Download as pdf or txt
You might also like
- H145 Transition Pilot - POI - 3 Week CourseDocument6 pagesH145 Transition Pilot - POI - 3 Week CourseAlex100% (1)
- Urology MCQs PDFDocument13 pagesUrology MCQs PDFendiNo ratings yet
- Associate Professor:Ivan Bonet. Obstetric and Gynecology Associate Professor:Ivan Bonet. Obstetric and GynecologyDocument31 pagesAssociate Professor:Ivan Bonet. Obstetric and Gynecology Associate Professor:Ivan Bonet. Obstetric and Gynecologyivan0% (1)
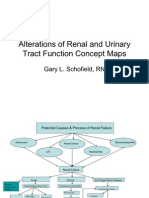
- Renal Concept MapDocument8 pagesRenal Concept MapRob DavilaNo ratings yet
- 01.EHS Elevator IL Course Material UpdatedDocument87 pages01.EHS Elevator IL Course Material UpdatedSamir ZaghloolNo ratings yet
- 2014-06-03 Construction Meeting Minutes PDFDocument3 pages2014-06-03 Construction Meeting Minutes PDFIthacaVoiceNo ratings yet
- Mnlkaxi QH: Manisha M.Sc. NursingDocument57 pagesMnlkaxi QH: Manisha M.Sc. NursingManisha ShakyaNo ratings yet
- Xv-B.pathologic Fetal Kidneys 2017Document8 pagesXv-B.pathologic Fetal Kidneys 2017jamiladeguzmanabcdefghijklmNo ratings yet
- Pediatric Urological Disorders: Professor Adel Al-HunayanDocument44 pagesPediatric Urological Disorders: Professor Adel Al-Hunayanmarina_shawkyNo ratings yet
- HydronephrosisDocument43 pagesHydronephrosisjessyNo ratings yet
- Kidney & Urinary Tract USDocument62 pagesKidney & Urinary Tract USBayarbaatar BoldNo ratings yet
- 03 US Alteraciones Congenitas RiñonDocument7 pages03 US Alteraciones Congenitas RiñonDonaldo ReleyNo ratings yet
- Radiologic Examination of The Urinary Tract: Dr. Dr. Soetojo, SpuDocument27 pagesRadiologic Examination of The Urinary Tract: Dr. Dr. Soetojo, SpuMeyLuvQiNo ratings yet
- NMT11 Urology Special NoteDocument36 pagesNMT11 Urology Special NoteYiba Zul100% (4)
- 2.obstruction of The Urinary TractDocument22 pages2.obstruction of The Urinary TractAkli JahNo ratings yet
- Obstructive Uropathy: Nitha. K 2 Year MSC NursingDocument67 pagesObstructive Uropathy: Nitha. K 2 Year MSC NursingNITHA KNo ratings yet
- Acterial Yelonephritis: Jennifer Good, DVM Mark P. Rondeau, DVM, DACVIM (SAIM)Document5 pagesActerial Yelonephritis: Jennifer Good, DVM Mark P. Rondeau, DVM, DACVIM (SAIM)Phương Liên Nguyễn ThịNo ratings yet
- 07 - Basics of Adrenal Urinary Tract Prostate and Testicle ImagingDocument139 pages07 - Basics of Adrenal Urinary Tract Prostate and Testicle ImagingHusam AbuodehNo ratings yet
- C5. Renal Disorders FileDocument38 pagesC5. Renal Disorders Filecoco brillqnteNo ratings yet
- 20 - Pediatric Urinary DisordersDocument62 pages20 - Pediatric Urinary DisordersKhaalid AbdirahmanNo ratings yet
- Congenital Urological Conditions - Dr. HawkarDocument38 pagesCongenital Urological Conditions - Dr. HawkarBashar KhalilNo ratings yet
- Menstrual DisordersDocument29 pagesMenstrual DisorderstuhinsinghNo ratings yet
- Pediatric Urologic Emergencies 1Document34 pagesPediatric Urologic Emergencies 1Waseem MoukhtarNo ratings yet
- Horseshoe Kidney: Prof DR DR Haerani Rasyid, Mes, SPPD, KGH, SPGK Tim Ginjal Hipertensi Unhas 2018Document16 pagesHorseshoe Kidney: Prof DR DR Haerani Rasyid, Mes, SPPD, KGH, SPGK Tim Ginjal Hipertensi Unhas 2018ummuhaniNo ratings yet
- Anorectal Disease and Common Anorectal DisordersDocument2 pagesAnorectal Disease and Common Anorectal DisordersIsabel CastilloNo ratings yet
- Sistem UrinariaDocument42 pagesSistem UrinariaHanny da GamaNo ratings yet
- Abdominal MassDocument5 pagesAbdominal MassArthana PutraNo ratings yet
- Urinary Track Infections . .1Document40 pagesUrinary Track Infections . .1ayesha sagheerNo ratings yet
- 1 ScrotumDocument7 pages1 ScrotumMohamed Al-zichrawyNo ratings yet
- Lo Week 5-1Document13 pagesLo Week 5-1Martien Silviandy SetiawanNo ratings yet
- Emergency in Urology - Edit241021Document76 pagesEmergency in Urology - Edit241021Alverina Ode Nifaki100% (1)
- Ch19-Pancreas - Mod3Document41 pagesCh19-Pancreas - Mod3mikky8204No ratings yet
- Acute and Chronic Urinary RetentionDocument3 pagesAcute and Chronic Urinary RetentionParyNo ratings yet
- Congenitalrenalanomalies 161209072225Document68 pagesCongenitalrenalanomalies 161209072225Ali SlimaniNo ratings yet
- Ms Reviewer Renal UrinaryDocument5 pagesMs Reviewer Renal UrinaryAlyssa Nicole CajayonNo ratings yet
- Approaches To Abdominal MassDocument49 pagesApproaches To Abdominal MassPatrick JohnNo ratings yet
- Test 3 NotesDocument35 pagesTest 3 Notesbjpalmer100% (2)
- Hematuria in ChildrenDocument27 pagesHematuria in ChildrenKousik AmancharlaNo ratings yet
- Scrotal AbnormalitiesDocument38 pagesScrotal AbnormalitiesmoominjunaidNo ratings yet
- Hydronephrosis OutlineDocument13 pagesHydronephrosis OutlineSarah Sy-SantosNo ratings yet
- CancersDocument39 pagesCancersmustafa atayaNo ratings yet
- Obstruksi Uropati IrfanDocument43 pagesObstruksi Uropati IrfanirfanNo ratings yet
- Block 3.3 Sesi 3 Pathology of Urinary Tract: by Asdos 2011: Vetta Awe Eric Lily Fiko Ghana Ikal Linda May FahmiDocument96 pagesBlock 3.3 Sesi 3 Pathology of Urinary Tract: by Asdos 2011: Vetta Awe Eric Lily Fiko Ghana Ikal Linda May Fahmimail junkNo ratings yet
- Urinary Symptoms - DR RashaDocument70 pagesUrinary Symptoms - DR RashaRasha TelebNo ratings yet
- Urinary System and Male Genital: Fajar L. Gultom Departemen Patologi Anatomik FK UKI December 2017Document50 pagesUrinary System and Male Genital: Fajar L. Gultom Departemen Patologi Anatomik FK UKI December 2017Sona SiburianNo ratings yet
- CAKUTDocument50 pagesCAKUTsantosh subediNo ratings yet
- Diana's Renal DiseasesDocument9 pagesDiana's Renal DiseasesdhyltonNo ratings yet
- 9.emma Renal Cysts Hanoi 2018Document39 pages9.emma Renal Cysts Hanoi 2018vd hungNo ratings yet
- Acuteurologicalconditions 130121123140 Phpapp01Document58 pagesAcuteurologicalconditions 130121123140 Phpapp01Dr. NasrumminallahNo ratings yet
- Urinary Incontinence, Pelvic Prolapse & Cancer ScreeningDocument25 pagesUrinary Incontinence, Pelvic Prolapse & Cancer ScreeningIsraa AlaaNo ratings yet
- Kidney, Bladder and Prostate Pathology For Allied Health SciencesDocument38 pagesKidney, Bladder and Prostate Pathology For Allied Health SciencesMichael BrownNo ratings yet
- Management ofARM&HSD 1Document54 pagesManagement ofARM&HSD 1Hayle MaryamNo ratings yet
- Congenital Anomalies of The KidneyDocument21 pagesCongenital Anomalies of The KidneyRaghu Rajan100% (1)
- Anomalies of The Upper Urinary TractDocument6 pagesAnomalies of The Upper Urinary TractMohamed Al-zichrawyNo ratings yet
- Renal Concept MapDocument8 pagesRenal Concept MapXtine CajiNo ratings yet
- Dr. Ghada Abu ShoshaDocument42 pagesDr. Ghada Abu Shoshatalaekrema01No ratings yet
- Fabry DiseaseDocument63 pagesFabry DiseaseKunal PaulNo ratings yet
- PELVIC URETERIC JUNCTION OBSTRUCTIONDocument75 pagesPELVIC URETERIC JUNCTION OBSTRUCTIONNoor AinNo ratings yet
- Litiasis VesicularDocument26 pagesLitiasis VesicularEULER FARADAY ALTAMIRANO FARFANNo ratings yet
- Sirosis Hepatis-Dikonversi-DikompresiDocument22 pagesSirosis Hepatis-Dikonversi-DikompresiAa SsNo ratings yet
- Abortion and Its Complications 2Document17 pagesAbortion and Its Complications 2api-3705046100% (2)
- Factors That Contribute To Successful Baking 9Document3 pagesFactors That Contribute To Successful Baking 9Michael Angelo Dela MasaNo ratings yet
- 22 Disritmia 2018Document60 pages22 Disritmia 2018Nur akilaNo ratings yet
- Removal of 1,2-Dichloroethane From Industrial Wastewater With Membrane FiltrationDocument9 pagesRemoval of 1,2-Dichloroethane From Industrial Wastewater With Membrane FiltrationArash AbbasiNo ratings yet
- Platts Nucleonics Week 19 July2012Document15 pagesPlatts Nucleonics Week 19 July2012Jovi Savitri Eka PutriNo ratings yet
- Playground Antonyms PDFDocument2 pagesPlayground Antonyms PDFChayne RodilNo ratings yet
- Therapeutic Modalities and RehabDocument77 pagesTherapeutic Modalities and RehabHarish Pai K100% (1)
- Company Profile - PretechDocument26 pagesCompany Profile - PretechanandivmNo ratings yet
- Cestode Parasites: Medical Parasitology, 2009 University of Palangkaraya Agus HaryonoDocument45 pagesCestode Parasites: Medical Parasitology, 2009 University of Palangkaraya Agus HaryonoMeylisa Gerson BayanNo ratings yet
- Elctrical Safety PaperV3 1Document6 pagesElctrical Safety PaperV3 120082012No ratings yet
- Living: Holiday CookbookDocument26 pagesLiving: Holiday CookbookКсения Карлина100% (4)
- 08CLecture - Welding Codes StandardsDocument15 pages08CLecture - Welding Codes StandardsDavid HuamanNo ratings yet
- USFS Mission - Tanzania - May 2009 - Water Resources in Tabora and Rukwa - For FRAMEDocument57 pagesUSFS Mission - Tanzania - May 2009 - Water Resources in Tabora and Rukwa - For FRAMERahul K Awade0% (1)
- Ra - AER003N PPRDocument1 pageRa - AER003N PPRShyam Sundar SahooNo ratings yet
- Mcqs On Agronomy: 1. Agriculture Is ADocument110 pagesMcqs On Agronomy: 1. Agriculture Is Ajamil ahmadNo ratings yet
- Eia - 1317 Study Report - Daystar DamDocument78 pagesEia - 1317 Study Report - Daystar DamRonnie WartNo ratings yet
- Process of HospitalizationDocument24 pagesProcess of HospitalizationFara Zaman100% (3)
- LeaP Science G7 Week 3 Q4 - JPSDocument7 pagesLeaP Science G7 Week 3 Q4 - JPSEdralyn PaduaNo ratings yet
- Automobile Technology: Engine MechanicalDocument3 pagesAutomobile Technology: Engine MechanicalWawan PrastiyantoNo ratings yet
- Lab 5 ImineDocument10 pagesLab 5 ImineCheng FuNo ratings yet
- Flamboyant Tree InformationDocument18 pagesFlamboyant Tree InformationHaimeNo ratings yet
- Mental AltitudeDocument16 pagesMental AltitudeAman OjhaNo ratings yet
- Lee Kok LiangDocument8 pagesLee Kok LiangAnonymous LGB1O2fA0% (1)
- Flojet Beverage CatDocument24 pagesFlojet Beverage CatRacil EzzedineNo ratings yet
- Binocular Vision ScheimanDocument732 pagesBinocular Vision ScheimanOptom Dang100% (1)
- Fuses and Its Types: C065 - C071 - C076 - C093Document20 pagesFuses and Its Types: C065 - C071 - C076 - C093Prapti PatelNo ratings yet
- Admin Assistant Receptionist Job DescriptionDocument4 pagesAdmin Assistant Receptionist Job DescriptionMitTuyetNo ratings yet
- Geotechnical Investigation Report TemplatesDocument16 pagesGeotechnical Investigation Report TemplatesCamille Angelie Soribello63% (8)