Download as docx, pdf, or txt
You might also like
- Patanjali Project ReportDocument56 pagesPatanjali Project ReportJanvi SinghNo ratings yet
- Primer of Bio Statistics 5edDocument372 pagesPrimer of Bio Statistics 5edlrc3No ratings yet
- Physician Factors Associated With Polypharmacy and Potentially Inappropriate Medication UseDocument9 pagesPhysician Factors Associated With Polypharmacy and Potentially Inappropriate Medication UseratnatriaaNo ratings yet
- Añonuevo Matorres Moreno Copernicus Final-Paper-Pr2Document43 pagesAñonuevo Matorres Moreno Copernicus Final-Paper-Pr211SA AÑONUEVO MARJORIE NICOLENo ratings yet
- Have These Symptoms Buy This Drug by Pauline ChenDocument3 pagesHave These Symptoms Buy This Drug by Pauline ChensuperherosavesNo ratings yet
- BMB Final PaperDocument5 pagesBMB Final Paperapi-285356783No ratings yet
- Research Paper On PolypharmacyDocument5 pagesResearch Paper On Polypharmacyefj02jba100% (1)
- Drug Normalisation DissertationDocument8 pagesDrug Normalisation DissertationUK100% (1)
- Dissertation On Prescription Drug AbuseDocument8 pagesDissertation On Prescription Drug AbuseWriteMyPaperForMeCheapAlbuquerque100% (1)
- Foster Kids More Likely To Receive 2 or More Antipsychotics: Expert Says Findings Raise A Red FlagDocument11 pagesFoster Kids More Likely To Receive 2 or More Antipsychotics: Expert Says Findings Raise A Red FlagGerly BallesterosNo ratings yet
- International Research Journal of PharmacyDocument5 pagesInternational Research Journal of PharmacyKoko DandashNo ratings yet
- Polypharmacy: in Older Adults at HomeDocument12 pagesPolypharmacy: in Older Adults at HomenellyNo ratings yet
- Journal 4Document17 pagesJournal 4Kimmy ChuNo ratings yet
- Adherence TheoriesDocument6 pagesAdherence TheoriesmakmgmNo ratings yet
- Antipsychotic Long Acting InjectionsDocument7 pagesAntipsychotic Long Acting InjectionsVoNda AprilianiNo ratings yet
- Research EssayDocument10 pagesResearch Essayapi-461330362No ratings yet
- Pharmaceutical Representatives: An Evidence-Based Review With Suggested Guidelines For ClerkshipsDocument5 pagesPharmaceutical Representatives: An Evidence-Based Review With Suggested Guidelines For Clerkshipsahmed22gouda22No ratings yet
- PolypharmacyDocument4 pagesPolypharmacyJeffrey Tan100% (1)
- Pharmacists Final CindidavisDocument7 pagesPharmacists Final Cindidavisapi-250612122No ratings yet
- Bila Pasien Tidak MampuDocument3 pagesBila Pasien Tidak MampuAndri FerdianNo ratings yet
- Research Papers On Prescription Drug AbuseDocument6 pagesResearch Papers On Prescription Drug Abusejsmyxkvkg100% (1)
- 18 Gouri Et AlDocument6 pages18 Gouri Et AleditorijmrhsNo ratings yet
- Geriatric PolypharmacyDocument6 pagesGeriatric PolypharmacyAnn DahngNo ratings yet
- Salud PublicaDocument21 pagesSalud PublicaJorge DiazNo ratings yet
- Cannabis For Symptom Management in Older Adults - 2020Document19 pagesCannabis For Symptom Management in Older Adults - 2020Carlos Ferrete JuniorNo ratings yet
- Medicine: Evidence BasedDocument2 pagesMedicine: Evidence BasedAustėjaVaičiulevičiūtėNo ratings yet
- Literature Review On Prescription Drug AbuseDocument8 pagesLiterature Review On Prescription Drug Abusejwuajdcnd100% (1)
- Barnes 2004 Complementary UseDocument18 pagesBarnes 2004 Complementary UseAntonio MoreiraNo ratings yet
- English 101 Annotated BiblographyDocument15 pagesEnglish 101 Annotated Biblographyapi-434255074No ratings yet
- Tassell, Pharmd Joanne Lafleur, Pharmd, MSPH 2010: Krzesinski JM Krzesinski FDocument10 pagesTassell, Pharmd Joanne Lafleur, Pharmd, MSPH 2010: Krzesinski JM Krzesinski FyehndNo ratings yet
- Factors Associated With Medication Adherence in Elderly Retired Outpatients in São Paulo, BrazilDocument10 pagesFactors Associated With Medication Adherence in Elderly Retired Outpatients in São Paulo, BrazilNelson Carvas JrNo ratings yet
- Patientsare Unwilling To Accept Physicians Decisions To Use Particular Medications. A Growing ProportionDocument2 pagesPatientsare Unwilling To Accept Physicians Decisions To Use Particular Medications. A Growing ProportionTSURAYYA ZAKIYYAHNo ratings yet
- Literature Review On PolypharmacyDocument5 pagesLiterature Review On Polypharmacyfuhukuheseg2100% (1)
- Normalisation of Drugs DissertationDocument8 pagesNormalisation of Drugs DissertationWriteMyPaperCanada100% (1)
- Research Papers On Clinical PharmacyDocument6 pagesResearch Papers On Clinical Pharmacyaflbrtdar100% (1)
- Prescription Drugs Abuse Research PaperDocument5 pagesPrescription Drugs Abuse Research Paperhubegynowig3100% (1)
- Prevalence of Self-Medication Practices and Its Associated Factors in Rural Bengaluru, Karnataka, IndiaDocument6 pagesPrevalence of Self-Medication Practices and Its Associated Factors in Rural Bengaluru, Karnataka, IndiaVijaya RaniNo ratings yet
- How To Improve Patient Compliance With Medication - IRXDocument4 pagesHow To Improve Patient Compliance With Medication - IRXShanza WaheedNo ratings yet
- Farmacología en AncianosDocument13 pagesFarmacología en AncianosGisselle RodriguezNo ratings yet
- Tanaman HerbalDocument134 pagesTanaman Herbalwhy_smart03No ratings yet
- Reducing Inappropriate Polypharmacy The Process of DeprescribingDocument8 pagesReducing Inappropriate Polypharmacy The Process of DeprescribingThiago SartiNo ratings yet
- Improving Primary Care in Rural Alabama With A Pharmacy InitiativeDocument7 pagesImproving Primary Care in Rural Alabama With A Pharmacy InitiativeBasilharbi HammadNo ratings yet
- Abstract 8Document1 pageAbstract 8michaelb4No ratings yet
- Over-the-Counter Medication Use, Perceived Safety, and Decision-Making Behaviors in Pregnant WomenDocument14 pagesOver-the-Counter Medication Use, Perceived Safety, and Decision-Making Behaviors in Pregnant WomenMaunish PatelNo ratings yet
- Literature Review Medication Safety in AustraliaDocument5 pagesLiterature Review Medication Safety in Australiaea7gpeqm100% (1)
- Geriatrics I-FDocument18 pagesGeriatrics I-FrxdocNo ratings yet
- Factors Associated With Patients' Incomplete Understanding of PrescriptionsDocument9 pagesFactors Associated With Patients' Incomplete Understanding of PrescriptionsCanlas John MichaelNo ratings yet
- Er UpdateDocument1 pageEr UpdateRiza AbinalNo ratings yet
- Final1 1Document23 pagesFinal1 1sheena LesNo ratings yet
- Handbook of Nonprescription Drugs Quick Reference 1st Edition Ebook PDFDocument62 pagesHandbook of Nonprescription Drugs Quick Reference 1st Edition Ebook PDFjeffrey.stanton398100% (53)
- Lack of Patient CounselingDocument15 pagesLack of Patient CounselingAzan AhmadNo ratings yet
- Interventions in Nursing HomesDocument18 pagesInterventions in Nursing Homesvictory818No ratings yet
- Family Medicine Thesis TopicsDocument4 pagesFamily Medicine Thesis Topicspatriciaadamsjackson100% (1)
- Prescription Drug Abuse ThesisDocument5 pagesPrescription Drug Abuse Thesistpynawfld100% (2)
- Reducing Medication Administration Errors in The Gerontology PopulationDocument8 pagesReducing Medication Administration Errors in The Gerontology PopulationNicholas GichukiNo ratings yet
- 5 Lessons To Learn From The Nocebo EffectDocument2 pages5 Lessons To Learn From The Nocebo Effecttami estradaNo ratings yet
- Bookshelf NBK43772Document13 pagesBookshelf NBK43772moraes.carvalho.fredNo ratings yet
- User's Guide to Natural Therapies for Cancer Prevention and ControlFrom EverandUser's Guide to Natural Therapies for Cancer Prevention and ControlRating: 5 out of 5 stars5/5 (1)
- Pharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceFrom EverandPharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceRating: 3 out of 5 stars3/5 (1)
- Lab 5-Nguyen The Huu-SE1841Document4 pagesLab 5-Nguyen The Huu-SE1841nguyenthehuu2003No ratings yet
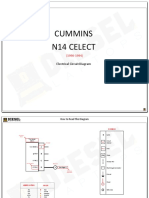
- Cummins N14 Celect: Electrical Circuit DiagramDocument9 pagesCummins N14 Celect: Electrical Circuit DiagramDiego Lira100% (1)
- Office Order 07 of 2024 - 240101 - 200240Document32 pagesOffice Order 07 of 2024 - 240101 - 200240Hemant SinhmarNo ratings yet
- Revise Chap 12Document14 pagesRevise Chap 12RACHEL DAMALERIONo ratings yet
- DF5.8.1 Formability Training ManualDocument107 pagesDF5.8.1 Formability Training ManualkillimakilliNo ratings yet
- EALS - Oral Recitation QuestionsDocument2 pagesEALS - Oral Recitation QuestionsClaudene GellaNo ratings yet
- SAP - MM Introduction & Enterprise StructureDocument40 pagesSAP - MM Introduction & Enterprise Structuresruthimannam28No ratings yet
- Topic: Functions and ArraysDocument16 pagesTopic: Functions and ArraysSandeep DwivediNo ratings yet
- Implen Smart Grid ColombiaDocument6 pagesImplen Smart Grid ColombiapabloNo ratings yet
- Case Study: Distributed Scrum Project For Dutch RailwaysDocument7 pagesCase Study: Distributed Scrum Project For Dutch RailwaysDark LordNo ratings yet
- Evaluating The Potential Impact of Ototoxicant Exposure On Worker HealthDocument17 pagesEvaluating The Potential Impact of Ototoxicant Exposure On Worker Healthani putkaradzeNo ratings yet
- Universal Mechanical Tester: Innovation With IntegrityDocument4 pagesUniversal Mechanical Tester: Innovation With IntegrityDlair Ramadan0% (1)
- CPF Form 4BDocument2 pagesCPF Form 4BBala SelvakumarNo ratings yet
- Oracle ERP Data SheetDocument2 pagesOracle ERP Data Sheetvinoth4iNo ratings yet
- 190 Service Manual - Aspire 1450Document107 pages190 Service Manual - Aspire 1450Soporte Tecnico Buenos AiresNo ratings yet
- Suntay vs. CA Case DigestDocument3 pagesSuntay vs. CA Case DigestCaitlin Kintanar100% (2)
- ElastomerDocument3 pagesElastomersiswoutNo ratings yet
- Case Accounting - Air Asia BerhadDocument15 pagesCase Accounting - Air Asia BerhadWahyutri IndonesiaNo ratings yet
- Lesson 4a. Officer-Violator RelationshipDocument3 pagesLesson 4a. Officer-Violator RelationshipalliahnahNo ratings yet
- Lemon BatteryDocument6 pagesLemon BatteryMohammed AsifNo ratings yet
- Comparative Study of Public and Private Telecom Wireless Services in IndiaDocument4 pagesComparative Study of Public and Private Telecom Wireless Services in Indiajonny bravoNo ratings yet
- Vinay 1 Final-Converted-Converted-Merged - 1 PDFDocument53 pagesVinay 1 Final-Converted-Converted-Merged - 1 PDFVinay GajulaNo ratings yet
- Operating Instructions Accessories Component Parts DC Pro Demag Chain HoistsDocument144 pagesOperating Instructions Accessories Component Parts DC Pro Demag Chain HoistsAristideNo ratings yet
- Digital Marketing Strategy and Marketing Mix UploadDocument39 pagesDigital Marketing Strategy and Marketing Mix UploadAmisha LalNo ratings yet
- Solved - For The Three-Bus System Whose Ybus Is Given, Calculate...Document6 pagesSolved - For The Three-Bus System Whose Ybus Is Given, Calculate...ZabeehullahmiakhailNo ratings yet
- Design Change Connexion - ECN - RegisterDocument3 pagesDesign Change Connexion - ECN - RegisterMbalekelwa MpembeNo ratings yet
- How To Avoid Negative Float in P6 Time ScheduleDocument2 pagesHow To Avoid Negative Float in P6 Time SchedulevouphNo ratings yet
- Appendix C Steam TablesDocument8 pagesAppendix C Steam TablesWin Alfalah Nasution100% (1)