Download as docx, pdf, or txt
You might also like
- Anna - UPDATED 6 - 25 Printable - (18+) School of Rock Waiver & Code of ConductDocument16 pagesAnna - UPDATED 6 - 25 Printable - (18+) School of Rock Waiver & Code of ConductJake HartgeNo ratings yet
- Global Oncology Trends 2021-2025Document70 pagesGlobal Oncology Trends 2021-2025Deepak MakkarNo ratings yet
- NCM 113 Final Module 8 LectureDocument8 pagesNCM 113 Final Module 8 LectureAngel Khrisna BacasmotNo ratings yet
- Top 10 Public Health Challenges To Track in 2023Document8 pagesTop 10 Public Health Challenges To Track in 2023Anne LauretaNo ratings yet
- Health Care Delivery SystemDocument63 pagesHealth Care Delivery SystemclarenzsolivenNo ratings yet
- Public Health in Humanitarian Crisis: Submitted by Name: Tarun Kumar Kushwaha Registration Number: 12018958Document21 pagesPublic Health in Humanitarian Crisis: Submitted by Name: Tarun Kumar Kushwaha Registration Number: 12018958tarun kushwahaNo ratings yet
- Community Health Nursing 1 Public Health Nursing in The PhilippinesDocument16 pagesCommunity Health Nursing 1 Public Health Nursing in The PhilippinesFlourence ZafranNo ratings yet
- Overview of Public Health Nursing in The Philippines: Learning ObjectivesDocument15 pagesOverview of Public Health Nursing in The Philippines: Learning ObjectivesRainy DaysNo ratings yet
- NCSC AssessmentDocument4 pagesNCSC AssessmentSushila KispottaNo ratings yet
- Un Platform FinalDocument18 pagesUn Platform FinalAginaya ReinNo ratings yet
- Primary Health CareDocument13 pagesPrimary Health CareJoia De Leon100% (3)
- 1020 3397 2020 2610 1148 1150 EngDocument3 pages1020 3397 2020 2610 1148 1150 EngRosales RonaldNo ratings yet
- CHN Modules No 3 4 PDFDocument262 pagesCHN Modules No 3 4 PDFMichael OblegoNo ratings yet
- A Position Pape-Wps OfficeDocument2 pagesA Position Pape-Wps OfficeReymart BuenNo ratings yet
- SSRN Id2625208 PDFDocument3 pagesSSRN Id2625208 PDFDiego Sebastián Rojas ToroNo ratings yet
- Primary Health CareDocument7 pagesPrimary Health CareCharlie Cotoner FalgueraNo ratings yet
- College of Nursing Module 5: Development Concepts, Principles and Strategies Overview of The ModuleDocument15 pagesCollege of Nursing Module 5: Development Concepts, Principles and Strategies Overview of The ModuleMarthy BollenaNo ratings yet
- Global Health Issues PPDocument91 pagesGlobal Health Issues PPRitaNo ratings yet
- Managing Health StrategiesDocument15 pagesManaging Health StrategiesMelaine TorreaNo ratings yet
- tmp243 TMPDocument3 pagestmp243 TMPFrontiersNo ratings yet
- Health CareDocument203 pagesHealth CareNiro ThakurNo ratings yet
- Public Health CourseworkDocument12 pagesPublic Health CourseworkAndrew AkamperezaNo ratings yet
- 0 CNU Nomination FormDocument3 pages0 CNU Nomination FormorlandawNo ratings yet
- Primary Health Care (PHC) in The PhilDocument23 pagesPrimary Health Care (PHC) in The PhilCLAUDETTE ANNE CORMARY100% (3)
- Civil Society's COVID-19 Calls To Action: PreambleDocument2 pagesCivil Society's COVID-19 Calls To Action: PreambleSyamsul PutraNo ratings yet
- 005handout 1.1.1 The Health ChallengeDocument4 pages005handout 1.1.1 The Health ChallengeDagnachew MulugetaNo ratings yet
- GROUP 2-Health-Care-Development-SystemDocument76 pagesGROUP 2-Health-Care-Development-SystemEzra MaeNo ratings yet
- Inbound 5566500222241268010Document38 pagesInbound 5566500222241268010Hazel Jane MillamaNo ratings yet
- Community Health Nursing LectureDocument35 pagesCommunity Health Nursing LectureMaxeneDhaleNo ratings yet
- Communicable DiseasesDocument10 pagesCommunicable Diseases2j9hddr7kpNo ratings yet
- Scope of Public HealthDocument33 pagesScope of Public Healthanjali100% (1)
- Global Health and Nursing Group 2Document16 pagesGlobal Health and Nursing Group 2Kathleen Camile CenaNo ratings yet
- Primary Health CareDocument57 pagesPrimary Health CareSwastika ShresthaNo ratings yet
- Primary Health CareDocument13 pagesPrimary Health Careرافت العواضيNo ratings yet
- Questions For Mr. Rajeev SadanandanDocument3 pagesQuestions For Mr. Rajeev SadanandanRajan MahalingamNo ratings yet
- CHN Lec P2Document40 pagesCHN Lec P2joy100% (1)
- The Twelfth Five-Year Plan For Health Sector DevelopmentDocument24 pagesThe Twelfth Five-Year Plan For Health Sector Developmentchain singh janviNo ratings yet
- Health and Economic Development: Linkage and ImpactDocument21 pagesHealth and Economic Development: Linkage and ImpactDora SimmonsNo ratings yet
- Batt Exam CHNDocument62 pagesBatt Exam CHNJoana Grace CortezNo ratings yet
- Primary Health Care (PHC) Is An Essential Health Care Made UniversallyDocument9 pagesPrimary Health Care (PHC) Is An Essential Health Care Made UniversallyAlimyon Abilar MontoloNo ratings yet
- Urban Health and Wellbeing Indian Case Studies 1st Ed 2020 978 981 13 6670 3 978 981 13 6671 0 - CompressDocument16 pagesUrban Health and Wellbeing Indian Case Studies 1st Ed 2020 978 981 13 6670 3 978 981 13 6671 0 - Compressisanvi0001No ratings yet
- PDP 2023 2028 - Chapter 2Document48 pagesPDP 2023 2028 - Chapter 2Krishna BalagaNo ratings yet
- Hsci 6330 Final ExamDocument7 pagesHsci 6330 Final Examapi-579553971No ratings yet
- Primary Health Care 1Document8 pagesPrimary Health Care 1JeanNo ratings yet
- Global Health and NursingDocument11 pagesGlobal Health and NursingDj Gwyn MandigmaNo ratings yet
- Consolidated FINALDocument25 pagesConsolidated FINALRainidah Mangotara Ismael-DericoNo ratings yet
- NCM 104 Lecture Chapter 2.1 Health-Care-Delivery-System 1Document25 pagesNCM 104 Lecture Chapter 2.1 Health-Care-Delivery-System 1Wilma Nierva BeraldeNo ratings yet
- Economic Impacts of Coronavirus Disease (COVID-19) in Developing CountriesDocument9 pagesEconomic Impacts of Coronavirus Disease (COVID-19) in Developing CountriesKyla Mae CastilloNo ratings yet
- CD59 11 e Strategy Resilent Health Post Covid 19Document21 pagesCD59 11 e Strategy Resilent Health Post Covid 19Estefania MatasNo ratings yet
- CHN Lecture Module 2 The Health Care Delivery SystemDocument38 pagesCHN Lecture Module 2 The Health Care Delivery SystemALLAN KARL N. YNGENTENo ratings yet
- Primary Health Care I 2021Document13 pagesPrimary Health Care I 2021Galakpai KolubahNo ratings yet
- NSTP 2 Module 5 - Health-1Document42 pagesNSTP 2 Module 5 - Health-1andrea arapocNo ratings yet
- NCM 104 Lecture Chapter 2.1 Health-Care-Delivery-SystemDocument112 pagesNCM 104 Lecture Chapter 2.1 Health-Care-Delivery-SystemWilma Nierva BeraldeNo ratings yet
- Health and DevelopmentDocument20 pagesHealth and DevelopmentZinhle MthembuNo ratings yet
- Noh 2016Document149 pagesNoh 2016ryuurecca100% (1)
- Current Status of Health and Disease Burden in IndiaDocument23 pagesCurrent Status of Health and Disease Burden in IndiaKavi rajput100% (1)
- Lecture Notes On NUCM 104Document10 pagesLecture Notes On NUCM 104Ciedelle Honey Lou DimaligNo ratings yet
- CHN 1 FullDocument88 pagesCHN 1 FullKristine Joy CamusNo ratings yet
- Primary Health CareDocument5 pagesPrimary Health CareYashoda AmarasekeraNo ratings yet
- Health Care System SendDocument113 pagesHealth Care System SendAsma AsriNo ratings yet
- Unveiling the Weaknesses: An Analysis of the World Health Organization's COVID-19 ResponseFrom EverandUnveiling the Weaknesses: An Analysis of the World Health Organization's COVID-19 ResponseNo ratings yet
- Certification From Hospital/ Institution Form: Last Name, First Name, Middle InitialDocument1 pageCertification From Hospital/ Institution Form: Last Name, First Name, Middle InitialJay-Anne RapanoNo ratings yet
- Manulife Affluence Max GoldDocument2 pagesManulife Affluence Max GoldJay-Anne RapanoNo ratings yet
- Office: of The SecretaryDocument1 pageOffice: of The SecretaryJay-Anne RapanoNo ratings yet
- Virtual LearningDocument6 pagesVirtual LearningJay-Anne RapanoNo ratings yet
- Manulife Affluence-Max-Elite BrochureDocument2 pagesManulife Affluence-Max-Elite BrochureJay-Anne RapanoNo ratings yet
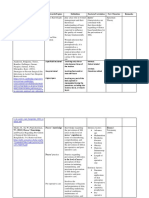
- Reference Keywords/Topics Factors/Correlates New Theories RemarksDocument5 pagesReference Keywords/Topics Factors/Correlates New Theories RemarksJay-Anne RapanoNo ratings yet
- Manulife Affluence BuilderDocument2 pagesManulife Affluence BuilderJay-Anne RapanoNo ratings yet
- Thyroid Cancer Case StudyDocument6 pagesThyroid Cancer Case StudyJay-Anne RapanoNo ratings yet
- Neonatal HematologyDocument83 pagesNeonatal HematologyJay-Anne RapanoNo ratings yet
- School of Health Sciences St. Paul University Philippines: Tuguegarao City, 3500Document2 pagesSchool of Health Sciences St. Paul University Philippines: Tuguegarao City, 3500Jay-Anne RapanoNo ratings yet
- School of Health Sciences St. Paul University Philippines: Tuguegarao City, 3500Document2 pagesSchool of Health Sciences St. Paul University Philippines: Tuguegarao City, 3500Jay-Anne RapanoNo ratings yet
- First PageDocument6 pagesFirst PageJay-Anne RapanoNo ratings yet
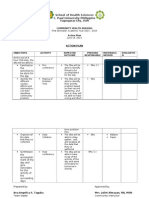
- Saint Paul University Philippines: Objectives Activity Time Frame Expected Outcome Materials Persons ResponsibleDocument2 pagesSaint Paul University Philippines: Objectives Activity Time Frame Expected Outcome Materials Persons ResponsibleJay-Anne RapanoNo ratings yet
- Saint Paul University Philippines: Tuguegarao City, Cagayan, 3500 A.Y. 2011-2012Document2 pagesSaint Paul University Philippines: Tuguegarao City, Cagayan, 3500 A.Y. 2011-2012Jay-Anne RapanoNo ratings yet
- St. Paul University Philippines: Tuguegarao City, Cagayan 3500 School of Health Sciences College of NursingDocument1 pageSt. Paul University Philippines: Tuguegarao City, Cagayan 3500 School of Health Sciences College of NursingJay-Anne RapanoNo ratings yet
- (Nakakaranas Ka Ba NG?) Masakit Lumunok) : Health Declaration TemperatureDocument1 page(Nakakaranas Ka Ba NG?) Masakit Lumunok) : Health Declaration TemperatureNatividad Jo Ann CuadroNo ratings yet
- Correspondence: Screening and Triage at Health-Care Facilities in Timor-Leste During The COVID-19 PandemicDocument1 pageCorrespondence: Screening and Triage at Health-Care Facilities in Timor-Leste During The COVID-19 PandemicdlundaNo ratings yet
- Covid 19 PDFDocument117 pagesCovid 19 PDFvicky anandNo ratings yet
- E-Module Listening BetterDocument92 pagesE-Module Listening BetterAnisa Putri RahmawatiNo ratings yet
- (ENG) Research Article - Pramadita Widya Garini - Imanuel Soni TanudjayaDocument10 pages(ENG) Research Article - Pramadita Widya Garini - Imanuel Soni TanudjayaImanuel SoniNo ratings yet
- National Youth Service CorpsDocument2 pagesNational Youth Service CorpsEngr Jay WhyNo ratings yet
- Disaster Triage Forgotten Lessons in Pandemic Covid-19 Management - Dr. Yogi Prabowo, SpOT (K)Document23 pagesDisaster Triage Forgotten Lessons in Pandemic Covid-19 Management - Dr. Yogi Prabowo, SpOT (K)Clara EverlastNo ratings yet
- Health Declaration Form (Annex A2) - KoronadalDocument3 pagesHealth Declaration Form (Annex A2) - KoronadalJephte MantalabaNo ratings yet
- FLCCC Alliance I MASKplus Protocol ENGLISHDocument2 pagesFLCCC Alliance I MASKplus Protocol ENGLISHnimrod20032003No ratings yet
- Assignment Strategic Human Resource Management: SUBMITTED TO: Ms. Asvir NaveedDocument6 pagesAssignment Strategic Human Resource Management: SUBMITTED TO: Ms. Asvir NaveedMuniza UsmanNo ratings yet
- Rizal Exam TipayEmelieDocument4 pagesRizal Exam TipayEmelieEmelie TipayNo ratings yet
- Editorial Commentary On The Indian Journal of Gastroenterology May-June 2020Document3 pagesEditorial Commentary On The Indian Journal of Gastroenterology May-June 2020sivagiri.pNo ratings yet
- DOH FebruaryDocument3 pagesDOH FebruaryMingNo ratings yet
- Tiara Puspita Dan Zahara Ilmiah SafitriDocument17 pagesTiara Puspita Dan Zahara Ilmiah SafitriTiara Puspita keperawatanNo ratings yet
- SAFETY MANAGEMENT SchholDocument4 pagesSAFETY MANAGEMENT SchholMikaNo ratings yet
- Research Chapter 1 5Document79 pagesResearch Chapter 1 5Nichole John Ernieta50% (2)
- Preprints Review 1marzoDocument61 pagesPreprints Review 1marzoJorgelina BernetNo ratings yet
- Family Escapes Death: Ti Gonzi Quits Drugs: Robbed During DemolitionsDocument16 pagesFamily Escapes Death: Ti Gonzi Quits Drugs: Robbed During DemolitionsAndrew JoriNo ratings yet
- Dear Citizen - Magarpatta City - Covid - 19 Emailer PDFDocument1 pageDear Citizen - Magarpatta City - Covid - 19 Emailer PDFPraveen KumarNo ratings yet
- CER - Description and Practice (ACE 2)Document2 pagesCER - Description and Practice (ACE 2)NunuNo ratings yet
- Guidelines Form Teledentistry 2020Document5 pagesGuidelines Form Teledentistry 2020Fery AnnNo ratings yet
- Covid19 Diagnosticproducts List enDocument54 pagesCovid19 Diagnosticproducts List enAmir Atef AhmedNo ratings yet
- Crew Change Procedures NPLDocument11 pagesCrew Change Procedures NPLMarsellus HakimNo ratings yet
- Chen Et Al., 2015 Sancar Et Al., 2018Document2 pagesChen Et Al., 2015 Sancar Et Al., 2018Sheryl Ann Barit PedinesNo ratings yet
- Missouri v. People's Republic of China - ComplaintDocument47 pagesMissouri v. People's Republic of China - ComplaintFox News88% (8)
- Homeopathy Covid-19 Part-3Document86 pagesHomeopathy Covid-19 Part-3deextlvlr vellore100% (1)
- Peac School Recovery and Readiness Plan FOR SCHOOLYEAR 2020-2021Document20 pagesPeac School Recovery and Readiness Plan FOR SCHOOLYEAR 2020-2021Anicadlien Ellipaw IninNo ratings yet
- Lompoc FCC Class Action Unlabeled Document 0000005Document34 pagesLompoc FCC Class Action Unlabeled Document 0000005Dave MinskyNo ratings yet