
Soliqua 100/33 (Insulin Glargine Plus Lixisenatide) Receives FDA Approval For Adults With Type 2 Diabetes
Soliqua 100/33 (Insulin Glargine Plus Lixisenatide) Receives FDA Approval For Adults With Type 2 Diabetes
You might also like
- Hesi Dosage Calculation Practice ExamDocument7 pagesHesi Dosage Calculation Practice ExamAna Bienne100% (1)
- Pharmacology Review NotesDocument24 pagesPharmacology Review NotescampbellqueenNo ratings yet
- Insulin Drug StudyDocument2 pagesInsulin Drug StudyRai Hanah92% (13)
- Practical Insulin: A Handbook for Prescribing ProvidersFrom EverandPractical Insulin: A Handbook for Prescribing ProvidersRating: 5 out of 5 stars5/5 (2)
- VancomycinDocument2 pagesVancomycinRye AnchNo ratings yet
- Diabetes SobrebasalizaciónDocument7 pagesDiabetes SobrebasalizaciónComisión Académica FCM - UNAHNo ratings yet
- Pharmacologic Approaches To Glycemic Treatment Standards of Medical Care in Diabetes-2018Document13 pagesPharmacologic Approaches To Glycemic Treatment Standards of Medical Care in Diabetes-2018ferrossanchezNo ratings yet
- Ajhp 140168Document12 pagesAjhp 140168cherrygems99No ratings yet
- What Is Diabetes, Its Types, Role of Insulin and Hypoglycemic Agents, Mode of Action, Side Effects, Pharmacodynamics and PharmacokineticsDocument9 pagesWhat Is Diabetes, Its Types, Role of Insulin and Hypoglycemic Agents, Mode of Action, Side Effects, Pharmacodynamics and PharmacokineticsIshaani GargNo ratings yet
- DR. BABUJANARTHANAN Antihyperglycemia DrugsDocument5 pagesDR. BABUJANARTHANAN Antihyperglycemia DrugsJerry TyokosuNo ratings yet
- Antidiabetic Drugs. Nurse 2024Document32 pagesAntidiabetic Drugs. Nurse 2024Ayro Business CenterNo ratings yet
- IJAMSCR-17-223 - 426-433 Review On Adverse Drug Reaction of Antidiabetic Drugs PDFDocument8 pagesIJAMSCR-17-223 - 426-433 Review On Adverse Drug Reaction of Antidiabetic Drugs PDFtrupetiNo ratings yet
- Pharmacology Reading Materials On DMDocument19 pagesPharmacology Reading Materials On DMJames SoeNo ratings yet
- Glubitor OdDocument7 pagesGlubitor OdSerenaNo ratings yet
- Pharmacology Chapter 38Document7 pagesPharmacology Chapter 38languha NgatiNo ratings yet
- Manejo de La DMGDocument5 pagesManejo de La DMGsandymejiaNo ratings yet
- Insulin Dan Oral DiabetesDocument30 pagesInsulin Dan Oral DiabetesIrsan Fahmi ANo ratings yet
- Steps: Liraglutide (Saxenda) For Weight LossDocument2 pagesSteps: Liraglutide (Saxenda) For Weight LossCésar EscalanteNo ratings yet
- Treatment of Diabetes MellitusDocument31 pagesTreatment of Diabetes MellitusIrfan IdealistNo ratings yet
- Incretin PharmDocument3 pagesIncretin PharmSlim SaaryNo ratings yet
- Drugs of DiabetesDocument42 pagesDrugs of Diabeteskwennybiang100% (1)
- Insulin Degludec Insulin Aspart (Ryzodeg 70 30) Prescribing ProtocolDocument5 pagesInsulin Degludec Insulin Aspart (Ryzodeg 70 30) Prescribing ProtocolMiraNo ratings yet
- PMC4020327-jdi 12214Document11 pagesPMC4020327-jdi 12214anca irinaNo ratings yet
- Glycemic and IRDocument10 pagesGlycemic and IRAyman AleemNo ratings yet
- DiabetesAlgorithm Stanford2018Document7 pagesDiabetesAlgorithm Stanford2018Rogelio MoscosoNo ratings yet
- لقطة شاشة ٢٠٢١-٠٢-٠٥ في ١.٤٦.٥٧ مDocument2 pagesلقطة شاشة ٢٠٢١-٠٢-٠٥ في ١.٤٦.٥٧ مDr. Emad Elbadawy د عماد البدويNo ratings yet
- (Product Name) MR Tablet 30mg (Product Name) MR Tablet 60mgDocument10 pages(Product Name) MR Tablet 30mg (Product Name) MR Tablet 60mggmsanto7No ratings yet
- Drug Interaction DMT2Document12 pagesDrug Interaction DMT2Dhonat FlashNo ratings yet
- Blood Glucose Control Pathway in Type 2 Diabetes Apr 2013Document2 pagesBlood Glucose Control Pathway in Type 2 Diabetes Apr 2013J WongNo ratings yet
- Effect of The GLP-1 Receptor Agonist Lixisenatide On Counter-Regulatory Responses To Hypoglycemia in Subjects With Insulin-Treated Type 2 DiabetesDocument8 pagesEffect of The GLP-1 Receptor Agonist Lixisenatide On Counter-Regulatory Responses To Hypoglycemia in Subjects With Insulin-Treated Type 2 DiabetestarietarooNo ratings yet
- The Frequency of Insulin GlargineDocument1 pageThe Frequency of Insulin GlargineSimona RaduNo ratings yet
- Soliqua LeafletDocument39 pagesSoliqua LeafletxtineNo ratings yet
- Newagentsforthe Treatmentoftype2Diabetes: Renata Libianto,, Elif I. EkinciDocument14 pagesNewagentsforthe Treatmentoftype2Diabetes: Renata Libianto,, Elif I. EkinciMilo De EscorpioNo ratings yet
- Pharmacotherapy of DMDocument28 pagesPharmacotherapy of DMQueenElsaNo ratings yet
- Drugs For Diabetes (Part 1)Document6 pagesDrugs For Diabetes (Part 1)حوراء عارف الموسويNo ratings yet
- Drugs in Type 2 DMDocument18 pagesDrugs in Type 2 DMhussain AltaherNo ratings yet
- DOM-24-1159 Fixed Ratio Insuline GlarginaDocument7 pagesDOM-24-1159 Fixed Ratio Insuline GlarginaLucia Guzman FernandezNo ratings yet
- Insulin Treatment in DiabetesDocument86 pagesInsulin Treatment in DiabetesAhsan Rauf100% (1)
- LantusDocument10 pagesLantusShanta100% (3)
- Diabetes MellitusDocument9 pagesDiabetes Mellitusapi-708254576No ratings yet
- Pharm Ch. 33 StudentDocument51 pagesPharm Ch. 33 Studentlizzy_lee23No ratings yet
- Diabetes Treatment: Dr. Chavan P.R. Pharm DDocument73 pagesDiabetes Treatment: Dr. Chavan P.R. Pharm DAvel ChandNo ratings yet
- 02 - Update Article New Oral Antidiabetic AgentsDocument7 pages02 - Update Article New Oral Antidiabetic AgentsMuhammad Lutfi Al AyubiNo ratings yet
- 02 Tatalaksana Terapi Insulin - Prof Tri Murti AndayaniDocument39 pages02 Tatalaksana Terapi Insulin - Prof Tri Murti AndayaniEndang Wulan SariNo ratings yet
- Endo Pharma ElhDocument14 pagesEndo Pharma Elhodiodi57No ratings yet
- Analogos de Insulina en DM 1 2017Document15 pagesAnalogos de Insulina en DM 1 2017LaurenArperNo ratings yet
- Endocrine SystemDocument21 pagesEndocrine SystemMona MahfouzNo ratings yet
- New Technologies and Therapies in The Management of DiabetesDocument8 pagesNew Technologies and Therapies in The Management of DiabetesArhaMozaNo ratings yet
- Hes 005 Session 16 SasDocument7 pagesHes 005 Session 16 SasJose Melmar Autida AutenticoNo ratings yet
- Gliclazide Diamicron: Generic Name Trade NameDocument8 pagesGliclazide Diamicron: Generic Name Trade NameIsabella SamsonNo ratings yet
- Type 2 DiabetesDocument2 pagesType 2 DiabetessaroshNo ratings yet
- Drugs For Diabetes MellitusDocument50 pagesDrugs For Diabetes MellitusCherenet TomaNo ratings yet
- LEC#37 Anti Diabetic Drugs (Insulin)Document20 pagesLEC#37 Anti Diabetic Drugs (Insulin)alihyderabro166No ratings yet
- General Principles of Insulin Therapy in Diabetes MellitusDocument12 pagesGeneral Principles of Insulin Therapy in Diabetes MellitusRuban RichardNo ratings yet
- Pharmacologic TheraphyDocument32 pagesPharmacologic TheraphyquinnNo ratings yet
- Galvus: Name of The MedicineDocument19 pagesGalvus: Name of The MedicinevrtzioNo ratings yet
- Saxagliptin and Metformin in Fixed Combination For The Treatment of Type 2 Diabetes in AdultsDocument11 pagesSaxagliptin and Metformin in Fixed Combination For The Treatment of Type 2 Diabetes in AdultsLaura MelatiNo ratings yet
- Novorapid Product Monograph PDFDocument50 pagesNovorapid Product Monograph PDFAtid AmandaNo ratings yet
- Endocrine CologyDocument124 pagesEndocrine CologyBehailu TejeNo ratings yet
- Insulin and Antidiabetic Drugs: Prof - DR Asya RehmanDocument23 pagesInsulin and Antidiabetic Drugs: Prof - DR Asya RehmanGareth BaleNo ratings yet
- Insulin Therapy in Type 2 Diabetes MellitusDocument40 pagesInsulin Therapy in Type 2 Diabetes MellitusEDWIN WIJAYANo ratings yet
- Insulin PharmacologyDocument4 pagesInsulin PharmacologySunilNo ratings yet
- Drugs That Cannot Be Crushed - Ms. HopeDocument4 pagesDrugs That Cannot Be Crushed - Ms. Hopemiggy13No ratings yet
- Kalium Durule Drug StudyDocument2 pagesKalium Durule Drug StudymichelleNo ratings yet
- Dosage AdjustmentDocument10 pagesDosage AdjustmentNido MalghaniNo ratings yet
- Mechanisms of Action OF Antifungal AgentsDocument5 pagesMechanisms of Action OF Antifungal AgentsshaitabliganNo ratings yet
- KetoconazoleDocument2 pagesKetoconazolenatinlalaNo ratings yet
- Antihistamine PresentationDocument34 pagesAntihistamine PresentationOpa Evilsiam100% (1)
- KeolaxDocument2 pagesKeolaxSaifur Rahman SuzonNo ratings yet
- Zinc SulfateDocument1 pageZinc SulfateAnna LaritaNo ratings yet
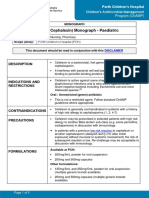
- Cefalexin (Cephalexin) Monograph - Paediatric: DescriptionDocument5 pagesCefalexin (Cephalexin) Monograph - Paediatric: Descriptioneinas omerNo ratings yet
- 1 Early Access Application 14 May 2018 PDFDocument2 pages1 Early Access Application 14 May 2018 PDFArdat LiliNo ratings yet
- Factors Affecting Drug Metabolism PDFDocument2 pagesFactors Affecting Drug Metabolism PDFPaige50% (2)
- Drug StudyDocument3 pagesDrug StudyPsalms Aubrey Domingo AcostaNo ratings yet
- NorgesicDocument3 pagesNorgesicValerie Santa GalganiNo ratings yet
- Coldex CapsuleDocument3 pagesColdex Capsulehk_scribdNo ratings yet
- Structure Activity Relationship of Steroids: by Dr. Preetish Ku. PanigrahyDocument39 pagesStructure Activity Relationship of Steroids: by Dr. Preetish Ku. Panigrahypreetish50% (4)
- StreptomycinDocument1 pageStreptomycinDemilyn Fat100% (2)
- 2022 Sept 30 DpriDocument51 pages2022 Sept 30 DpriChari RivoNo ratings yet
- Critical Care Price ListDocument4 pagesCritical Care Price ListmailmeamritasharmaNo ratings yet
- Obat Sistem HematologiDocument21 pagesObat Sistem HematologiSuryana AdityaNo ratings yet
- Appendix 14 Clinical Pharmacy Screen of Medication Charts Inpatient Units 1Document5 pagesAppendix 14 Clinical Pharmacy Screen of Medication Charts Inpatient Units 1scd_chesa_189432221No ratings yet
- BronchodilatorsDocument41 pagesBronchodilatorsLeong Zhee ChuanNo ratings yet
- ETIKET BOX OBAT PATEN Box BesarDocument5 pagesETIKET BOX OBAT PATEN Box Besarbabas basriNo ratings yet
- MTUS Drug ListDocument1 pageMTUS Drug List9300187476No ratings yet
- Drug RationaleDocument77 pagesDrug RationaleYolanda WilliamsNo ratings yet
- 6 Beta Adrenergic BlockersDocument19 pages6 Beta Adrenergic Blockersmatchees-gone rogue100% (1)
- I43Be) Utaj 3A Flekot 1.: 3E14PehDocument8 pagesI43Be) Utaj 3A Flekot 1.: 3E14PehSuzana Panova-CvetkovskaNo ratings yet
- ASHP - Guidelines On Preventing Medication ErrorsDocument17 pagesASHP - Guidelines On Preventing Medication Errorsstudy bandingNo ratings yet
- Permintaan Pustu Burmeso Agustus 2023Document3 pagesPermintaan Pustu Burmeso Agustus 2023Black Bullet13No ratings yet






















































































Download as pdf or txt
You might also like
- Hesi Dosage Calculation Practice ExamDocument7 pagesHesi Dosage Calculation Practice ExamAna Bienne100% (1)
- Pharmacology Review NotesDocument24 pagesPharmacology Review NotescampbellqueenNo ratings yet
- Insulin Drug StudyDocument2 pagesInsulin Drug StudyRai Hanah92% (13)
- Practical Insulin: A Handbook for Prescribing ProvidersFrom EverandPractical Insulin: A Handbook for Prescribing ProvidersRating: 5 out of 5 stars5/5 (2)
- VancomycinDocument2 pagesVancomycinRye AnchNo ratings yet
- Diabetes SobrebasalizaciónDocument7 pagesDiabetes SobrebasalizaciónComisión Académica FCM - UNAHNo ratings yet
- Pharmacologic Approaches To Glycemic Treatment Standards of Medical Care in Diabetes-2018Document13 pagesPharmacologic Approaches To Glycemic Treatment Standards of Medical Care in Diabetes-2018ferrossanchezNo ratings yet
- Ajhp 140168Document12 pagesAjhp 140168cherrygems99No ratings yet
- What Is Diabetes, Its Types, Role of Insulin and Hypoglycemic Agents, Mode of Action, Side Effects, Pharmacodynamics and PharmacokineticsDocument9 pagesWhat Is Diabetes, Its Types, Role of Insulin and Hypoglycemic Agents, Mode of Action, Side Effects, Pharmacodynamics and PharmacokineticsIshaani GargNo ratings yet
- DR. BABUJANARTHANAN Antihyperglycemia DrugsDocument5 pagesDR. BABUJANARTHANAN Antihyperglycemia DrugsJerry TyokosuNo ratings yet
- Antidiabetic Drugs. Nurse 2024Document32 pagesAntidiabetic Drugs. Nurse 2024Ayro Business CenterNo ratings yet
- IJAMSCR-17-223 - 426-433 Review On Adverse Drug Reaction of Antidiabetic Drugs PDFDocument8 pagesIJAMSCR-17-223 - 426-433 Review On Adverse Drug Reaction of Antidiabetic Drugs PDFtrupetiNo ratings yet
- Pharmacology Reading Materials On DMDocument19 pagesPharmacology Reading Materials On DMJames SoeNo ratings yet
- Glubitor OdDocument7 pagesGlubitor OdSerenaNo ratings yet
- Pharmacology Chapter 38Document7 pagesPharmacology Chapter 38languha NgatiNo ratings yet
- Manejo de La DMGDocument5 pagesManejo de La DMGsandymejiaNo ratings yet
- Insulin Dan Oral DiabetesDocument30 pagesInsulin Dan Oral DiabetesIrsan Fahmi ANo ratings yet
- Steps: Liraglutide (Saxenda) For Weight LossDocument2 pagesSteps: Liraglutide (Saxenda) For Weight LossCésar EscalanteNo ratings yet
- Treatment of Diabetes MellitusDocument31 pagesTreatment of Diabetes MellitusIrfan IdealistNo ratings yet
- Incretin PharmDocument3 pagesIncretin PharmSlim SaaryNo ratings yet
- Drugs of DiabetesDocument42 pagesDrugs of Diabeteskwennybiang100% (1)
- Insulin Degludec Insulin Aspart (Ryzodeg 70 30) Prescribing ProtocolDocument5 pagesInsulin Degludec Insulin Aspart (Ryzodeg 70 30) Prescribing ProtocolMiraNo ratings yet
- PMC4020327-jdi 12214Document11 pagesPMC4020327-jdi 12214anca irinaNo ratings yet
- Glycemic and IRDocument10 pagesGlycemic and IRAyman AleemNo ratings yet
- DiabetesAlgorithm Stanford2018Document7 pagesDiabetesAlgorithm Stanford2018Rogelio MoscosoNo ratings yet
- لقطة شاشة ٢٠٢١-٠٢-٠٥ في ١.٤٦.٥٧ مDocument2 pagesلقطة شاشة ٢٠٢١-٠٢-٠٥ في ١.٤٦.٥٧ مDr. Emad Elbadawy د عماد البدويNo ratings yet
- (Product Name) MR Tablet 30mg (Product Name) MR Tablet 60mgDocument10 pages(Product Name) MR Tablet 30mg (Product Name) MR Tablet 60mggmsanto7No ratings yet
- Drug Interaction DMT2Document12 pagesDrug Interaction DMT2Dhonat FlashNo ratings yet
- Blood Glucose Control Pathway in Type 2 Diabetes Apr 2013Document2 pagesBlood Glucose Control Pathway in Type 2 Diabetes Apr 2013J WongNo ratings yet
- Effect of The GLP-1 Receptor Agonist Lixisenatide On Counter-Regulatory Responses To Hypoglycemia in Subjects With Insulin-Treated Type 2 DiabetesDocument8 pagesEffect of The GLP-1 Receptor Agonist Lixisenatide On Counter-Regulatory Responses To Hypoglycemia in Subjects With Insulin-Treated Type 2 DiabetestarietarooNo ratings yet
- The Frequency of Insulin GlargineDocument1 pageThe Frequency of Insulin GlargineSimona RaduNo ratings yet
- Soliqua LeafletDocument39 pagesSoliqua LeafletxtineNo ratings yet
- Newagentsforthe Treatmentoftype2Diabetes: Renata Libianto,, Elif I. EkinciDocument14 pagesNewagentsforthe Treatmentoftype2Diabetes: Renata Libianto,, Elif I. EkinciMilo De EscorpioNo ratings yet
- Pharmacotherapy of DMDocument28 pagesPharmacotherapy of DMQueenElsaNo ratings yet
- Drugs For Diabetes (Part 1)Document6 pagesDrugs For Diabetes (Part 1)حوراء عارف الموسويNo ratings yet
- Drugs in Type 2 DMDocument18 pagesDrugs in Type 2 DMhussain AltaherNo ratings yet
- DOM-24-1159 Fixed Ratio Insuline GlarginaDocument7 pagesDOM-24-1159 Fixed Ratio Insuline GlarginaLucia Guzman FernandezNo ratings yet
- Insulin Treatment in DiabetesDocument86 pagesInsulin Treatment in DiabetesAhsan Rauf100% (1)
- LantusDocument10 pagesLantusShanta100% (3)
- Diabetes MellitusDocument9 pagesDiabetes Mellitusapi-708254576No ratings yet
- Pharm Ch. 33 StudentDocument51 pagesPharm Ch. 33 Studentlizzy_lee23No ratings yet
- Diabetes Treatment: Dr. Chavan P.R. Pharm DDocument73 pagesDiabetes Treatment: Dr. Chavan P.R. Pharm DAvel ChandNo ratings yet
- 02 - Update Article New Oral Antidiabetic AgentsDocument7 pages02 - Update Article New Oral Antidiabetic AgentsMuhammad Lutfi Al AyubiNo ratings yet
- 02 Tatalaksana Terapi Insulin - Prof Tri Murti AndayaniDocument39 pages02 Tatalaksana Terapi Insulin - Prof Tri Murti AndayaniEndang Wulan SariNo ratings yet
- Endo Pharma ElhDocument14 pagesEndo Pharma Elhodiodi57No ratings yet
- Analogos de Insulina en DM 1 2017Document15 pagesAnalogos de Insulina en DM 1 2017LaurenArperNo ratings yet
- Endocrine SystemDocument21 pagesEndocrine SystemMona MahfouzNo ratings yet
- New Technologies and Therapies in The Management of DiabetesDocument8 pagesNew Technologies and Therapies in The Management of DiabetesArhaMozaNo ratings yet
- Hes 005 Session 16 SasDocument7 pagesHes 005 Session 16 SasJose Melmar Autida AutenticoNo ratings yet
- Gliclazide Diamicron: Generic Name Trade NameDocument8 pagesGliclazide Diamicron: Generic Name Trade NameIsabella SamsonNo ratings yet
- Type 2 DiabetesDocument2 pagesType 2 DiabetessaroshNo ratings yet
- Drugs For Diabetes MellitusDocument50 pagesDrugs For Diabetes MellitusCherenet TomaNo ratings yet
- LEC#37 Anti Diabetic Drugs (Insulin)Document20 pagesLEC#37 Anti Diabetic Drugs (Insulin)alihyderabro166No ratings yet
- General Principles of Insulin Therapy in Diabetes MellitusDocument12 pagesGeneral Principles of Insulin Therapy in Diabetes MellitusRuban RichardNo ratings yet
- Pharmacologic TheraphyDocument32 pagesPharmacologic TheraphyquinnNo ratings yet
- Galvus: Name of The MedicineDocument19 pagesGalvus: Name of The MedicinevrtzioNo ratings yet
- Saxagliptin and Metformin in Fixed Combination For The Treatment of Type 2 Diabetes in AdultsDocument11 pagesSaxagliptin and Metformin in Fixed Combination For The Treatment of Type 2 Diabetes in AdultsLaura MelatiNo ratings yet
- Novorapid Product Monograph PDFDocument50 pagesNovorapid Product Monograph PDFAtid AmandaNo ratings yet
- Endocrine CologyDocument124 pagesEndocrine CologyBehailu TejeNo ratings yet
- Insulin and Antidiabetic Drugs: Prof - DR Asya RehmanDocument23 pagesInsulin and Antidiabetic Drugs: Prof - DR Asya RehmanGareth BaleNo ratings yet
- Insulin Therapy in Type 2 Diabetes MellitusDocument40 pagesInsulin Therapy in Type 2 Diabetes MellitusEDWIN WIJAYANo ratings yet
- Insulin PharmacologyDocument4 pagesInsulin PharmacologySunilNo ratings yet
- Drugs That Cannot Be Crushed - Ms. HopeDocument4 pagesDrugs That Cannot Be Crushed - Ms. Hopemiggy13No ratings yet
- Kalium Durule Drug StudyDocument2 pagesKalium Durule Drug StudymichelleNo ratings yet
- Dosage AdjustmentDocument10 pagesDosage AdjustmentNido MalghaniNo ratings yet
- Mechanisms of Action OF Antifungal AgentsDocument5 pagesMechanisms of Action OF Antifungal AgentsshaitabliganNo ratings yet
- KetoconazoleDocument2 pagesKetoconazolenatinlalaNo ratings yet
- Antihistamine PresentationDocument34 pagesAntihistamine PresentationOpa Evilsiam100% (1)
- KeolaxDocument2 pagesKeolaxSaifur Rahman SuzonNo ratings yet
- Zinc SulfateDocument1 pageZinc SulfateAnna LaritaNo ratings yet
- Cefalexin (Cephalexin) Monograph - Paediatric: DescriptionDocument5 pagesCefalexin (Cephalexin) Monograph - Paediatric: Descriptioneinas omerNo ratings yet
- 1 Early Access Application 14 May 2018 PDFDocument2 pages1 Early Access Application 14 May 2018 PDFArdat LiliNo ratings yet
- Factors Affecting Drug Metabolism PDFDocument2 pagesFactors Affecting Drug Metabolism PDFPaige50% (2)
- Drug StudyDocument3 pagesDrug StudyPsalms Aubrey Domingo AcostaNo ratings yet
- NorgesicDocument3 pagesNorgesicValerie Santa GalganiNo ratings yet
- Coldex CapsuleDocument3 pagesColdex Capsulehk_scribdNo ratings yet
- Structure Activity Relationship of Steroids: by Dr. Preetish Ku. PanigrahyDocument39 pagesStructure Activity Relationship of Steroids: by Dr. Preetish Ku. Panigrahypreetish50% (4)
- StreptomycinDocument1 pageStreptomycinDemilyn Fat100% (2)
- 2022 Sept 30 DpriDocument51 pages2022 Sept 30 DpriChari RivoNo ratings yet
- Critical Care Price ListDocument4 pagesCritical Care Price ListmailmeamritasharmaNo ratings yet
- Obat Sistem HematologiDocument21 pagesObat Sistem HematologiSuryana AdityaNo ratings yet
- Appendix 14 Clinical Pharmacy Screen of Medication Charts Inpatient Units 1Document5 pagesAppendix 14 Clinical Pharmacy Screen of Medication Charts Inpatient Units 1scd_chesa_189432221No ratings yet
- BronchodilatorsDocument41 pagesBronchodilatorsLeong Zhee ChuanNo ratings yet
- ETIKET BOX OBAT PATEN Box BesarDocument5 pagesETIKET BOX OBAT PATEN Box Besarbabas basriNo ratings yet
- MTUS Drug ListDocument1 pageMTUS Drug List9300187476No ratings yet
- Drug RationaleDocument77 pagesDrug RationaleYolanda WilliamsNo ratings yet
- 6 Beta Adrenergic BlockersDocument19 pages6 Beta Adrenergic Blockersmatchees-gone rogue100% (1)
- I43Be) Utaj 3A Flekot 1.: 3E14PehDocument8 pagesI43Be) Utaj 3A Flekot 1.: 3E14PehSuzana Panova-CvetkovskaNo ratings yet
- ASHP - Guidelines On Preventing Medication ErrorsDocument17 pagesASHP - Guidelines On Preventing Medication Errorsstudy bandingNo ratings yet
- Permintaan Pustu Burmeso Agustus 2023Document3 pagesPermintaan Pustu Burmeso Agustus 2023Black Bullet13No ratings yet