Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Yu-Chen Lee PHYS20100 - ContinuousAssessment - Assignment#3 - WorksheetDocument5 pagesYu-Chen Lee PHYS20100 - ContinuousAssessment - Assignment#3 - Worksheet李雨宸No ratings yet
- Director of Pharmacy, Clinical PharmacistDocument3 pagesDirector of Pharmacy, Clinical Pharmacistapi-77860855No ratings yet
- Volume 5 Over-the-Counter ProductsDocument478 pagesVolume 5 Over-the-Counter ProductsDikri Fadhlurrohman100% (2)
- Synthesis, Characterization and Biocompatibility Evaluation of Novel Chitosan Lipid Micro-Systems For Modified Release of Diclofenac SodiumDocument22 pagesSynthesis, Characterization and Biocompatibility Evaluation of Novel Chitosan Lipid Micro-Systems For Modified Release of Diclofenac SodiumpelinNo ratings yet
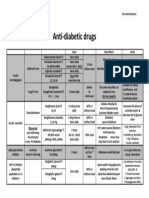
- Anti Diabetic DrugsDocument1 pageAnti Diabetic DrugsWael hadNo ratings yet
- Obesity and Anticipated Difficult Airway - A Comprehensive Approach With Videolaryngoscopy, Ramp Position, Sevoflurane and Opioid Free AnaesthesiaDocument8 pagesObesity and Anticipated Difficult Airway - A Comprehensive Approach With Videolaryngoscopy, Ramp Position, Sevoflurane and Opioid Free AnaesthesiaIJAR JOURNALNo ratings yet
- Resuscitation MedicationDocument1 pageResuscitation MedicationDen SinyoNo ratings yet
- Pharma Prelim Assignment 1 - Pharmacodynamics..Document2 pagesPharma Prelim Assignment 1 - Pharmacodynamics..Kimberly Wyne SantosNo ratings yet
- Leptomeningeal DiseaseDocument17 pagesLeptomeningeal DiseaseForem ZayneNo ratings yet
- India - Pharmaceuticals MarketDocument14 pagesIndia - Pharmaceuticals MarketNaveena ShreeNo ratings yet
- Antibacterial Activity of Inter Node and Leaves of Mentha Arvensis Yerba Buena Againts Staphyloccocus Epidermidis CheckedDocument5 pagesAntibacterial Activity of Inter Node and Leaves of Mentha Arvensis Yerba Buena Againts Staphyloccocus Epidermidis CheckedWynonnaNo ratings yet
- Antibiotic Classification & Mechanism - Basic Science - OrthobulletsDocument9 pagesAntibiotic Classification & Mechanism - Basic Science - OrthobulletsHossam Elden Helmy HaridyNo ratings yet
- Bipolar Disorder PDFDocument108 pagesBipolar Disorder PDFMaica LectanaNo ratings yet
- Protocol Jco.19.03355Document99 pagesProtocol Jco.19.03355malakmounirNo ratings yet
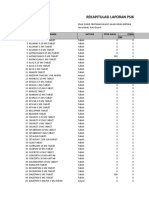
- Rekapitulasi Laporan Psikotropika: NO Nama Satuan Stok Awal Pemasukan PBFDocument9 pagesRekapitulasi Laporan Psikotropika: NO Nama Satuan Stok Awal Pemasukan PBFlarasNo ratings yet
- UnasynDocument3 pagesUnasynianecunar100% (4)
- Ebook Fundamentals of Pharmacognosy and Phytotherapy PDF Full Chapter PDFDocument59 pagesEbook Fundamentals of Pharmacognosy and Phytotherapy PDF Full Chapter PDFmary.rainey124100% (35)
- Preformulation - A Foundation For PDFDocument4 pagesPreformulation - A Foundation For PDFSamer OdehNo ratings yet
- Photosensitive Diseases: 1. Solar Dermatitis, SunburnDocument8 pagesPhotosensitive Diseases: 1. Solar Dermatitis, SunburnOliver RomaineNo ratings yet
- Sector BiotechDocument109 pagesSector BiotechoptisearchNo ratings yet
- Legalization of Marijuana in The PhilippinesDocument12 pagesLegalization of Marijuana in The PhilippinesJenny ChavezNo ratings yet
- AceclofenacDocument2 pagesAceclofenacfullname11No ratings yet
- Vagus Nerve Neuropathy Related To SARS COV-2 InfectionDocument3 pagesVagus Nerve Neuropathy Related To SARS COV-2 Infectionmpm8471No ratings yet
- A Prolonged Release Parenteral Drug Delivery SystemDocument11 pagesA Prolonged Release Parenteral Drug Delivery SystemronnymcmNo ratings yet
- Presenter-Dr. Tesita SherryDocument109 pagesPresenter-Dr. Tesita SherryTesitaNo ratings yet
- Bronchodilators and Other Respiratory AgentsDocument61 pagesBronchodilators and Other Respiratory Agentsone_nd_onlyuNo ratings yet
- Essential TremorDocument8 pagesEssential Tremordeepak_anvekarNo ratings yet
- Limnophila (Scrophulariaceae) Chemical and Pharmaceutical Aspects - An UpdateDocument14 pagesLimnophila (Scrophulariaceae) Chemical and Pharmaceutical Aspects - An UpdateKhánh Linh LêNo ratings yet
- Turnaround Time - Project Reupdated PDFDocument41 pagesTurnaround Time - Project Reupdated PDFDhanashree DalviNo ratings yet
- Orca Share Media1677034827919 7033993886882488759Document5 pagesOrca Share Media1677034827919 7033993886882488759GayleNo ratings yet