med, Edd Leslie Delong, RDH, As, BSHS, MhaDocument29 pagesThe Intraoral and Extraoral Exam: Nancy W. Burkhart, BSDH, Med, Edd Leslie Delong, RDH, As, BSHS, Mhamuhammad nauvalNo ratings yet
- Chinese Dental Students' Knowledge and Attitudes Toward HIV/AIDSDocument7 pagesChinese Dental Students' Knowledge and Attitudes Toward HIV/AIDStamara tugasNo ratings yet
- Articol1 1Document12 pagesArticol1 1Smaranda GavrilNo ratings yet
- JB AdeoyeDocument12 pagesJB AdeoyeAdeoye JoshuaNo ratings yet
- Mikroba KankerDocument12 pagesMikroba KankerSilpi HamidiyahNo ratings yet
- 24 PrabaDocument9 pages24 PrabaAbdul GhofurNo ratings yet
- Prevalence of Self-Medication With Analgesics Among People Referring To Outpatient Dental Clinics in An Iranian PopulationDocument6 pagesPrevalence of Self-Medication With Analgesics Among People Referring To Outpatient Dental Clinics in An Iranian PopulationSofiaNo ratings yet
- APJCP Volume 16 Issue 18 Pages 8215-8220Document6 pagesAPJCP Volume 16 Issue 18 Pages 8215-8220A A Ngurah Wisnu Adiputra CNo ratings yet
- Artikel Ira Published 04042019Document5 pagesArtikel Ira Published 04042019cheatingw995No ratings yet
- UTS ARS105 - 20210309093 - Karisna AgustinDocument12 pagesUTS ARS105 - 20210309093 - Karisna AgustinsariputriutamiNo ratings yet
- Cancer Screening in the Developing World: Case Studies and Strategies from the FieldFrom EverandCancer Screening in the Developing World: Case Studies and Strategies from the FieldMadelon L. FinkelNo ratings yet
- Deha Tasarim KatalogDocument100 pagesDeha Tasarim KatalogEren ColakogluNo ratings yet
- Dokumen - Tips - 2016 11 22 A Complete Undergraduate Course Andrew M Steane Oxford JniversityDocument8 pagesDokumen - Tips - 2016 11 22 A Complete Undergraduate Course Andrew M Steane Oxford Jniversitykontakt.mfiedorowiczNo ratings yet
- ALTITUDE Presentation DeckDocument35 pagesALTITUDE Presentation DeckVikas ChaudharyNo ratings yet
- Instalacion de Kits de Aislamiento PIKOTEKDocument2 pagesInstalacion de Kits de Aislamiento PIKOTEKAlfonso Alberto ArguelloNo ratings yet
- Sin & Cos - The Programmer's PalsDocument24 pagesSin & Cos - The Programmer's PalsRicardo De Oliveira AlvesNo ratings yet
- Features: Ac DC Switching Power SupplyDocument1 pageFeatures: Ac DC Switching Power SupplyvernillaNo ratings yet
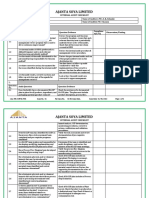
- Internal Audit Checklist Food Safety-MRDocument5 pagesInternal Audit Checklist Food Safety-MRRavi BaghelNo ratings yet
- Model Based Control Design: Alf IsakssonDocument17 pagesModel Based Control Design: Alf IsakssonSertug BaşarNo ratings yet
- Gardening Is Beneficial For Health: A Meta-AnalysisDocument8 pagesGardening Is Beneficial For Health: A Meta-AnalysisHaritha DeviNo ratings yet
- Ecg Machine Contec Type 1200gDocument3 pagesEcg Machine Contec Type 1200gFeliciaSetiawanNo ratings yet
- Heat Tracing Iso 2Document1 pageHeat Tracing Iso 2jsmnjasmines100% (1)
- Introduction of Africa and AsiaDocument9 pagesIntroduction of Africa and AsiaEllen Jane SilaNo ratings yet
- Tall Buildings and Its Structural SystemDocument54 pagesTall Buildings and Its Structural SystemPragya Roy83% (6)
- Compressed Air - 2 PDFDocument18 pagesCompressed Air - 2 PDFnuwaNo ratings yet
- Cooley, Charles - Social Organization. A Study of The Larger Mind (1909) (1910) PDFDocument458 pagesCooley, Charles - Social Organization. A Study of The Larger Mind (1909) (1910) PDFGermán Giupponi100% (1)
- The Lighting Cheat Sheet, by Andrew PriceDocument3 pagesThe Lighting Cheat Sheet, by Andrew PricekouzaNo ratings yet
- Star Delta Transformations: 1. Calculate The Total Resistance, R, of The Circuit BelowDocument11 pagesStar Delta Transformations: 1. Calculate The Total Resistance, R, of The Circuit BelowTina EllisonNo ratings yet
- L T Committee Opinion: Ist of ItlesDocument11 pagesL T Committee Opinion: Ist of ItlesnathanielNo ratings yet
- Forensicballistic Final-ExamDocument7 pagesForensicballistic Final-ExamJonel BallesterosNo ratings yet
- Clay & Shale Industries in OntarioDocument193 pagesClay & Shale Industries in OntarioJohn JohnsonNo ratings yet
- Topic 6 RECUERDOS DE FILIPINASDocument12 pagesTopic 6 RECUERDOS DE FILIPINASJan Arlyn JuanicoNo ratings yet
- Magb1 User Guide v1.1 EngDocument51 pagesMagb1 User Guide v1.1 EngPsu ChandasiriNo ratings yet
- Session - 2 Other Sources HintsDocument36 pagesSession - 2 Other Sources HintsJohn KAlespiNo ratings yet
- Engine Control Toyota Cuiser 2007 - 1GR - FeDocument6 pagesEngine Control Toyota Cuiser 2007 - 1GR - Fe35.Hoàng Xuân TânNo ratings yet
- Consumption of Functional Food and Our Health ConcernsDocument8 pagesConsumption of Functional Food and Our Health ConcernsPhysiology by Dr RaghuveerNo ratings yet
- AAS TroubleshootDocument30 pagesAAS TroubleshootKimi RinaNo ratings yet
- SIemens Air Damper ActuatorDocument40 pagesSIemens Air Damper ActuatorHENRYNo ratings yet