Download as pdf or txt
You might also like
- Limatations in OrthodonticsDocument122 pagesLimatations in Orthodonticsavanthika krishnarajNo ratings yet
- Anatomy AETCOM Questions and Answers SR. NO. Subtopic Competency Number Name Description Xiv Aetcom Core/ YDocument8 pagesAnatomy AETCOM Questions and Answers SR. NO. Subtopic Competency Number Name Description Xiv Aetcom Core/ YAyesha Singh100% (3)
- PR10 Counseling Individual PtsDocument41 pagesPR10 Counseling Individual PtsAhmad Al-RusasiNo ratings yet
- Client-Centered TherapyDocument22 pagesClient-Centered TherapyEarl ConeseNo ratings yet
- Examination & Diagnosis of Edentulous Patients: Presented By: Dr. Jehan Dordi 1 Yr. MdsDocument159 pagesExamination & Diagnosis of Edentulous Patients: Presented By: Dr. Jehan Dordi 1 Yr. MdsAkanksha MahajanNo ratings yet
- Diagnosis and Treatment Planning - Removable Partial Denture Part-1Document38 pagesDiagnosis and Treatment Planning - Removable Partial Denture Part-1Ahmed AliNo ratings yet
- Chapter 1 DiagnosisDocument32 pagesChapter 1 DiagnosisMohamed KilaniNo ratings yet
- Diagnosis and Treatment PlanningDocument46 pagesDiagnosis and Treatment Planningsiddu76100% (2)
- Case History and DiagnosisDocument306 pagesCase History and DiagnosismmNo ratings yet
- 2 - Diagnosis and Treatment PlanningDocument55 pages2 - Diagnosis and Treatment Planningamoon almNo ratings yet
- Savio Case Presentation Format 2024Document156 pagesSavio Case Presentation Format 2024Jeamine Talaver PalenciaNo ratings yet
- Diagnosis and Treatment Planning Part 1Document12 pagesDiagnosis and Treatment Planning Part 1Shahrukh ali khanNo ratings yet
- Diagnosis and Treatment Plan of An Edentulous MouthDocument53 pagesDiagnosis and Treatment Plan of An Edentulous MouthKayode Ibitoye100% (5)
- Approach To The Evaluation of A PatientDocument7 pagesApproach To The Evaluation of A PatienthithNo ratings yet
- Diagnosis and Treatment PlanningDocument66 pagesDiagnosis and Treatment PlanningVincent SerNo ratings yet
- Patient Encounter, Medical Chart, Interviewing and Respiratory HistoryDocument62 pagesPatient Encounter, Medical Chart, Interviewing and Respiratory HistoryggNo ratings yet
- Glick 2021Document18 pagesGlick 2021dra.claudiamaria.tiNo ratings yet
- Sample Questions For NZREX ClinicalDocument18 pagesSample Questions For NZREX ClinicalAbs KarimiNo ratings yet
- History Taking, Treatment Planning 1Document117 pagesHistory Taking, Treatment Planning 1bhamaNo ratings yet
- Communication SkillsDocument42 pagesCommunication Skillsdoctor mizoNo ratings yet
- Course Guide: Year 3Document52 pagesCourse Guide: Year 3Elise ChuaNo ratings yet
- Pom MidtermsDocument692 pagesPom MidtermsGwyneth MendozaNo ratings yet
- Nursing Assessment by ObunadikeDocument25 pagesNursing Assessment by Obunadikefeljennie2000No ratings yet
- Understanding The Psychology of Geriatric Edentulous PatientsDocument5 pagesUnderstanding The Psychology of Geriatric Edentulous PatientsAna RahăuNo ratings yet
- 14 Essentials To Assessment and Care PlanMT2013!08!018-BRODATY - 0Document9 pages14 Essentials To Assessment and Care PlanMT2013!08!018-BRODATY - 0Danielcc Lee100% (1)
- Patients InterviewDocument73 pagesPatients InterviewCantoria Willa 2 PTNo ratings yet
- Documentation and Medical RecordsDocument14 pagesDocumentation and Medical Recordsdoctor mizoNo ratings yet
- Physician - Patient RelationshipDocument28 pagesPhysician - Patient Relationshipmohammed barwaryNo ratings yet
- Stirling Et Al 2007 Elective Orthognathic Treatment Decision Making A Survey of Patient Reasons and ExperiencesDocument15 pagesStirling Et Al 2007 Elective Orthognathic Treatment Decision Making A Survey of Patient Reasons and ExperiencesPeter SerNo ratings yet
- Case HistoryDocument68 pagesCase HistoryShruti GargNo ratings yet
- SAQs VariousDocument16 pagesSAQs Variousapi-26291651100% (3)
- History, Diagnosis and Treatement Planning in Removable Partial DenturesDocument96 pagesHistory, Diagnosis and Treatement Planning in Removable Partial DenturesPriya BagalNo ratings yet
- Introduction To Pedi PTDocument36 pagesIntroduction To Pedi PTTitanium TssNo ratings yet
- ART Adherence: Small TalksDocument12 pagesART Adherence: Small TalksShondiandNo ratings yet
- Diagnosis & Treatment Planning For Edentulous PatientDocument9 pagesDiagnosis & Treatment Planning For Edentulous PatientChhavi sharmaNo ratings yet
- Dashboard Library Study Plans Qbank Analysis Account Help Center & Legal InfoDocument42 pagesDashboard Library Study Plans Qbank Analysis Account Help Center & Legal InfoGauri SurnerNo ratings yet
- Understanding The Psychology of Geriatric Edentulous PatientsDocument5 pagesUnderstanding The Psychology of Geriatric Edentulous PatientsAlvaro LeónNo ratings yet
- NCM112 Prelim ReviewerDocument7 pagesNCM112 Prelim ReviewerKrame G.No ratings yet
- Pak Orthod J 2012 4 2 44 47Document4 pagesPak Orthod J 2012 4 2 44 47Jose PerezNo ratings yet
- Patient History: Prof. Hoda ElguindyDocument14 pagesPatient History: Prof. Hoda Elguindyyahia salah100% (1)
- MD in General Medicine (Revised)Document28 pagesMD in General Medicine (Revised)Mayank ParasharNo ratings yet
- Common Cardiopulmonary SymptomsDocument73 pagesCommon Cardiopulmonary SymptomsDharlyn MungcalNo ratings yet
- Diagnosis: Risk Factors For Partially Edentulous PatientDocument8 pagesDiagnosis: Risk Factors For Partially Edentulous PatientnjucyNo ratings yet
- AUA Clinical Curriculum 2013Document15 pagesAUA Clinical Curriculum 2013Ogine L. LoNo ratings yet
- Propaedeutics of intеrnаl medicine as аn introduction to the clinic of internal medicine. Questioning and physical examination of the patient. Еthical and deontological aspectsDocument42 pagesPropaedeutics of intеrnаl medicine as аn introduction to the clinic of internal medicine. Questioning and physical examination of the patient. Еthical and deontological aspectsDonia HnainiaNo ratings yet
- Therapy-I: Fuad A. Mohammed Clinical Pharmacist & LecturerDocument102 pagesTherapy-I: Fuad A. Mohammed Clinical Pharmacist & LecturerGalataa MuktaarNo ratings yet
- Cognitive Impairment Evaluation and ManagementDocument19 pagesCognitive Impairment Evaluation and ManagementSAMUEL MARIN FUQUENENo ratings yet
- Week 2 - Day 1 - Introduction To Clinical Medicine IDocument54 pagesWeek 2 - Day 1 - Introduction To Clinical Medicine INsikan GabrielNo ratings yet
- Diagnosis of CDDocument79 pagesDiagnosis of CDAbdelrahman GalalNo ratings yet
- Diagnosis and Treatment Planning of CD PatientsDocument95 pagesDiagnosis and Treatment Planning of CD PatientsAnjana ThomasNo ratings yet
- K3 - Kuliah 4 Diagnosis-TX-planningDocument19 pagesK3 - Kuliah 4 Diagnosis-TX-planningilhamNo ratings yet
- MacloedDocument21 pagesMacloedramadoy454No ratings yet
- Screening For Aod Use NursingDocument31 pagesScreening For Aod Use NursingSaqib Ur Rehman KarlalNo ratings yet
- Diagnosis and Treatment Plan of CDDocument12 pagesDiagnosis and Treatment Plan of CDIbrahim HashimiNo ratings yet
- De-Briefing of The GP Visit and Impact of Social IssuesDocument29 pagesDe-Briefing of The GP Visit and Impact of Social IssuesAshley LewisNo ratings yet
- Finding the Path in Alzheimer’s Disease: Early Diagnosis to Ongoing Collaborative CareFrom EverandFinding the Path in Alzheimer’s Disease: Early Diagnosis to Ongoing Collaborative CareNo ratings yet
- Treatment Planning in Restorative Dentistry and Implant ProsthodonticsFrom EverandTreatment Planning in Restorative Dentistry and Implant ProsthodonticsNo ratings yet
- Dynamic Navigation in Dental Implantology: The Influence of Surgical Experience On Implant Placement Accuracy and Operating Time. An in Vitro StudyDocument9 pagesDynamic Navigation in Dental Implantology: The Influence of Surgical Experience On Implant Placement Accuracy and Operating Time. An in Vitro StudySahana RangarajanNo ratings yet
- Mandibular MovementDocument56 pagesMandibular MovementSahana RangarajanNo ratings yet
- Clinical Report Rehabilitation of Maxillary Surgical Defect With A Cast Partial Denture ObturatorDocument4 pagesClinical Report Rehabilitation of Maxillary Surgical Defect With A Cast Partial Denture ObturatorSahana RangarajanNo ratings yet
- Support in Complete DentureDocument16 pagesSupport in Complete DentureSahana RangarajanNo ratings yet
- Support in Complete DentureDocument30 pagesSupport in Complete DentureSahana Rangarajan100% (2)
- Different Types of Tooth PreparationDocument56 pagesDifferent Types of Tooth PreparationSahana Rangarajan100% (1)
- Factors Affecting Shade of All Ceramic Restorations - A Literature ReviewDocument8 pagesFactors Affecting Shade of All Ceramic Restorations - A Literature ReviewSahana RangarajanNo ratings yet
- Mouth Guards in Dentistry-A Review: September 2018Document6 pagesMouth Guards in Dentistry-A Review: September 2018Sahana RangarajanNo ratings yet
- Fulltext - Jda v5 Id1107Document3 pagesFulltext - Jda v5 Id1107Sahana RangarajanNo ratings yet
- Frankel Appliance Certified Fixed Orthodontic Courses by Indian Dental AcademyDocument76 pagesFrankel Appliance Certified Fixed Orthodontic Courses by Indian Dental AcademySahana RangarajanNo ratings yet
- 7 Shreeprada Dash IJPHRDDecember 2018 IssueDocument7 pages7 Shreeprada Dash IJPHRDDecember 2018 IssueSahana RangarajanNo ratings yet
- Finishing and Polishing Agents: - Presented by DR Arpita DuttaDocument89 pagesFinishing and Polishing Agents: - Presented by DR Arpita DuttaSahana RangarajanNo ratings yet
- A Hollow Bulb Obturator For Maxillary Resection in A Completely Edentulous PatientDocument6 pagesA Hollow Bulb Obturator For Maxillary Resection in A Completely Edentulous PatientSahana RangarajanNo ratings yet
- 6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothDocument6 pages6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothSahana RangarajanNo ratings yet
- 7 RetainerinorthodonticsDocument6 pages7 RetainerinorthodonticsSahana RangarajanNo ratings yet
- 3D Printing Industry Roadmap - India (Aerospace) Summit DocumentDocument19 pages3D Printing Industry Roadmap - India (Aerospace) Summit DocumentSahana RangarajanNo ratings yet
- Sauser 1957Document9 pagesSauser 1957Sahana RangarajanNo ratings yet
- Long-Term Follow-Up of Maxillary Fixed Retention: Survival Rate and Periodontal HealthDocument7 pagesLong-Term Follow-Up of Maxillary Fixed Retention: Survival Rate and Periodontal HealthSahana RangarajanNo ratings yet
- Review: Types of Finish Lines or Gingival Margins Intooth PreparationDocument6 pagesReview: Types of Finish Lines or Gingival Margins Intooth PreparationSahana RangarajanNo ratings yet
- Significance of Facebow For Dental RestorationsDocument5 pagesSignificance of Facebow For Dental RestorationsSahana RangarajanNo ratings yet
- Elegant Galaxy Background Breakthrough by SlidesgoDocument48 pagesElegant Galaxy Background Breakthrough by SlidesgoSahana RangarajanNo ratings yet
- Gothic Arch TrachingDocument7 pagesGothic Arch TrachingSahana RangarajanNo ratings yet
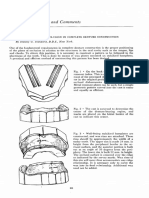
- Cases and Comments: by Stanley G. Standard, D.D.S., New YorkDocument3 pagesCases and Comments: by Stanley G. Standard, D.D.S., New YorkSahana RangarajanNo ratings yet
- Prosthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerDocument6 pagesProsthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerSahana RangarajanNo ratings yet
- Tocilizumab CovidDocument15 pagesTocilizumab CovidAponte MaríaNo ratings yet
- 01 Pharmacology PST 05-1Document319 pages01 Pharmacology PST 05-1ambroceNo ratings yet
- Ethics Applied in NursingDocument3 pagesEthics Applied in NursingGil GanibanNo ratings yet
- Mini Implants in Orthodontics: Review ArticleDocument5 pagesMini Implants in Orthodontics: Review Articledrzana78No ratings yet
- 148 1 Pmss MeritList 2022-23Document89 pages148 1 Pmss MeritList 2022-23Spark FootwearNo ratings yet
- Homoeopathic Intervention in PsoriasisDocument25 pagesHomoeopathic Intervention in PsoriasisAnil Subhash RathodNo ratings yet
- Poster Papostblo Aguilar 3Document1 pagePoster Papostblo Aguilar 3Juan Pablo AguilarNo ratings yet
- Outcomes of Dogs Undergoing Limb Amputation, Owner Satisfaction With Limb Amputation Procedures, and Owner Perceptions Regarding Postsurgical Adaptation: 64 Cases (2005-2012)Document7 pagesOutcomes of Dogs Undergoing Limb Amputation, Owner Satisfaction With Limb Amputation Procedures, and Owner Perceptions Regarding Postsurgical Adaptation: 64 Cases (2005-2012)William ChandlerNo ratings yet
- Ic VeastDocument11 pagesIc VeastReza EbookNo ratings yet
- Operating RoomDocument9 pagesOperating RoomMarie Ashley CasiaNo ratings yet
- Lec 10 MidtermsDocument1 pageLec 10 MidtermsMitzi AngelaNo ratings yet
- Functional Abdominal Cramping Pain Expert Practical Guidance 2022Document9 pagesFunctional Abdominal Cramping Pain Expert Practical Guidance 2022Mohamad MostafaNo ratings yet
- Emhj 16 1 2010Document134 pagesEmhj 16 1 2010Muhammad SaeedNo ratings yet
- The Identification and Prevention of Cybercrime in The Healthcare IndustryDocument10 pagesThe Identification and Prevention of Cybercrime in The Healthcare IndustryImran AlamNo ratings yet
- Knowledge, Attitude and Awareness of Intraoral Radiographic Imaging Techniques Among Dental Students Across Chennai A Questionnaire StudyDocument6 pagesKnowledge, Attitude and Awareness of Intraoral Radiographic Imaging Techniques Among Dental Students Across Chennai A Questionnaire StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- BOSIET With EBS Course Descriptor & Joinning InstructionDocument5 pagesBOSIET With EBS Course Descriptor & Joinning InstructionNisamudheenNo ratings yet
- Voucher TopamaxDocument2 pagesVoucher Topamaxapi-3738852100% (1)
- Endorsement KardexDocument3 pagesEndorsement Kardexapi-19780865100% (2)
- Evolving Regulatory Perspectives On Digital Health Technologies For Medicinal Product DevelopmentDocument11 pagesEvolving Regulatory Perspectives On Digital Health Technologies For Medicinal Product DevelopmentNot 8No ratings yet
- Prescription WritingDocument28 pagesPrescription WritingEshana AryaNo ratings yet
- Family Nursing and Family Health Nursing ProcessDocument92 pagesFamily Nursing and Family Health Nursing ProcessKailash NagarNo ratings yet
- Case 4 HTN CVDDocument8 pagesCase 4 HTN CVDapi-491807608No ratings yet
- Tugas 1 - Nazratul Adzkia (2007110083) - Kelas CDocument133 pagesTugas 1 - Nazratul Adzkia (2007110083) - Kelas CNazratul AdzkiaNo ratings yet
- Study Buddies 1080Document12 pagesStudy Buddies 1080Greg SJNo ratings yet
- Buy AmoxicillinDocument1 pageBuy Amoxicillinanon_823821469No ratings yet
- Chinmay Pandya ProfileDocument1 pageChinmay Pandya Profileice_fire0073075No ratings yet
- MCN Questionnaire DraftDocument8 pagesMCN Questionnaire DraftJenny AjocNo ratings yet
- Unit 3 Module Networking TemplateDocument17 pagesUnit 3 Module Networking Templateapi-562162979No ratings yet
- Asian Hospital ResearchDocument9 pagesAsian Hospital ResearchTrincyNo ratings yet