Download as docx, pdf, or txt
You might also like
- Unit Iii Meaning and Significance of Statistical Process Control (SPC)Document7 pagesUnit Iii Meaning and Significance of Statistical Process Control (SPC)prasannabalajiNo ratings yet
- Huawei ICT Competition 2019-2020 Preliminary Examination Outline - PAkDocument5 pagesHuawei ICT Competition 2019-2020 Preliminary Examination Outline - PAkHamad KhanNo ratings yet
- 3.3-jcp00-cuginiEFFECT OF SRPDocument7 pages3.3-jcp00-cuginiEFFECT OF SRPNeli IvanovaNo ratings yet
- 20-Article Text-36-1-10-20180320 PDFDocument11 pages20-Article Text-36-1-10-20180320 PDFAnonymous WlnsCwAjFNo ratings yet
- A Comparative Study of Dermatoglyphics in Individuals With Normal Occlusions and MalocclusionsDocument7 pagesA Comparative Study of Dermatoglyphics in Individuals With Normal Occlusions and Malocclusionschandralekha jayamaniNo ratings yet
- Chapter IiiDocument10 pagesChapter IiiSheryl JesslynNo ratings yet
- Dermatoglyphics and Malocclusion - Are They Related ?: Manuscript InfoDocument7 pagesDermatoglyphics and Malocclusion - Are They Related ?: Manuscript InfoHardiklalakiyaNo ratings yet
- HC e Cera (Comparacao)Document6 pagesHC e Cera (Comparacao)JARDEL DOS SANTOS SILVANo ratings yet
- D I D C A I V S: Ermatoglyphics Nterpretation of Ental Aries: N N TudyDocument3 pagesD I D C A I V S: Ermatoglyphics Nterpretation of Ental Aries: N N TudyShahanaaz ShaikNo ratings yet
- Fluoride VarnishDocument6 pagesFluoride VarnishNiki MeNo ratings yet
- Standardizing Interarch Tooth-Size Harmony in A SyrianDocument4 pagesStandardizing Interarch Tooth-Size Harmony in A SyrianHafaifa TaiebNo ratings yet
- Prevalence of Dental Caries of One Grade School Children in KarachiDocument3 pagesPrevalence of Dental Caries of One Grade School Children in KarachikajdfaskNo ratings yet
- Malocclusion and Orthodontic Treatment Need Among 12-15-Year-Old Children in NairobiDocument6 pagesMalocclusion and Orthodontic Treatment Need Among 12-15-Year-Old Children in NairobiWainaianaNo ratings yet
- Koroluk 16 04Document6 pagesKoroluk 16 04Anitha AugustineNo ratings yet
- Oral CandidiasisDocument4 pagesOral CandidiasisAnonymous 0ttLN5No ratings yet
- Tooth Size Discrepancies in Libyan Class I and II Orthodontic Patients Cross Sectional Retrospective StudyDocument5 pagesTooth Size Discrepancies in Libyan Class I and II Orthodontic Patients Cross Sectional Retrospective StudyAdvanced Research PublicationsNo ratings yet
- Two-Year Split-Mouth Randomized Controlled Clinical Trial On The Progression of Proximal Carious Lesions On Primary Molars After Resin InfiltrationDocument6 pagesTwo-Year Split-Mouth Randomized Controlled Clinical Trial On The Progression of Proximal Carious Lesions On Primary Molars After Resin InfiltrationsofiaNo ratings yet
- Ijcmsr 3 1 58 v1 2Document3 pagesIjcmsr 3 1 58 v1 2vinaNo ratings yet
- DTM - 2126 Manuscript 12213 1 10 20191114Document7 pagesDTM - 2126 Manuscript 12213 1 10 20191114Cinthia PatronNo ratings yet
- Black Tooth Stain and Dental Caries Among Udaipur School ChildrenDocument5 pagesBlack Tooth Stain and Dental Caries Among Udaipur School ChildrenMardiyah PratiwiNo ratings yet
- Libro de ActasDocument3 pagesLibro de ActasWendy BarrazuetaNo ratings yet
- A Cross-Sectional Study of Factors Associated With Prevalence and Progress of Dentin HypersensitivityDocument3 pagesA Cross-Sectional Study of Factors Associated With Prevalence and Progress of Dentin HypersensitivityAlya Hana NatasyaNo ratings yet
- Irigasi 3.8% SDFDocument5 pagesIrigasi 3.8% SDFatmokotomoNo ratings yet
- Proiect Et IoanaDocument6 pagesProiect Et IoanaldgiNo ratings yet
- Discussion: Cross-Sectional and DescriptiveDocument11 pagesDiscussion: Cross-Sectional and DescriptiveKavin Maalan SadasseevanNo ratings yet
- Krishan KumarDocument7 pagesKrishan KumarVi LinhNo ratings yet
- Oral Health Status of Disabled ChildrenDocument4 pagesOral Health Status of Disabled ChildrenVõ XinhNo ratings yet
- Examination of Young Children With Lea SymbolsDocument6 pagesExamination of Young Children With Lea SymbolsArturo GuilliemNo ratings yet
- Prevalence of Pacifier-Sucking Habits and Successful Methods To Eliminate Them-A Preliminary StudyDocument4 pagesPrevalence of Pacifier-Sucking Habits and Successful Methods To Eliminate Them-A Preliminary StudysrinandanNo ratings yet
- Fcimb 07 00392Document11 pagesFcimb 07 00392Sares DaselvaNo ratings yet
- Archives of Oral BiologyDocument11 pagesArchives of Oral BiologyJohamurillocNo ratings yet
- Jurnal English 5Document7 pagesJurnal English 5Yulia Dwi KartikaNo ratings yet
- 1.1 Need For The StudyDocument35 pages1.1 Need For The StudyNAGESH RAJNo ratings yet
- Safety and Efficacy of Dente91 MOM Toothpaste and Dente91 MOM Mouthwash in Pregnant FemalesDocument4 pagesSafety and Efficacy of Dente91 MOM Toothpaste and Dente91 MOM Mouthwash in Pregnant FemalesAnuj MundhraNo ratings yet
- Hasil Dan Pembahasan - Id.enDocument6 pagesHasil Dan Pembahasan - Id.enKirana Aulia PutriNo ratings yet
- Application of Community Periodontal Index in NigeriaDocument4 pagesApplication of Community Periodontal Index in NigeriaAhmad Abd El-GhaniNo ratings yet
- Dental Plaque Score Index Differences in Children With Mental Retardation: With and Without SupervisionDocument10 pagesDental Plaque Score Index Differences in Children With Mental Retardation: With and Without SupervisionWindy Puspa KusumahNo ratings yet
- Periodontal Status of Habitual Adult Users of Miswak Sticks or Toothbrushes Among A Population in Al-Madinah Al-MunawaraDocument5 pagesPeriodontal Status of Habitual Adult Users of Miswak Sticks or Toothbrushes Among A Population in Al-Madinah Al-MunawaraJanuhu ZakaryNo ratings yet
- Dental Trauma in Contact SportsDocument6 pagesDental Trauma in Contact Sportsjessica soaresNo ratings yet
- Red Green Color Vision Deficiency and Lack of Awareness in Rural School IndiaDocument3 pagesRed Green Color Vision Deficiency and Lack of Awareness in Rural School India0039 NURUL HANI IZZUANI BINTI AFRIZANNo ratings yet
- J Ajodo 2010 03 024Document7 pagesJ Ajodo 2010 03 024Amal KebirNo ratings yet
- Tratamiento para La AMEDocument7 pagesTratamiento para La AMEJhon SuquinaguaNo ratings yet
- DE5 OA Rohin-2Document4 pagesDE5 OA Rohin-2The Lost GuyNo ratings yet
- 2-4pm Extraction Class IIDocument10 pages2-4pm Extraction Class IIKristty MagallanesNo ratings yet
- 8.biostatistics IIIDocument39 pages8.biostatistics IIIMahnoor khanNo ratings yet
- Quantifying Effects in Two-Sample Environmental Experiments Using Bootstrap Confidence IntervalsDocument13 pagesQuantifying Effects in Two-Sample Environmental Experiments Using Bootstrap Confidence Intervalsgautamsethi8561No ratings yet
- Test Group: 7: ResultsDocument25 pagesTest Group: 7: ResultsGayathri LalNo ratings yet
- Plaque Removal Efficacy of Triple-Headed Toothbrush in 4-6-Year-Old Children A Randomized Crossover Study - PMCDocument1 pagePlaque Removal Efficacy of Triple-Headed Toothbrush in 4-6-Year-Old Children A Randomized Crossover Study - PMCnada.elsaeidNo ratings yet
- Ipi350248 PDFDocument12 pagesIpi350248 PDFPutu karang atmadiNo ratings yet
- Ipi350248 PDFDocument12 pagesIpi350248 PDFPutu karang atmadiNo ratings yet
- Ipi350248 PDFDocument12 pagesIpi350248 PDFPutu karang atmadiNo ratings yet
- Ipi350248 PDFDocument12 pagesIpi350248 PDFPutu karang atmadiNo ratings yet
- Ipi350248 PDFDocument12 pagesIpi350248 PDFPutu karang atmadiNo ratings yet
- Ipi350248 PDFDocument12 pagesIpi350248 PDFPutu karang atmadiNo ratings yet
- Ipi350248 PDFDocument12 pagesIpi350248 PDFPutu karang atmadiNo ratings yet
- Ipi350248 PDFDocument12 pagesIpi350248 PDFPutu karang atmadiNo ratings yet
- File Kapita DyscalculiaDocument22 pagesFile Kapita DyscalculiaDiana RosdianaNo ratings yet
- CUHK STAT3004 Assignment 2Document3 pagesCUHK STAT3004 Assignment 2屁屁豬No ratings yet
- IJO Volume 5 Issue 1 Pages 62-69Document8 pagesIJO Volume 5 Issue 1 Pages 62-69Iddi IddiNo ratings yet
- Roxana 2Document4 pagesRoxana 2Kirvase DanNo ratings yet
- Color and Appearance in DentistryFrom EverandColor and Appearance in DentistryAlvaro Della BonaNo ratings yet
- Interventions for Autism: Evidence for Educational and Clinical PracticeFrom EverandInterventions for Autism: Evidence for Educational and Clinical PracticeNo ratings yet
- 4-Optical Properties of Materials-Dielectrics and MetalsDocument36 pages4-Optical Properties of Materials-Dielectrics and MetalsvenkateshsanthiNo ratings yet
- (Rise Up) - Straight Lines - Sep 1Document238 pages(Rise Up) - Straight Lines - Sep 1prakhar100% (1)
- Chapter - 1-QMDocument56 pagesChapter - 1-QMtebelayhabitamu12No ratings yet
- Grading Rubric TitrationDocument2 pagesGrading Rubric Titrationapi-205419744No ratings yet
- Photo Mechanic 4.5.3 ManualDocument132 pagesPhoto Mechanic 4.5.3 ManualRodrigo Franco Carlovich MoreiraNo ratings yet
- Basic Principles For Sizing Grease InterceptorsDocument5 pagesBasic Principles For Sizing Grease InterceptorsSharon LambertNo ratings yet
- Bharat Heavy Electricals Limited: Tvenkat@bheltry - Co.inDocument5 pagesBharat Heavy Electricals Limited: Tvenkat@bheltry - Co.inRukma Goud Shakkari100% (1)
- Manual EP200 enDocument42 pagesManual EP200 enJose AguirreNo ratings yet
- Limit States Design of Crane Runway GirdersDocument7 pagesLimit States Design of Crane Runway GirdersRatna YanuarNo ratings yet
- BOSCH Bio DecontaminationH2O2Document25 pagesBOSCH Bio DecontaminationH2O2Davide GrioniNo ratings yet
- LPM NutshellDocument8 pagesLPM NutshellRaja SekarNo ratings yet
- Using eQube-BITcRA To Make Sense of PLM DataDocument15 pagesUsing eQube-BITcRA To Make Sense of PLM Datayacey52153No ratings yet
- ATP Guidelines For Sector AdditionDocument31 pagesATP Guidelines For Sector AdditionGaurav SinghNo ratings yet
- Essential Spreadsheets Book-2Document40 pagesEssential Spreadsheets Book-2señalesuisNo ratings yet
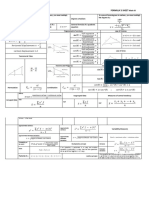
- FORMULA S SHEET Math IIIDocument2 pagesFORMULA S SHEET Math IIIDani RuizNo ratings yet
- MGT LearningDocument18 pagesMGT Learningmoraiskp321No ratings yet
- Emergency Braking SystemDocument4 pagesEmergency Braking Systemieee4mybusinessonlyNo ratings yet
- Assignment 5 A - Quadratic EquationsDocument4 pagesAssignment 5 A - Quadratic EquationsSakiNo ratings yet
- MPPT Tecnicas.Document21 pagesMPPT Tecnicas.Daniel Alonso Juárez MartínezNo ratings yet
- Buy 13-Inch MacBook Pro - Apple (IN)Document1 pageBuy 13-Inch MacBook Pro - Apple (IN)dummy page7007No ratings yet
- PG2794 00 - en GBDocument4 pagesPG2794 00 - en GBphalkejituNo ratings yet
- OP Flash DistillationDocument11 pagesOP Flash DistillationDylan Navarro LNo ratings yet
- OTFS: A New Modulation Scheme For High Mobility Use Cases: M. K. Ramachandran, G. D. Surabhi and A. ChockalingamDocument22 pagesOTFS: A New Modulation Scheme For High Mobility Use Cases: M. K. Ramachandran, G. D. Surabhi and A. ChockalingamUpasana KouravNo ratings yet
- SPSS Wulan RahmaniaDocument12 pagesSPSS Wulan RahmaniaUlanNo ratings yet
- Hubungan Mutu Pelayanan Kesehatan Dengan Kepuasan Pasien Rawat Ninap Di Rumah Sakit Umum Daya Makssar TAHUN 2012Document14 pagesHubungan Mutu Pelayanan Kesehatan Dengan Kepuasan Pasien Rawat Ninap Di Rumah Sakit Umum Daya Makssar TAHUN 2012uli shalatiyaNo ratings yet
- Customer Inquiry Sheet BlankDocument3 pagesCustomer Inquiry Sheet BlankAbunawas_MJNo ratings yet
- Shan Zhong, Student Member, IEEE, and Ali Abur, Senior Member, IEEEDocument5 pagesShan Zhong, Student Member, IEEE, and Ali Abur, Senior Member, IEEEAhmadinijadNo ratings yet
- 2) DMD 3123 - Co Automatic Vehicle TransmissionDocument9 pages2) DMD 3123 - Co Automatic Vehicle TransmissionShinobi 05No ratings yet