Download as pdf or txt
You might also like
- Pharmacology Usmle Step 1Document5 pagesPharmacology Usmle Step 1raj_1041100% (16)
- Meeks Lifespan Development Exam 1 ReviewDocument8 pagesMeeks Lifespan Development Exam 1 Reviewdick mgeeNo ratings yet
- Thyroid Disorders in PregnancyDocument46 pagesThyroid Disorders in PregnancyMara Medina - BorleoNo ratings yet
- Module 11 Balasbas Cyrel Andrie V.Document13 pagesModule 11 Balasbas Cyrel Andrie V.Mary Angeline De LeonNo ratings yet
- Dyscephalia Mandibulo-Oculo-FacialisDocument5 pagesDyscephalia Mandibulo-Oculo-FacialisReyes Ivan García CuevasNo ratings yet
- Fertility and The FaceDocument6 pagesFertility and The FaceMatteo GobboNo ratings yet
- Jurnal InfanticideDocument4 pagesJurnal InfanticideElma NurNo ratings yet
- Jurnal Infanticide PDFDocument4 pagesJurnal Infanticide PDFAbdulAzizNo ratings yet
- Educ 101.module 11Document8 pagesEduc 101.module 11Avigale VelascoNo ratings yet
- Shanske 1997Document4 pagesShanske 1997dad dzd adaNo ratings yet
- Name: Meldred J. Lelis Course/Year: BEED-1: Activity 1: Let's Watch!Document9 pagesName: Meldred J. Lelis Course/Year: BEED-1: Activity 1: Let's Watch!Meldred J. LelisNo ratings yet
- Scientific Evidence For ReincarnationDocument2 pagesScientific Evidence For ReincarnationS.r. SarathNo ratings yet
- Lifebeforebirth: Consider This Observation by A New York DoctorDocument2 pagesLifebeforebirth: Consider This Observation by A New York DoctorAsida Maronsing DelionNo ratings yet
- Pedia Block 3 Part 2 RecallsDocument77 pagesPedia Block 3 Part 2 RecallsDale OcampoNo ratings yet
- Progressive Era EssaysDocument5 pagesProgressive Era Essaysafibafftauhxeh100% (2)
- MCN Case Pre 1 1Document64 pagesMCN Case Pre 1 1Rolland Ray MendozaNo ratings yet
- The First Nine MonthsDocument9 pagesThe First Nine MonthsSayeed KhanNo ratings yet
- Educ 101 ReviewerDocument27 pagesEduc 101 ReviewerRolando AmadNo ratings yet
- The Prenatal Development.. PPT PresentationDocument38 pagesThe Prenatal Development.. PPT PresentationalexandravisteriaNo ratings yet
- Moral Issues of Birth DeformitiesDocument3 pagesMoral Issues of Birth DeformitiesPham PhamIoNo ratings yet
- Abortion - Does The Bible Speak To ItDocument26 pagesAbortion - Does The Bible Speak To ItjhonNo ratings yet
- Catholic Church TeachingDocument4 pagesCatholic Church Teachingasixtioso7850No ratings yet
- Ausmolo N1A Activity5Document4 pagesAusmolo N1A Activity5MV ANo ratings yet
- Fausto - SterlingDocument35 pagesFausto - SterlingAlex BlencoweNo ratings yet
- Variacion en PuberDocument13 pagesVariacion en PuberCesar ChinoNo ratings yet
- Dwnload Full Childhood and Adolescence Voyages in Development 6th Edition Rathus Solutions Manual PDFDocument36 pagesDwnload Full Childhood and Adolescence Voyages in Development 6th Edition Rathus Solutions Manual PDFdoughnut.synocilj084s100% (13)
- Childhood and Adolescence Voyages in Development 6th Edition Rathus Solutions ManualDocument36 pagesChildhood and Adolescence Voyages in Development 6th Edition Rathus Solutions Manualaudiblycaribbeeuwiq100% (23)
- The Living Embryo and Making of Whole Mounts 72Document7 pagesThe Living Embryo and Making of Whole Mounts 72joemark_narsico5796100% (1)
- Eye 198865Document15 pagesEye 198865Apps OmNo ratings yet
- Ethics in Research Involving Human Subjects at The Beginning of LifeDocument15 pagesEthics in Research Involving Human Subjects at The Beginning of LifeDr. Liza ManaloNo ratings yet
- Neurological Reorganization For Brain Injury by Sargent L. Goodchild, Jr.Document6 pagesNeurological Reorganization For Brain Injury by Sargent L. Goodchild, Jr.autismoneNo ratings yet
- Layered BookDocument14 pagesLayered Bookapi-318163621No ratings yet
- Cytogenetics Lecture #1Document4 pagesCytogenetics Lecture #1Bryle Owen Rañoa LabangNo ratings yet
- CH 10 Class 8th Answer SheetDocument3 pagesCH 10 Class 8th Answer SheetSvanik DuttaNo ratings yet
- PSY 101 Week 5 Final PaperDocument7 pagesPSY 101 Week 5 Final PaperElisa FlemingNo ratings yet
- General PsychologyDocument80 pagesGeneral PsychologyPedro Caingal PerezNo ratings yet
- Pneumonia Careplan MedDocument17 pagesPneumonia Careplan MedGayatri MudliyarNo ratings yet
- Summary of Grantly Dick-Read & Ina May Gaskin's Childbirth Without FearFrom EverandSummary of Grantly Dick-Read & Ina May Gaskin's Childbirth Without FearRating: 3.5 out of 5 stars3.5/5 (2)
- Time - How First Nine MonthsDocument6 pagesTime - How First Nine MonthsSuperfixenNo ratings yet
- 6.1 Assessment of Fetal Growth & DevekiomentDocument9 pages6.1 Assessment of Fetal Growth & DevekiomentRafael OliveiraNo ratings yet
- Dwnload Full Comprehensive Stress Management 13th Edition Greenberg Test Bank PDFDocument35 pagesDwnload Full Comprehensive Stress Management 13th Edition Greenberg Test Bank PDFgeck.nereis3vwg100% (20)
- MCN II AntepartumDocument28 pagesMCN II AntepartumJharaNo ratings yet
- Neonatal AscariasisDocument3 pagesNeonatal AscariasisAnonymous Tr4aGt7No ratings yet
- Analysis of Research by Professor Ian StevensonDocument7 pagesAnalysis of Research by Professor Ian Stevensonprabhatranjan23No ratings yet
- Aborto en Los Niños ADocument2 pagesAborto en Los Niños AEs PaNo ratings yet
- Archie Kalokerinos - Shaken Baby Syndrome - An Abusive DiagnosisDocument70 pagesArchie Kalokerinos - Shaken Baby Syndrome - An Abusive DiagnosisLuc LiebecqNo ratings yet
- Secrets of Your Cells: Discovering Your Body's Inner IntelligenceFrom EverandSecrets of Your Cells: Discovering Your Body's Inner IntelligenceRating: 1 out of 5 stars1/5 (1)
- Conception To Adolescent 107 NormalDocument12 pagesConception To Adolescent 107 NormalMark Jhon PausanosNo ratings yet
- Stem Cells: Controversy at the Frontiers of ScienceFrom EverandStem Cells: Controversy at the Frontiers of ScienceRating: 5 out of 5 stars5/5 (2)
- DVD Outline PDF ExampleDocument4 pagesDVD Outline PDF Exampletrash1000No ratings yet
- Chapter 5 Developing Through The Life Span - 42 QuestionsDocument13 pagesChapter 5 Developing Through The Life Span - 42 QuestionsLee ThompsonNo ratings yet
- Developing Through The Life SpanDocument11 pagesDeveloping Through The Life SpanMa. Nenita L. MagallanesNo ratings yet
- Developing Through The Life Span: Learning ObjectivesDocument18 pagesDeveloping Through The Life Span: Learning ObjectivesHayaton IRNo ratings yet
- Spiritual Health & Wellness: Let's Talk About Peace & Power: Spiritual Health & Wellness, #2From EverandSpiritual Health & Wellness: Let's Talk About Peace & Power: Spiritual Health & Wellness, #2No ratings yet
- Ped01-Module 4Document2 pagesPed01-Module 4Charlene Jadie EmbradoNo ratings yet
- Preboards2 DevpsyDocument10 pagesPreboards2 Devpsyarniedado07No ratings yet
- CamScanner 10-29-2020 13.11.47Document69 pagesCamScanner 10-29-2020 13.11.47Yuki ChanNo ratings yet
- Psychiatric Advanced Practice Nursing 1st Edition Perese Test BankDocument35 pagesPsychiatric Advanced Practice Nursing 1st Edition Perese Test Bankphysetergrannam.devtjz100% (30)
- And Care: Unit Prenatal DevelopmentDocument9 pagesAnd Care: Unit Prenatal DevelopmentPratibha ChNo ratings yet
- Dream Life - Allan HobsonDocument307 pagesDream Life - Allan HobsonJose MuñozNo ratings yet
- Case Report: Persistent Open Anterior Fontanelle in A Healthy 32-Month-Old BoyDocument2 pagesCase Report: Persistent Open Anterior Fontanelle in A Healthy 32-Month-Old BoydickyaririsandyNo ratings yet
- Questions For NursingDocument26 pagesQuestions For Nursingjoan olanteNo ratings yet
- Nursing BulletsDocument65 pagesNursing Bulletsjoan olanteNo ratings yet
- Funda Board ExamDocument107 pagesFunda Board Examjoan olanteNo ratings yet
- Renal System: Diagnostic ExaminationsDocument8 pagesRenal System: Diagnostic Examinationsjoan olanteNo ratings yet
- About 70% of All Sensory Information Reaches The Brain Through The EyesDocument127 pagesAbout 70% of All Sensory Information Reaches The Brain Through The Eyesjoan olanteNo ratings yet
- Psychosexual Disorders: Pedophilia Gender Identity DisorderDocument5 pagesPsychosexual Disorders: Pedophilia Gender Identity Disorderjoan olanteNo ratings yet
- Cbahi Esr Standards PDFDocument10 pagesCbahi Esr Standards PDFjoan olanteNo ratings yet
- Documentation in Nursing: Mahmood AhmedDocument41 pagesDocumentation in Nursing: Mahmood Ahmedjoan olanteNo ratings yet
- Nursing Service MANUALDocument37 pagesNursing Service MANUALjoan olanteNo ratings yet
- Intra-Uterine Device (IUD) Insertion Equipment ListDocument2 pagesIntra-Uterine Device (IUD) Insertion Equipment Listjoan olanteNo ratings yet
- 3D Bioprinting of Endocrine GlandsDocument12 pages3D Bioprinting of Endocrine GlandsDivya DarshiniNo ratings yet
- Propylthiouracil 2Document14 pagesPropylthiouracil 2Magdy Ali ELsherbenyNo ratings yet
- Graves DiseaseDocument6 pagesGraves Diseaseabida.syeda.718No ratings yet
- Kab ReetDocument254 pagesKab ReetAsia AlhkeemNo ratings yet
- Diagnosis and Management of Thyroid Disease During Pregnancy and Postpartum - ATADocument61 pagesDiagnosis and Management of Thyroid Disease During Pregnancy and Postpartum - ATAtabhsinghiNo ratings yet
- TFG Alba Redon LagoDocument42 pagesTFG Alba Redon LagoIswarya RajkumarNo ratings yet
- HeadDocument9 pagesHeadAnonymous BzS0RF1qyNo ratings yet
- Congenital HypothyroidismDocument18 pagesCongenital Hypothyroidismcalamyl295No ratings yet
- # Pembagian Kelas Alkes Per KategoriDocument41 pages# Pembagian Kelas Alkes Per KategoriR.A.R TVNo ratings yet
- Endocrine MedicationsDocument47 pagesEndocrine MedicationsAamir AzizNo ratings yet
- MR NITIN PDFDocument2 pagesMR NITIN PDFVenkat Nitin GuttaNo ratings yet
- Theories Factors Affecting Growth and DevelopmentDocument73 pagesTheories Factors Affecting Growth and DevelopmentYasmeen Jaffer100% (1)
- Nilsson 2017Document18 pagesNilsson 2017نذير الشرعبيNo ratings yet
- Class 10 Chapter 12 The Endocrine SystemDocument14 pagesClass 10 Chapter 12 The Endocrine SystemDXN LUDHIANANo ratings yet
- L34 - MR - Nilesh Yadav - Kota CC 6 RAY-99/100, Bajrang Nagar Main Road, Near Bright Land School, Kota-324001Document11 pagesL34 - MR - Nilesh Yadav - Kota CC 6 RAY-99/100, Bajrang Nagar Main Road, Near Bright Land School, Kota-324001Shivam MittalNo ratings yet
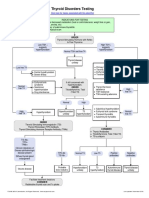
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmRezi HelperNo ratings yet
- Chapter 12 12.6 and 12.7Document16 pagesChapter 12 12.6 and 12.7Omkara HiteshNo ratings yet
- PopcornDocument41 pagesPopcorntrixia therese00No ratings yet
- Lecture10 CommunicationIII 1Document30 pagesLecture10 CommunicationIII 1Liana Rose MeregildoNo ratings yet
- ThyroidectomyDocument51 pagesThyroidectomyPopey Moore100% (1)
- Biochemistry of Hormones - Lecture NotesDocument9 pagesBiochemistry of Hormones - Lecture NotesAyukafangha EtandoNo ratings yet
- Pregnancy Thyroid DiseaseDocument8 pagesPregnancy Thyroid DiseaseYhang Lidi TamaNo ratings yet
- Subacute Thyroiditis PDFDocument102 pagesSubacute Thyroiditis PDFIoana BodescuNo ratings yet
- Interpretation of Lab Test ProfilesDocument18 pagesInterpretation of Lab Test Profilesrox_anne100% (1)
- Biochem Experiment 5Document6 pagesBiochem Experiment 5Julius Memeg PanayoNo ratings yet
- Department of Hormones: TSH 1.1 mIU/LDocument1 pageDepartment of Hormones: TSH 1.1 mIU/LSankar KsNo ratings yet
- 6 Day Advanced Water FastingDocument78 pages6 Day Advanced Water Fastingmariyastoj100% (1)