
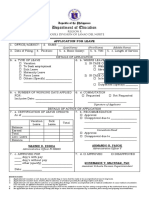
New Leave Form
New Leave Form
You might also like
- General Instruction Manual: Saudi Arabian Oil Company (Saudi Aramco) 710.014 Issuing Org. 3/01/2009 NEW Subject 1 OF 9Document9 pagesGeneral Instruction Manual: Saudi Arabian Oil Company (Saudi Aramco) 710.014 Issuing Org. 3/01/2009 NEW Subject 1 OF 9Delta akathehuskyNo ratings yet
- Factors Affecting Employee PerformanceDocument13 pagesFactors Affecting Employee PerformanceSara75% (4)
- Research ProposalDocument6 pagesResearch Proposalapi-322388206100% (1)
- Leave FormsDocument2 pagesLeave FormsRuffa Sabas AlferezNo ratings yet
- Application For Leave: Department of Education Region V Dividion of Camarines SurDocument2 pagesApplication For Leave: Department of Education Region V Dividion of Camarines Sursalve parfiles100% (1)
- CS Form No. 6 Revised 2020 Application For Leave FillableDocument2 pagesCS Form No. 6 Revised 2020 Application For Leave FillableXJ Bhevz OlsNo ratings yet
- Form 6Document3 pagesForm 6Eugelly Rivera100% (1)
- Application For Leave: CSC Form 6 District of Calumpit NorthDocument1 pageApplication For Leave: CSC Form 6 District of Calumpit NorthCrenz AcedillaNo ratings yet
- Cs Form No. 6 Application For Leave 2021 1 1Document1 pageCs Form No. 6 Application For Leave 2021 1 1mark jerald ritaNo ratings yet
- New Form 6 Leave Form TEACHERSDocument2 pagesNew Form 6 Leave Form TEACHERSmarites mercedNo ratings yet
- Application For Leave: Details of Action of ApplicationDocument7 pagesApplication For Leave: Details of Action of ApplicationJoanne Marie RoblesNo ratings yet
- Form 6 (Application For Leave)Document1 pageForm 6 (Application For Leave)Ccatherine Isanan-HilisanNo ratings yet
- Application For LeaveDocument2 pagesApplication For LeaveRAndy rodelasNo ratings yet
- Form 6 Revised 2020 RegionDocument5 pagesForm 6 Revised 2020 RegionLIEZEL BERSALESNo ratings yet
- Application For Leave: Cs Form 6Document2 pagesApplication For Leave: Cs Form 6Eduardo Jr PorrasNo ratings yet
- Form 6 NewDocument6 pagesForm 6 NewAnn Kempher Viernes NovalNo ratings yet
- Application For Leave (Form 6)Document1 pageApplication For Leave (Form 6)MARCELINA CABARINGNo ratings yet
- Application For Leave: Sardua Maria Calpiza Jauculan Assistant Regional Director Dilg R6 - OardDocument2 pagesApplication For Leave: Sardua Maria Calpiza Jauculan Assistant Regional Director Dilg R6 - OardDILG ConcepcionNo ratings yet
- CS Form No. 6 Revised 2020 Application For Leave FillableDocument3 pagesCS Form No. 6 Revised 2020 Application For Leave FillableFrenz Dela CruzNo ratings yet
- Department of Education: Application For LeaveDocument3 pagesDepartment of Education: Application For LeaveNicole Mo IINo ratings yet
- Leave Form For SH or Principal 1 Day 29 DaysDocument4 pagesLeave Form For SH or Principal 1 Day 29 Daysneri jadeNo ratings yet
- FORM6 DepEd CODEDDocument3 pagesFORM6 DepEd CODEDMaitem Stephanie GalosNo ratings yet
- CS Form No. 6 Revised 2020 Application For Leave FillableDocument2 pagesCS Form No. 6 Revised 2020 Application For Leave Fillablerhoda marimlaNo ratings yet
- Leave FormDocument1 pageLeave FormPrincess AmarahNo ratings yet
- Application For LeaveDocument2 pagesApplication For LeaveJinn Dalisay Uy100% (3)
- CSC Leave FormDocument2 pagesCSC Leave FormJosefina-RHUNo ratings yet
- New Format Form 6Document2 pagesNew Format Form 6rosette UngabNo ratings yet
- Department of Education: Application For LeaveDocument1 pageDepartment of Education: Application For LeavePatudan ESNo ratings yet
- Leave FormDocument2 pagesLeave FormMichaelle BunaoNo ratings yet
- Leave FormDocument1 pageLeave FormReffinej Abu de VillaNo ratings yet
- CS Form No. 6 Revised 2020 Application For Leave UpdatedDocument6 pagesCS Form No. 6 Revised 2020 Application For Leave Updatedpared1414No ratings yet
- CS Form No. 6 Revised 2020 Application For Leave Fillable 1 2Document4 pagesCS Form No. 6 Revised 2020 Application For Leave Fillable 1 2dyvejoytNo ratings yet
- Application For LeaveDocument10 pagesApplication For LeaveMary Ann AlmadinNo ratings yet
- Application For Leave: Department of EducationDocument10 pagesApplication For Leave: Department of EducationCHERRY UNANo ratings yet
- Application For Leave: 9 Days Below)Document3 pagesApplication For Leave: 9 Days Below)Nona Shella Diaz AbelgasNo ratings yet
- Application For Leave Ramos Raul Junio: Head Teacher I Catalino Castaneda ES / Bayambang IIDocument2 pagesApplication For Leave Ramos Raul Junio: Head Teacher I Catalino Castaneda ES / Bayambang IIraul ramosNo ratings yet
- NEW CS Form No. 6 Revised 2020 Application For Leave Fillable 1Document3 pagesNEW CS Form No. 6 Revised 2020 Application For Leave Fillable 1Reymart BorresNo ratings yet
- TEACHER CS Form No. 6 Revised 2020 Application For Leave Fillable 1 2020 Updated1Document2 pagesTEACHER CS Form No. 6 Revised 2020 Application For Leave Fillable 1 2020 Updated1Helen Joy Grijaldo JueleNo ratings yet
- CS Form No. 6 Revised 2020 Application For Leave Fillable 1Document4 pagesCS Form No. 6 Revised 2020 Application For Leave Fillable 1Gabriel De Los ReyesNo ratings yet
- CS Form No. 6 Revised 2020 More Than 60 DaysDocument1 pageCS Form No. 6 Revised 2020 More Than 60 DaysMa Ann Jubay Limbaga-BasaloNo ratings yet
- Leave Form CS Form No. 6 Revised 2020Document3 pagesLeave Form CS Form No. 6 Revised 2020Jeffree Lann AlvarezNo ratings yet
- Application For LeaveDocument2 pagesApplication For LeaveGeorge Blaire RasNo ratings yet
- CS Form No. 6 Revised 2023Document2 pagesCS Form No. 6 Revised 2023ANA CELLA MARZONo ratings yet
- CS Form No. 6 Revised 2020 2Document14 pagesCS Form No. 6 Revised 2020 2Geralyn GulaneNo ratings yet
- CS Form No. 6 Revised 2020 Application For LeaveDocument2 pagesCS Form No. 6 Revised 2020 Application For LeaveMara HeramizNo ratings yet
- Form-6 2023Document2 pagesForm-6 2023Chaselle PortesNo ratings yet
- BPS Form 6 Application For LeaveDocument2 pagesBPS Form 6 Application For LeaveAR IvleNo ratings yet
- Leave Form FORM 6 KARTDocument10 pagesLeave Form FORM 6 KARTPaaralan Ng PaclasanNo ratings yet
- Application For LeaveDocument2 pagesApplication For LeaveChristine Joy LozaresNo ratings yet
- Leave Form BLANKDocument1 pageLeave Form BLANKankarapeNo ratings yet
- Leave Form CS Form No. 6 Revised 2020Document4 pagesLeave Form CS Form No. 6 Revised 2020EdgarNo ratings yet
- Application For Leave: de Guzman Theresa Faye Aquino Adas Ii AccountingDocument2 pagesApplication For Leave: de Guzman Theresa Faye Aquino Adas Ii AccountingTheresa Faye De GuzmanNo ratings yet
- Form 6 1 NewDocument4 pagesForm 6 1 NewNiño PiornatoNo ratings yet
- Form 6 Leave Paper Revised 2021Document2 pagesForm 6 Leave Paper Revised 2021marites gallardoNo ratings yet
- CS Form No. 6 Revised 2020 Application For Leave Fillable 1Document4 pagesCS Form No. 6 Revised 2020 Application For Leave Fillable 1Joevan VillaflorNo ratings yet
- Department of Education: Application For LeaveDocument1 pageDepartment of Education: Application For LeaveRyan EnriquezNo ratings yet
- Out Patient (Specify)Document1 pageOut Patient (Specify)Toga MarMarNo ratings yet
- Form 6 NewDocument2 pagesForm 6 NewJenevey AlcoberNo ratings yet
- Leave FormDocument3 pagesLeave Formchito SarmientoNo ratings yet
- A. Application For Leave: CSC Form 6Document1 pageA. Application For Leave: CSC Form 6giareysieNo ratings yet
- CS Form No. 6, Revised 2020 (Application For Leave) (Fillable)Document2 pagesCS Form No. 6, Revised 2020 (Application For Leave) (Fillable)ArlanNo ratings yet
- Leave Form For SH or Principal (1 Day-60 Days)Document3 pagesLeave Form For SH or Principal (1 Day-60 Days)mark joseph quichoNo ratings yet
- Job Stress QuestionnaireDocument2 pagesJob Stress QuestionnaireMake Image RealNo ratings yet
- Would You Rather Be An Entrepreneur 2Document25 pagesWould You Rather Be An Entrepreneur 2Eduardo CanelaNo ratings yet
- Slord Development V NoyaDocument9 pagesSlord Development V NoyaJulius Edward GuzmanNo ratings yet
- Ranking Method of Performance AppraisalDocument6 pagesRanking Method of Performance AppraisalKyle annie100% (1)
- Article XiiiDocument21 pagesArticle XiiiJan Marlowe ArcoNo ratings yet
- Career Aspirations of GenerationzDocument4 pagesCareer Aspirations of Generationzvikas kunduNo ratings yet
- The Employment of Labour (Standing Orders) Act, 1965Document21 pagesThe Employment of Labour (Standing Orders) Act, 1965mrshaha2005No ratings yet
- Hudson The Case For Work Life BalanceDocument39 pagesHudson The Case For Work Life BalanceGABRIEL ELLISENo ratings yet
- ANNEX E Terminos y Condiciones Generales Contratos de Servicios UNICEFDocument14 pagesANNEX E Terminos y Condiciones Generales Contratos de Servicios UNICEFLuis Fernando Gomez suarezNo ratings yet
- Technical CorrespondenceDocument21 pagesTechnical Correspondenceirfan khosoNo ratings yet
- CHAPTER VI - Socio-Economic AspectDocument4 pagesCHAPTER VI - Socio-Economic AspectJun RecuerdoNo ratings yet
- Training and DevelopmentDocument12 pagesTraining and DevelopmentASNENo ratings yet
- Career Management - Meaning, Process and Objectives - Marketing91Document18 pagesCareer Management - Meaning, Process and Objectives - Marketing91AhlamNo ratings yet
- Headspace White Paper - Stress at Work - How Mindfulness Can HelpDocument8 pagesHeadspace White Paper - Stress at Work - How Mindfulness Can Helpsantiago macias0% (1)
- 1Document7 pages1Yak LeeNo ratings yet
- Employment Ordinance, Chapter 57 - Rest Days, Holidays and LeaveDocument0 pagesEmployment Ordinance, Chapter 57 - Rest Days, Holidays and Leavesasi_hkNo ratings yet
- CNA-Comelec CNADocument16 pagesCNA-Comelec CNApaomillan0423No ratings yet
- Seminar Primark Case StudyDocument7 pagesSeminar Primark Case StudyAdeline OtNo ratings yet
- 15 Dagasdas v. GrandplacementDocument12 pages15 Dagasdas v. GrandplacementClarissa SawaliNo ratings yet
- Basic Concepts and Principles of Construction Claims - Khuong Do BlogDocument12 pagesBasic Concepts and Principles of Construction Claims - Khuong Do BlogKhuong DoNo ratings yet
- Managing People and OrganizationDocument1 pageManaging People and OrganizationLea Mae NepuetoNo ratings yet
- KDSDocument69 pagesKDSTehsin Zaman67% (6)
- M6931 Legal Services in Australia Industry ReportDocument32 pagesM6931 Legal Services in Australia Industry ReportAnge OuNo ratings yet
- 35 Paquette V Amaruk Wilderness and Another No 4 2016 BCHRT 35Document28 pages35 Paquette V Amaruk Wilderness and Another No 4 2016 BCHRT 35The Vancouver SunNo ratings yet
- Session1 (1) JuanaDocument2 pagesSession1 (1) JuanaKammla MirandaNo ratings yet
- UiPath-Future of Work TLPDocument16 pagesUiPath-Future of Work TLPAbdoul Quang CuongNo ratings yet
- 2-RFP-18-006 FY2018 Tree Planting Project PDFDocument74 pages2-RFP-18-006 FY2018 Tree Planting Project PDFMarc BosiNo ratings yet























































































Download as docx, pdf, or txt
You might also like
- General Instruction Manual: Saudi Arabian Oil Company (Saudi Aramco) 710.014 Issuing Org. 3/01/2009 NEW Subject 1 OF 9Document9 pagesGeneral Instruction Manual: Saudi Arabian Oil Company (Saudi Aramco) 710.014 Issuing Org. 3/01/2009 NEW Subject 1 OF 9Delta akathehuskyNo ratings yet
- Factors Affecting Employee PerformanceDocument13 pagesFactors Affecting Employee PerformanceSara75% (4)
- Research ProposalDocument6 pagesResearch Proposalapi-322388206100% (1)
- Leave FormsDocument2 pagesLeave FormsRuffa Sabas AlferezNo ratings yet
- Application For Leave: Department of Education Region V Dividion of Camarines SurDocument2 pagesApplication For Leave: Department of Education Region V Dividion of Camarines Sursalve parfiles100% (1)
- CS Form No. 6 Revised 2020 Application For Leave FillableDocument2 pagesCS Form No. 6 Revised 2020 Application For Leave FillableXJ Bhevz OlsNo ratings yet
- Form 6Document3 pagesForm 6Eugelly Rivera100% (1)
- Application For Leave: CSC Form 6 District of Calumpit NorthDocument1 pageApplication For Leave: CSC Form 6 District of Calumpit NorthCrenz AcedillaNo ratings yet
- Cs Form No. 6 Application For Leave 2021 1 1Document1 pageCs Form No. 6 Application For Leave 2021 1 1mark jerald ritaNo ratings yet
- New Form 6 Leave Form TEACHERSDocument2 pagesNew Form 6 Leave Form TEACHERSmarites mercedNo ratings yet
- Application For Leave: Details of Action of ApplicationDocument7 pagesApplication For Leave: Details of Action of ApplicationJoanne Marie RoblesNo ratings yet
- Form 6 (Application For Leave)Document1 pageForm 6 (Application For Leave)Ccatherine Isanan-HilisanNo ratings yet
- Application For LeaveDocument2 pagesApplication For LeaveRAndy rodelasNo ratings yet
- Form 6 Revised 2020 RegionDocument5 pagesForm 6 Revised 2020 RegionLIEZEL BERSALESNo ratings yet
- Application For Leave: Cs Form 6Document2 pagesApplication For Leave: Cs Form 6Eduardo Jr PorrasNo ratings yet
- Form 6 NewDocument6 pagesForm 6 NewAnn Kempher Viernes NovalNo ratings yet
- Application For Leave (Form 6)Document1 pageApplication For Leave (Form 6)MARCELINA CABARINGNo ratings yet
- Application For Leave: Sardua Maria Calpiza Jauculan Assistant Regional Director Dilg R6 - OardDocument2 pagesApplication For Leave: Sardua Maria Calpiza Jauculan Assistant Regional Director Dilg R6 - OardDILG ConcepcionNo ratings yet
- CS Form No. 6 Revised 2020 Application For Leave FillableDocument3 pagesCS Form No. 6 Revised 2020 Application For Leave FillableFrenz Dela CruzNo ratings yet
- Department of Education: Application For LeaveDocument3 pagesDepartment of Education: Application For LeaveNicole Mo IINo ratings yet
- Leave Form For SH or Principal 1 Day 29 DaysDocument4 pagesLeave Form For SH or Principal 1 Day 29 Daysneri jadeNo ratings yet
- FORM6 DepEd CODEDDocument3 pagesFORM6 DepEd CODEDMaitem Stephanie GalosNo ratings yet
- CS Form No. 6 Revised 2020 Application For Leave FillableDocument2 pagesCS Form No. 6 Revised 2020 Application For Leave Fillablerhoda marimlaNo ratings yet
- Leave FormDocument1 pageLeave FormPrincess AmarahNo ratings yet
- Application For LeaveDocument2 pagesApplication For LeaveJinn Dalisay Uy100% (3)
- CSC Leave FormDocument2 pagesCSC Leave FormJosefina-RHUNo ratings yet
- New Format Form 6Document2 pagesNew Format Form 6rosette UngabNo ratings yet
- Department of Education: Application For LeaveDocument1 pageDepartment of Education: Application For LeavePatudan ESNo ratings yet
- Leave FormDocument2 pagesLeave FormMichaelle BunaoNo ratings yet
- Leave FormDocument1 pageLeave FormReffinej Abu de VillaNo ratings yet
- CS Form No. 6 Revised 2020 Application For Leave UpdatedDocument6 pagesCS Form No. 6 Revised 2020 Application For Leave Updatedpared1414No ratings yet
- CS Form No. 6 Revised 2020 Application For Leave Fillable 1 2Document4 pagesCS Form No. 6 Revised 2020 Application For Leave Fillable 1 2dyvejoytNo ratings yet
- Application For LeaveDocument10 pagesApplication For LeaveMary Ann AlmadinNo ratings yet
- Application For Leave: Department of EducationDocument10 pagesApplication For Leave: Department of EducationCHERRY UNANo ratings yet
- Application For Leave: 9 Days Below)Document3 pagesApplication For Leave: 9 Days Below)Nona Shella Diaz AbelgasNo ratings yet
- Application For Leave Ramos Raul Junio: Head Teacher I Catalino Castaneda ES / Bayambang IIDocument2 pagesApplication For Leave Ramos Raul Junio: Head Teacher I Catalino Castaneda ES / Bayambang IIraul ramosNo ratings yet
- NEW CS Form No. 6 Revised 2020 Application For Leave Fillable 1Document3 pagesNEW CS Form No. 6 Revised 2020 Application For Leave Fillable 1Reymart BorresNo ratings yet
- TEACHER CS Form No. 6 Revised 2020 Application For Leave Fillable 1 2020 Updated1Document2 pagesTEACHER CS Form No. 6 Revised 2020 Application For Leave Fillable 1 2020 Updated1Helen Joy Grijaldo JueleNo ratings yet
- CS Form No. 6 Revised 2020 Application For Leave Fillable 1Document4 pagesCS Form No. 6 Revised 2020 Application For Leave Fillable 1Gabriel De Los ReyesNo ratings yet
- CS Form No. 6 Revised 2020 More Than 60 DaysDocument1 pageCS Form No. 6 Revised 2020 More Than 60 DaysMa Ann Jubay Limbaga-BasaloNo ratings yet
- Leave Form CS Form No. 6 Revised 2020Document3 pagesLeave Form CS Form No. 6 Revised 2020Jeffree Lann AlvarezNo ratings yet
- Application For LeaveDocument2 pagesApplication For LeaveGeorge Blaire RasNo ratings yet
- CS Form No. 6 Revised 2023Document2 pagesCS Form No. 6 Revised 2023ANA CELLA MARZONo ratings yet
- CS Form No. 6 Revised 2020 2Document14 pagesCS Form No. 6 Revised 2020 2Geralyn GulaneNo ratings yet
- CS Form No. 6 Revised 2020 Application For LeaveDocument2 pagesCS Form No. 6 Revised 2020 Application For LeaveMara HeramizNo ratings yet
- Form-6 2023Document2 pagesForm-6 2023Chaselle PortesNo ratings yet
- BPS Form 6 Application For LeaveDocument2 pagesBPS Form 6 Application For LeaveAR IvleNo ratings yet
- Leave Form FORM 6 KARTDocument10 pagesLeave Form FORM 6 KARTPaaralan Ng PaclasanNo ratings yet
- Application For LeaveDocument2 pagesApplication For LeaveChristine Joy LozaresNo ratings yet
- Leave Form BLANKDocument1 pageLeave Form BLANKankarapeNo ratings yet
- Leave Form CS Form No. 6 Revised 2020Document4 pagesLeave Form CS Form No. 6 Revised 2020EdgarNo ratings yet
- Application For Leave: de Guzman Theresa Faye Aquino Adas Ii AccountingDocument2 pagesApplication For Leave: de Guzman Theresa Faye Aquino Adas Ii AccountingTheresa Faye De GuzmanNo ratings yet
- Form 6 1 NewDocument4 pagesForm 6 1 NewNiño PiornatoNo ratings yet
- Form 6 Leave Paper Revised 2021Document2 pagesForm 6 Leave Paper Revised 2021marites gallardoNo ratings yet
- CS Form No. 6 Revised 2020 Application For Leave Fillable 1Document4 pagesCS Form No. 6 Revised 2020 Application For Leave Fillable 1Joevan VillaflorNo ratings yet
- Department of Education: Application For LeaveDocument1 pageDepartment of Education: Application For LeaveRyan EnriquezNo ratings yet
- Out Patient (Specify)Document1 pageOut Patient (Specify)Toga MarMarNo ratings yet
- Form 6 NewDocument2 pagesForm 6 NewJenevey AlcoberNo ratings yet
- Leave FormDocument3 pagesLeave Formchito SarmientoNo ratings yet
- A. Application For Leave: CSC Form 6Document1 pageA. Application For Leave: CSC Form 6giareysieNo ratings yet
- CS Form No. 6, Revised 2020 (Application For Leave) (Fillable)Document2 pagesCS Form No. 6, Revised 2020 (Application For Leave) (Fillable)ArlanNo ratings yet
- Leave Form For SH or Principal (1 Day-60 Days)Document3 pagesLeave Form For SH or Principal (1 Day-60 Days)mark joseph quichoNo ratings yet
- Job Stress QuestionnaireDocument2 pagesJob Stress QuestionnaireMake Image RealNo ratings yet
- Would You Rather Be An Entrepreneur 2Document25 pagesWould You Rather Be An Entrepreneur 2Eduardo CanelaNo ratings yet
- Slord Development V NoyaDocument9 pagesSlord Development V NoyaJulius Edward GuzmanNo ratings yet
- Ranking Method of Performance AppraisalDocument6 pagesRanking Method of Performance AppraisalKyle annie100% (1)
- Article XiiiDocument21 pagesArticle XiiiJan Marlowe ArcoNo ratings yet
- Career Aspirations of GenerationzDocument4 pagesCareer Aspirations of Generationzvikas kunduNo ratings yet
- The Employment of Labour (Standing Orders) Act, 1965Document21 pagesThe Employment of Labour (Standing Orders) Act, 1965mrshaha2005No ratings yet
- Hudson The Case For Work Life BalanceDocument39 pagesHudson The Case For Work Life BalanceGABRIEL ELLISENo ratings yet
- ANNEX E Terminos y Condiciones Generales Contratos de Servicios UNICEFDocument14 pagesANNEX E Terminos y Condiciones Generales Contratos de Servicios UNICEFLuis Fernando Gomez suarezNo ratings yet
- Technical CorrespondenceDocument21 pagesTechnical Correspondenceirfan khosoNo ratings yet
- CHAPTER VI - Socio-Economic AspectDocument4 pagesCHAPTER VI - Socio-Economic AspectJun RecuerdoNo ratings yet
- Training and DevelopmentDocument12 pagesTraining and DevelopmentASNENo ratings yet
- Career Management - Meaning, Process and Objectives - Marketing91Document18 pagesCareer Management - Meaning, Process and Objectives - Marketing91AhlamNo ratings yet
- Headspace White Paper - Stress at Work - How Mindfulness Can HelpDocument8 pagesHeadspace White Paper - Stress at Work - How Mindfulness Can Helpsantiago macias0% (1)
- 1Document7 pages1Yak LeeNo ratings yet
- Employment Ordinance, Chapter 57 - Rest Days, Holidays and LeaveDocument0 pagesEmployment Ordinance, Chapter 57 - Rest Days, Holidays and Leavesasi_hkNo ratings yet
- CNA-Comelec CNADocument16 pagesCNA-Comelec CNApaomillan0423No ratings yet
- Seminar Primark Case StudyDocument7 pagesSeminar Primark Case StudyAdeline OtNo ratings yet
- 15 Dagasdas v. GrandplacementDocument12 pages15 Dagasdas v. GrandplacementClarissa SawaliNo ratings yet
- Basic Concepts and Principles of Construction Claims - Khuong Do BlogDocument12 pagesBasic Concepts and Principles of Construction Claims - Khuong Do BlogKhuong DoNo ratings yet
- Managing People and OrganizationDocument1 pageManaging People and OrganizationLea Mae NepuetoNo ratings yet
- KDSDocument69 pagesKDSTehsin Zaman67% (6)
- M6931 Legal Services in Australia Industry ReportDocument32 pagesM6931 Legal Services in Australia Industry ReportAnge OuNo ratings yet
- 35 Paquette V Amaruk Wilderness and Another No 4 2016 BCHRT 35Document28 pages35 Paquette V Amaruk Wilderness and Another No 4 2016 BCHRT 35The Vancouver SunNo ratings yet
- Session1 (1) JuanaDocument2 pagesSession1 (1) JuanaKammla MirandaNo ratings yet
- UiPath-Future of Work TLPDocument16 pagesUiPath-Future of Work TLPAbdoul Quang CuongNo ratings yet
- 2-RFP-18-006 FY2018 Tree Planting Project PDFDocument74 pages2-RFP-18-006 FY2018 Tree Planting Project PDFMarc BosiNo ratings yet