Download as pdf or txt
You might also like
- 5 - Introduction To Communicable DiseaseDocument32 pages5 - Introduction To Communicable DiseaseGetom Ngukir100% (1)
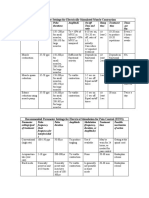
- Parameter Settings For Electrically Stimulated Muscle ContractionDocument3 pagesParameter Settings For Electrically Stimulated Muscle Contractionpallen100% (5)
- (MI) Patient Profile DatabaseDocument11 pages(MI) Patient Profile DatabaseMurathi Mwangi100% (1)
- FNCPDocument1 pageFNCPkristel_nicole18yahoNo ratings yet
- Gluco Induced OsteopDocument13 pagesGluco Induced Osteopmatheus galvãoNo ratings yet
- Capture The Fracture - Use of Bone Turnover MarkerDocument7 pagesCapture The Fracture - Use of Bone Turnover MarkergusdeNo ratings yet
- Pathophysiology of Bone MetastasesDocument5 pagesPathophysiology of Bone MetastasesdyahNo ratings yet
- Bone Disease in Chronic Kidney Disease and Kidney TransplantDocument27 pagesBone Disease in Chronic Kidney Disease and Kidney TransplantBhanu KumarNo ratings yet
- Group Ii: Harni Sartika Sandrawati Nangsih S. Slamet Rusman Hasanuddin Yusnita UsmanDocument17 pagesGroup Ii: Harni Sartika Sandrawati Nangsih S. Slamet Rusman Hasanuddin Yusnita UsmanYusnitaUsmanNo ratings yet
- Glucocorticoid-Induced Osteoporosis: Pathophysiology and TherapyDocument10 pagesGlucocorticoid-Induced Osteoporosis: Pathophysiology and TherapyMuhammad Isnaini ZuhriNo ratings yet
- L36 - Back Pain in An Elderly Woman - 2012Document46 pagesL36 - Back Pain in An Elderly Woman - 2012edwinfy123No ratings yet
- ESO Spesifik Pada Organ SpesifikDocument44 pagesESO Spesifik Pada Organ SpesifikLidwina Margaretha LakaNo ratings yet
- Arthrosis of KneeDocument30 pagesArthrosis of Kneebiomechy oktomalioputriNo ratings yet
- Arthrosis of KneeDocument30 pagesArthrosis of Kneebiomechy oktomalioputriNo ratings yet
- Effects of Microgravity On Bone DensityDocument9 pagesEffects of Microgravity On Bone DensityAffan Nadeem QaziNo ratings yet
- OsteoporosisDocument13 pagesOsteoporosisclaudyNo ratings yet
- Denosumab: An Emerging Therapy in Pediatric Bone Disorders: Pediatrics (L Ward and E Imel, Section Editors)Document10 pagesDenosumab: An Emerging Therapy in Pediatric Bone Disorders: Pediatrics (L Ward and E Imel, Section Editors)Dita Putri DamayantiNo ratings yet
- Biology of BoneDocument30 pagesBiology of BoneChris Jardine LiNo ratings yet
- Pathophysiology-Pathomechanics Dan Penegakan Diagnosis OsteoporosisDocument90 pagesPathophysiology-Pathomechanics Dan Penegakan Diagnosis Osteoporosissingle_ladyNo ratings yet
- Fimmu 13 1005665Document14 pagesFimmu 13 1005665sopha seyhaNo ratings yet
- OsteoporosisDocument35 pagesOsteoporosisFarida Abo ElmagdNo ratings yet
- Pathogenesis of Osteoporosis 2: Cli Ord J. RosenDocument13 pagesPathogenesis of Osteoporosis 2: Cli Ord J. RosenRonald TejoprayitnoNo ratings yet
- Nutritional Zinc Plays A Pivotal Role in Bone Health and Osteoporosis PreventionDocument14 pagesNutritional Zinc Plays A Pivotal Role in Bone Health and Osteoporosis PreventionDewi HenssaNo ratings yet
- Adverse Effects of Corticosteroids On BoneDocument6 pagesAdverse Effects of Corticosteroids On BoneDiego Rivas-VazquezNo ratings yet
- Effects of Glucosamine and Chondroitin Sulfate On Cartilage Metabolism in OA. Outlook On Other Nutrient Partners Especially Omega-3 Fatty AcidsDocument17 pagesEffects of Glucosamine and Chondroitin Sulfate On Cartilage Metabolism in OA. Outlook On Other Nutrient Partners Especially Omega-3 Fatty Acidsharvestmoon.harvestingtimeNo ratings yet
- Doosis KalsiumDocument8 pagesDoosis KalsiumNurul Kamilah SadliNo ratings yet
- Thiazolidinediones On PPARg The Roles in Bone RemoDocument9 pagesThiazolidinediones On PPARg The Roles in Bone RemoNguyễn Hoàng Thiên TânNo ratings yet
- Frontiers in Bioscience 4, d662-670, October 15, 1999Document9 pagesFrontiers in Bioscience 4, d662-670, October 15, 1999Aldo HoxhaNo ratings yet
- The Effect of Icariin On Bone Metabolism and Its Potential Clinical ApplicationDocument12 pagesThe Effect of Icariin On Bone Metabolism and Its Potential Clinical ApplicationBrenda MartinsNo ratings yet
- OsteoporosisDocument35 pagesOsteoporosisSanjeev MehtaNo ratings yet
- BP MecanismDocument14 pagesBP MecanismAdryana StefyNo ratings yet
- Normal Bone Formation and RemodelingDocument4 pagesNormal Bone Formation and RemodelingFernando AnibanNo ratings yet
- Secondary OsteoporosisDocument22 pagesSecondary OsteoporosisBenny Chris TantoNo ratings yet
- Update Osteoporosis Management (Listo)Document18 pagesUpdate Osteoporosis Management (Listo)Jossie AcuñaNo ratings yet
- Osseteointegration of Dental ImplantDocument24 pagesOsseteointegration of Dental ImplantFajar Kusuma Dwi KurniawanNo ratings yet
- 1042 FullDocument9 pages1042 Fulloki harisandiNo ratings yet
- Chondroprotective Effects of The Combination ChondroitinDocument9 pagesChondroprotective Effects of The Combination Chondroitincursotplo2021No ratings yet
- Regulatory Pathways Revealing New Approaches2008Document14 pagesRegulatory Pathways Revealing New Approaches2008Cami GutierrezNo ratings yet
- LID201112052004Document10 pagesLID201112052004Gia BảoNo ratings yet
- Pathophysiology of OsteoarthritisDocument3 pagesPathophysiology of OsteoarthritisHajar ToharNo ratings yet
- Non-Enzymatic Glycation of Bone Collagen Modifies Osteoclastic Activity and DifferentiationDocument28 pagesNon-Enzymatic Glycation of Bone Collagen Modifies Osteoclastic Activity and Differentiationdumboo21No ratings yet
- Yoon-Kyum Shin, Young Kwon Yoon, Kyung Bae Chung, Yumie Rhee, Sung-Rae ChoDocument6 pagesYoon-Kyum Shin, Young Kwon Yoon, Kyung Bae Chung, Yumie Rhee, Sung-Rae ChoRisky Ilona SaputraNo ratings yet
- Recent Advances in The Pathogenesis and Treatment of OsteoporosisDocument5 pagesRecent Advances in The Pathogenesis and Treatment of OsteoporosisAnil JohnNo ratings yet
- OSTEOPOROSISDocument39 pagesOSTEOPOROSISHapsari Wibawani 'winda'No ratings yet
- Secondary Osteoporosis - A Still Neglected ConditionDocument4 pagesSecondary Osteoporosis - A Still Neglected ConditionClaudiaGuerreroNo ratings yet
- Osteogenesi ImperfectaDocument8 pagesOsteogenesi ImperfectaAna Priscila RamirezNo ratings yet
- Tto de La Osteoporosis - 2020Document16 pagesTto de La Osteoporosis - 2020GilbertoNo ratings yet
- Bone Turnover Markers: Use in Fracture Prediction: Tatiane Vilaca, Fatma Gossiel, and Richard EastellDocument7 pagesBone Turnover Markers: Use in Fracture Prediction: Tatiane Vilaca, Fatma Gossiel, and Richard EastellPoramate PITAK-ARNNOPNo ratings yet
- Clinical Aspects, Pathology and Pathophysiology of OsteoarthritisDocument3 pagesClinical Aspects, Pathology and Pathophysiology of OsteoarthritisOscar NgNo ratings yet
- Metabolic Bone DiseaseDocument6 pagesMetabolic Bone Diseasekartini ciatawiNo ratings yet
- Bone Erosion Rheumatoid Arthritis Mechanisms Diagnosis&TreatmentDocument9 pagesBone Erosion Rheumatoid Arthritis Mechanisms Diagnosis&TreatmentMaría RodríguezNo ratings yet
- Bones & Joints Pathology 4thDocument8 pagesBones & Joints Pathology 4thlovelyc95No ratings yet
- Osteoporosis After TransplantationDocument8 pagesOsteoporosis After TransplantationDennis KabuchwaNo ratings yet
- Nihms-1007745 TNF BoneDocument15 pagesNihms-1007745 TNF BoneAndyka YasaNo ratings yet
- Prof. Dr. Hazem Abd El-Azeem Professor of Orthopaedic Surgery Cairo UniversityDocument47 pagesProf. Dr. Hazem Abd El-Azeem Professor of Orthopaedic Surgery Cairo UniversitytarikeopsNo ratings yet
- Bone Grafts and Their SubstitutesDocument4 pagesBone Grafts and Their SubstitutesIndriastuti SoetomoNo ratings yet
- Lecture 31 Osteoporosis Pathophys FlattenedDocument3 pagesLecture 31 Osteoporosis Pathophys FlattenedAhmed Mashaly100% (1)
- Death&Birth 00Document23 pagesDeath&Birth 00kyz79No ratings yet
- Hyperphosphatemia CKDDocument9 pagesHyperphosphatemia CKDNico MirassoNo ratings yet
- CCCCCCCDocument4 pagesCCCCCCCGali Alfaro ZagalNo ratings yet
- Os 1 251Document7 pagesOs 1 251mukhlis akmalNo ratings yet
- Osteoporosis: Current Concepts: Ibrahim Akkawi Hassan ZmerlyDocument6 pagesOsteoporosis: Current Concepts: Ibrahim Akkawi Hassan ZmerlyDimas M IlhamNo ratings yet
- Module 4 HomeworkDocument4 pagesModule 4 HomeworkCj LinceNo ratings yet
- Reviseddd (Mia)Document16 pagesReviseddd (Mia)kuro hanabusaNo ratings yet
- MSE Research 1Document11 pagesMSE Research 1kuro hanabusaNo ratings yet
- Nursing - Assessment - (Mse) (Josol)Document5 pagesNursing - Assessment - (Mse) (Josol)kuro hanabusaNo ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Inference Goal Nursing Intervention Rationale EvaluationDocument1 pageNursing Care Plan Cues Nursing Diagnosis Inference Goal Nursing Intervention Rationale Evaluationkuro hanabusaNo ratings yet
- Nursing Care Plan 1Document5 pagesNursing Care Plan 1kuro hanabusaNo ratings yet
- Date Identified: July 13, 2021 Date Evaluated: July 20, 2021 TetengDocument5 pagesDate Identified: July 13, 2021 Date Evaluated: July 20, 2021 Tetengkuro hanabusaNo ratings yet
- Anxiety NCPDocument2 pagesAnxiety NCPkuro hanabusaNo ratings yet
- Drug Study (Acamprosate (Campral) and Bupropion)Document5 pagesDrug Study (Acamprosate (Campral) and Bupropion)kuro hanabusaNo ratings yet
- Quiz (Perfect)Document3 pagesQuiz (Perfect)kuro hanabusaNo ratings yet
- Drug Study (Loxapine, Haloperidol)Document5 pagesDrug Study (Loxapine, Haloperidol)kuro hanabusa100% (2)
- Program Design (Dance Therapy)Document3 pagesProgram Design (Dance Therapy)kuro hanabusaNo ratings yet
- Pre-Test (B)Document7 pagesPre-Test (B)kuro hanabusaNo ratings yet
- Psychoanalysis and Psychodynamic TherapiesDocument51 pagesPsychoanalysis and Psychodynamic Therapieskuro hanabusaNo ratings yet
- Journal Reflection On Nursing Care PlanDocument9 pagesJournal Reflection On Nursing Care Plankuro hanabusaNo ratings yet
- Journal Reflection On Mental Status Examination 1Document9 pagesJournal Reflection On Mental Status Examination 1kuro hanabusaNo ratings yet
- Journal Reflection On Therapeutic ModalitiesDocument23 pagesJournal Reflection On Therapeutic Modalitieskuro hanabusaNo ratings yet
- Psychoanalysis and Psychodynamic TherapiesDocument51 pagesPsychoanalysis and Psychodynamic Therapieskuro hanabusaNo ratings yet
- Mental Status Examination: Concerns and AddictionDocument2 pagesMental Status Examination: Concerns and Addictionkuro hanabusaNo ratings yet
- DocxDocument53 pagesDocxkuro hanabusaNo ratings yet
- Francisco Arcellana: 4 Life Lessons That Can Be Derived From The StoryDocument1 pageFrancisco Arcellana: 4 Life Lessons That Can Be Derived From The Storykuro hanabusaNo ratings yet
- Philippine Literature During American RegimeDocument13 pagesPhilippine Literature During American Regimekuro hanabusaNo ratings yet
- CNT Manual 7th EditionDocument85 pagesCNT Manual 7th EditionStoopidHead100% (1)
- Note TakingDocument57 pagesNote TakingLee이서영No ratings yet
- Drug Presentation On Anti-Hypertensive: All India Institute of Medical and Science New Delhi 2021-2022Document12 pagesDrug Presentation On Anti-Hypertensive: All India Institute of Medical and Science New Delhi 2021-2022Priya SinghNo ratings yet
- CLPNM PD Nursing Foot CareDocument9 pagesCLPNM PD Nursing Foot CareMourad LAKHOUADRANo ratings yet
- Pre AnestesiDocument64 pagesPre AnestesiKevin YonathanNo ratings yet
- Dry Eye Syndrome - Basic and Clinical PerspectivesDocument129 pagesDry Eye Syndrome - Basic and Clinical PerspectivesPutri kartiniNo ratings yet
- Cardiovascular Hypertensive Crisis Recent EvidenceDocument6 pagesCardiovascular Hypertensive Crisis Recent Evidenceagustinaw1981No ratings yet
- Incident Classification: Class I Incidents: DateDocument3 pagesIncident Classification: Class I Incidents: DateJuan Ernesto Benavides VNo ratings yet
- Rheumatoid Arthritis PathophysiologyDocument3 pagesRheumatoid Arthritis PathophysiologyArunNo ratings yet
- CC1 Lab Manual FinalDocument14 pagesCC1 Lab Manual FinalMelody PardilloNo ratings yet
- Review Article: Biliary Atresia: 50 Years After The First KasaiDocument16 pagesReview Article: Biliary Atresia: 50 Years After The First Kasaibela RachmanNo ratings yet
- Genacol Instant: The Most Complete Reference Booklet About CollagenDocument28 pagesGenacol Instant: The Most Complete Reference Booklet About CollagendiosesatomicsNo ratings yet
- Riqas Ri RQ9142 11aDocument6 pagesRiqas Ri RQ9142 11aGrescia Ramos VegaNo ratings yet
- BerirabDocument6 pagesBerirabfateme.tf.1999No ratings yet
- Chd. AmiDocument4 pagesChd. AmiDead shotNo ratings yet
- Therapeutic Communication Between Nurse - PatientDocument10 pagesTherapeutic Communication Between Nurse - PatientLucy P PutriNo ratings yet
- Diagnostic Test For Endocrine DisordersDocument15 pagesDiagnostic Test For Endocrine DisordersRichard Deo R. Alave100% (1)
- Neonatal Sepsis - A Review: January 2012Document9 pagesNeonatal Sepsis - A Review: January 2012Tiwi QiraNo ratings yet
- THE Beginner'S Guide To Earthing: Brought To You byDocument23 pagesTHE Beginner'S Guide To Earthing: Brought To You byPopescu AndreeaNo ratings yet
- The Fastest Way To Sleep?Document7 pagesThe Fastest Way To Sleep?NNorameenNo ratings yet
- WHO Global Pandemic Phases and The Stages For Federal Government ResponseDocument4 pagesWHO Global Pandemic Phases and The Stages For Federal Government ResponseMara Luisa PanopioNo ratings yet
- Proprioception, Vestibular & CoordinationDocument28 pagesProprioception, Vestibular & Coordinationzm2h8hpsq8No ratings yet
- Mesotherapy in The Treatment of MusculoskeletalDocument11 pagesMesotherapy in The Treatment of MusculoskeletalArmin ArceoNo ratings yet
- Pe AnswerssDocument9 pagesPe AnswerssAngela Ruth MoranNo ratings yet
- Hesi Comprehensive Review For The Nclex RN Examination 6E Oct 3 2019 - 0323582451 - Elsevier Hesi Full ChapterDocument67 pagesHesi Comprehensive Review For The Nclex RN Examination 6E Oct 3 2019 - 0323582451 - Elsevier Hesi Full Chaptertracy.zimmer564100% (17)
- Concept PaperDocument3 pagesConcept PaperNndaydna0% (1)