Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- To Make Flip Flop Led Flasher Circuit Using Transistor Bc547Document17 pagesTo Make Flip Flop Led Flasher Circuit Using Transistor Bc547ananyabedekar83No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Chapter 6 StressDocument9 pagesChapter 6 StressSiti Sarah Zalikha Binti Umar BakiNo ratings yet
- Arthur Clifton GuytonDocument2 pagesArthur Clifton GuytonArlyn SanchezNo ratings yet
- Artigo Trauma GenitalDocument7 pagesArtigo Trauma GenitalMarcella Bastos PersianoNo ratings yet
- Extramammary Paget's Disease: Surgical Treatment With Mohs Micrographic SurgeryDocument7 pagesExtramammary Paget's Disease: Surgical Treatment With Mohs Micrographic SurgeryMarcella Bastos PersianoNo ratings yet
- Gynecologic Oncology: Yipin Cai, Weiqi Sheng, Libing Xiang, Xiaohua Wu, Huijuan YangDocument5 pagesGynecologic Oncology: Yipin Cai, Weiqi Sheng, Libing Xiang, Xiaohua Wu, Huijuan YangMarcella Bastos PersianoNo ratings yet
- HER-2/neu Expression in Paget Disease of The Vulva and The Female BreastDocument5 pagesHER-2/neu Expression in Paget Disease of The Vulva and The Female BreastMarcella Bastos PersianoNo ratings yet
- Logging Best Practices Guide PDFDocument12 pagesLogging Best Practices Guide PDFbnanduriNo ratings yet
- The Last LessonDocument31 pagesThe Last LessonKanika100% (1)
- Usia Signifikan.Document14 pagesUsia Signifikan.neli fitriaNo ratings yet
- How To Register A Partnership in SECDocument4 pagesHow To Register A Partnership in SECMa Zola EstelaNo ratings yet
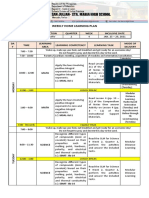
- Weekly Home Learning Plan: Grade Section Quarter Week Inclusive DateDocument3 pagesWeekly Home Learning Plan: Grade Section Quarter Week Inclusive DateMarvin Yebes ArceNo ratings yet
- GIS Based Analysis On Walkability of Commercial Streets at Continuing Growth Stages - EditedDocument11 pagesGIS Based Analysis On Walkability of Commercial Streets at Continuing Growth Stages - EditedemmanuelNo ratings yet
- Steve Nison - Candlestick Patterns - RezumatDocument22 pagesSteve Nison - Candlestick Patterns - RezumatSIightlyNo ratings yet
- A Bravo Delta Lancaster Model Worth 329: 38 Paralle L Paralle LDocument116 pagesA Bravo Delta Lancaster Model Worth 329: 38 Paralle L Paralle LAnonymous 7Je2SSU100% (2)
- Intro To ForsciDocument16 pagesIntro To ForsciChloe MaciasNo ratings yet
- Indercos2021 Fulltext Congress BookDocument294 pagesIndercos2021 Fulltext Congress BookDr Sneha's Skin and Allergy Clinic IndiaNo ratings yet
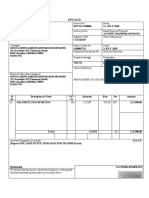
- Invoice: Qrt. No - : Cc-15, Civil Township Rourkela, Dist - (Sundargarh (Odisha) - 769012 GSTIN - 21ACWFS2234G1Z4Document2 pagesInvoice: Qrt. No - : Cc-15, Civil Township Rourkela, Dist - (Sundargarh (Odisha) - 769012 GSTIN - 21ACWFS2234G1Z4PUNYASHLOK PANDANo ratings yet
- Process of Concept Formation: ReferencesDocument1 pageProcess of Concept Formation: ReferencesRamani SwarnaNo ratings yet
- SPOUSES SALVADOR ABELLA v. SPOUSES ROMEO ABELLADocument2 pagesSPOUSES SALVADOR ABELLA v. SPOUSES ROMEO ABELLAAlia Arnz-Dragon100% (1)
- HABASIT 04 Guía Ingeniería HabasitLINKDocument100 pagesHABASIT 04 Guía Ingeniería HabasitLINKKyriakos MichalakiNo ratings yet
- Dedication Certificate John Clyde D. Cristobal: This Certifies ThatDocument1 pageDedication Certificate John Clyde D. Cristobal: This Certifies ThatAGSAOAY JASON F.No ratings yet
- Product Data Sheet Ingenuity Core LRDocument16 pagesProduct Data Sheet Ingenuity Core LRCeoĐứcTrườngNo ratings yet
- Influence of Cooling Rate On The Structure and Formation of Oxide Scale in LowDocument7 pagesInfluence of Cooling Rate On The Structure and Formation of Oxide Scale in LowVarun MangaloreNo ratings yet
- GAS ModelDocument3 pagesGAS ModelDibyendu ShilNo ratings yet
- Manual Mycom InglêsDocument158 pagesManual Mycom InglêsJorge Palinkas100% (1)
- Level B1 - Threshold: Speaking Mark Scheme - Assessor'sDocument2 pagesLevel B1 - Threshold: Speaking Mark Scheme - Assessor'sdeasaadiah100% (1)
- Study of Blood Groups and Rhesus Factor in Beta Thalassemia Patients Undergoing Blood TransfusionsDocument6 pagesStudy of Blood Groups and Rhesus Factor in Beta Thalassemia Patients Undergoing Blood TransfusionsOpenaccess Research paperNo ratings yet
- Past Simple Weekend.m4aDocument7 pagesPast Simple Weekend.m4aCarmen Victoria Niño RamosNo ratings yet
- Internet Banking Java Project ReportDocument68 pagesInternet Banking Java Project ReportKUMAR NILESH100% (1)
- Belgian Carrier PigeonDocument145 pagesBelgian Carrier PigeonstepathcNo ratings yet
- Sap Fico Blueprint-1Document32 pagesSap Fico Blueprint-1Deepak AggarwalNo ratings yet
- Dissertation Topics in HindiDocument7 pagesDissertation Topics in HindiPaperWritingCompanyBillings100% (1)
- Care of Terminally IllDocument34 pagesCare of Terminally Illbemina jaNo ratings yet