Download as pdf or txt
You might also like
- Test Bank For Human Diseases 8th Edition ZelmanDocument22 pagesTest Bank For Human Diseases 8th Edition Zelmandenisedanielsbkgqyzmtr100% (36)
- Test Banks Gary PersingDocument35 pagesTest Banks Gary PersingAlexander Santiago ParelNo ratings yet
- Your Breath On Yoga: The Anatomy & Physiology of Breathing for Teachers and Students of YogaFrom EverandYour Breath On Yoga: The Anatomy & Physiology of Breathing for Teachers and Students of YogaNo ratings yet
- John PFTDocument231 pagesJohn PFTAlexander Santiago ParelNo ratings yet
- Lecture 1 - Development of Respiratory SystemDocument27 pagesLecture 1 - Development of Respiratory SystemRachmad MusyaffaNo ratings yet
- Development of Respiratory System: Dr. Saeed Vohra & Dr. Sanaa AlshaarawyDocument26 pagesDevelopment of Respiratory System: Dr. Saeed Vohra & Dr. Sanaa AlshaarawyChristineNo ratings yet
- Embryology of Heart and LungDocument7 pagesEmbryology of Heart and Lungavinash dhameriyaNo ratings yet
- Intrauterine Development: Premidterm CoverageDocument14 pagesIntrauterine Development: Premidterm Coverageaidan udjamanNo ratings yet
- Developmental Biology of The Pulmonary Circulation: Alison HislopDocument10 pagesDevelopmental Biology of The Pulmonary Circulation: Alison HislopMarcela RodriguezNo ratings yet
- Neonatology: Addisu Aa (Lecturer, MSC in CM)Document35 pagesNeonatology: Addisu Aa (Lecturer, MSC in CM)Abiy AliyeNo ratings yet
- Neonatal Respiratory Care NotesDocument136 pagesNeonatal Respiratory Care NotesJade Louise FkshmNo ratings yet
- Neonatal Respiration PhysiologyDocument6 pagesNeonatal Respiration PhysiologyRaja Ahmad Rusdan MusyawirNo ratings yet
- Development of Respiratory System and Its AnomaliesDocument17 pagesDevelopment of Respiratory System and Its AnomaliesmichaelqurtisNo ratings yet
- Lec 4Document6 pagesLec 4ibrahim.21hm32No ratings yet
- Embryology 4Document18 pagesEmbryology 4hauwauyusufmaijeddahNo ratings yet
- Pulmonary EmbolismDocument21 pagesPulmonary EmbolismMadhu Bala100% (2)
- Report Cluster 4Document111 pagesReport Cluster 4Jelmalyn BasaliNo ratings yet
- All About RespiratoryDocument69 pagesAll About RespiratoryMarcellina Awing100% (1)
- 1 (Lung Development)Document12 pages1 (Lung Development)Dr.sonuNo ratings yet
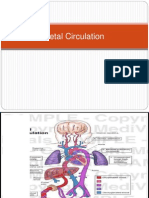
- Fetal CirculationDocument39 pagesFetal CirculationjerlinNo ratings yet
- Ultrasound in Obstet Gyne - 2002 - Laudy - The Fetal Lung 1 Developmental AspectsDocument7 pagesUltrasound in Obstet Gyne - 2002 - Laudy - The Fetal Lung 1 Developmental AspectsRafael JustinoNo ratings yet
- Normal Fetal Growth and DevelopmentDocument38 pagesNormal Fetal Growth and DevelopmentArhum SiddiqiNo ratings yet
- LP BBLDocument21 pagesLP BBLSalsabilla KimikoNo ratings yet
- 3.embryonic & Fetal Period 1st Yr MedcDocument34 pages3.embryonic & Fetal Period 1st Yr MedcTofik MohammedNo ratings yet
- The Respiratory System: Supplement To Text, Chapter 9Document77 pagesThe Respiratory System: Supplement To Text, Chapter 9Christina GonezNo ratings yet
- 2 Paediatrics and Neonatal AnesthesiaDocument87 pages2 Paediatrics and Neonatal Anesthesiahailemichael chekolNo ratings yet
- Module 3 Fetal DevelopmentDocument7 pagesModule 3 Fetal DevelopmentRichel TalattagNo ratings yet
- Extraembryonic MembraneDocument41 pagesExtraembryonic MembraneDangkoNo ratings yet
- Transitory Neonatal Status: Karazin Kharkiv National University Department of PediatricsDocument51 pagesTransitory Neonatal Status: Karazin Kharkiv National University Department of PediatricsSiddhartha MohapatraNo ratings yet
- Lung Development and Fetal CirculationDocument9 pagesLung Development and Fetal CirculationJade ProvidenceNo ratings yet
- Development of Respiratory SystemDocument46 pagesDevelopment of Respiratory SystemSusan SarkerNo ratings yet
- Fetal Circulation and Circulatory Changes at Birth - Pulei - 2024-05-03Document36 pagesFetal Circulation and Circulatory Changes at Birth - Pulei - 2024-05-03shemobaigwa79No ratings yet
- Development of Body Cavities and Diaphragm: Pleuro-Pericardial and Pleuro-Peritoneal MembraneDocument14 pagesDevelopment of Body Cavities and Diaphragm: Pleuro-Pericardial and Pleuro-Peritoneal MembraneÑäd ÉèmNo ratings yet
- Development of The Respiratory SystemDocument22 pagesDevelopment of The Respiratory SystemtuhinNo ratings yet
- Fetal Cardiopulmonary Development OutlineDocument7 pagesFetal Cardiopulmonary Development OutlineRLibdehNo ratings yet
- Introduction To Physiological Changes in NEONATAL AND PEDIATRIC RESPICARE James Astrologo LamusaoDocument88 pagesIntroduction To Physiological Changes in NEONATAL AND PEDIATRIC RESPICARE James Astrologo LamusaoDanao, Aira A.No ratings yet
- Embryo. Lec.2 Larynx, Trachea and LungsDocument11 pagesEmbryo. Lec.2 Larynx, Trachea and Lungsزينب فؤاد موسىNo ratings yet
- 12 Lung DevelopmentDocument36 pages12 Lung Developmentf3er3No ratings yet
- Fertilization: Glora P. de Leon, RN, RM, ManDocument103 pagesFertilization: Glora P. de Leon, RN, RM, ManJoan VillafrancaNo ratings yet
- Development of Respiratory SDocument35 pagesDevelopment of Respiratory SMunewer AbdellaNo ratings yet
- Corticosteroid in Lung MaturationDocument12 pagesCorticosteroid in Lung Maturationtommy japolaNo ratings yet
- Embryologi OF The Respiratory System: Arti Rosaria Dewi, DRDocument60 pagesEmbryologi OF The Respiratory System: Arti Rosaria Dewi, DRAsti NuriatiNo ratings yet
- Pedia Pulmo 1Document129 pagesPedia Pulmo 1Sven OrdanzaNo ratings yet
- Pedia Pulmo 1Document129 pagesPedia Pulmo 1Sven OrdanzaNo ratings yet
- Adaption of Infants To Extra-Uterine LifeDocument10 pagesAdaption of Infants To Extra-Uterine LifeJulienne QuintaoNo ratings yet
- Physiology AssignmentDocument9 pagesPhysiology AssignmentArsh NazNo ratings yet
- Development of Respiratory SystemDocument34 pagesDevelopment of Respiratory SystemNatalie HuiNo ratings yet
- Fetal CirculationDocument28 pagesFetal CirculationNelai GoNo ratings yet
- Fetal and Neonatal Physiology PDFDocument33 pagesFetal and Neonatal Physiology PDFObsaNo ratings yet
- PBL 2 KLP 9aDocument40 pagesPBL 2 KLP 9aPutri ReniNo ratings yet
- Maternal and Child Health Nursing (NCM 101 Lect) Part 1Document4 pagesMaternal and Child Health Nursing (NCM 101 Lect) Part 1yunjung0518100% (7)
- 3-Embryology of Respiratory SystemDocument25 pages3-Embryology of Respiratory SystemNur HikmahNo ratings yet
- Embryology Respiratory System: Formation of Lung BudsDocument1 pageEmbryology Respiratory System: Formation of Lung Budsrezairfan221No ratings yet
- Update Fetal Circulation - MDM AmyDocument10 pagesUpdate Fetal Circulation - MDM AmyNana Yunus100% (1)
- Embryo Development Lungs+Body CavityDocument8 pagesEmbryo Development Lungs+Body CavityKingNo ratings yet
- Human Reproduction-13 - May 21Document72 pagesHuman Reproduction-13 - May 21Upal PramanickNo ratings yet
- 11th Lecture Amnion& Amniotic FluidDocument35 pages11th Lecture Amnion& Amniotic FluidHussein Al Saedi100% (1)
- Chapter 3 (Final)Document14 pagesChapter 3 (Final)Pureza Maye SalapangNo ratings yet
- Stages of Fetal DevelopmentDocument92 pagesStages of Fetal DevelopmentMelissa Diego-sarmiento100% (1)
- Pulmonary diseases.pdfDocument70 pagesPulmonary diseases.pdfBella GreyNo ratings yet
- PlacentaDocument21 pagesPlacentaAttiqaQureshiNo ratings yet
- Bronchioles Then Divide Into Three TypesDocument3 pagesBronchioles Then Divide Into Three TypesJeremy EvansNo ratings yet
- Observations on Abortion: Containing an account of the manner in which it is accomplished, the causes which produced it, and the method of preventing or treating itFrom EverandObservations on Abortion: Containing an account of the manner in which it is accomplished, the causes which produced it, and the method of preventing or treating itNo ratings yet
- Pulmo HPNDocument36 pagesPulmo HPNAlexander Santiago ParelNo ratings yet
- MountaiNut Back LabelDocument1 pageMountaiNut Back LabelAlexander Santiago ParelNo ratings yet
- Printable Water Color Quote BookmarksDocument1 pagePrintable Water Color Quote BookmarksAlexander Santiago ParelNo ratings yet
- A Genealogical Analysis of PassivityDocument145 pagesA Genealogical Analysis of PassivityAlexander Santiago ParelNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument45 pagesChronic Obstructive Pulmonary DiseaseAlexander Santiago ParelNo ratings yet
- Thesis Manuscript - UIGANDocument110 pagesThesis Manuscript - UIGANAlexander Santiago Parel100% (1)
- Sleep ApneaDocument14 pagesSleep ApneaAlexander Santiago ParelNo ratings yet
- Pleural EffDocument30 pagesPleural EffAlexander Santiago ParelNo ratings yet
- Pulmo ThromboembolismDocument34 pagesPulmo ThromboembolismAlexander Santiago ParelNo ratings yet
- ABG and Oximetry StudentDocument86 pagesABG and Oximetry StudentAlexander Santiago ParelNo ratings yet
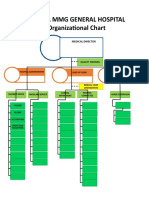
- Hospital Organizational ChartDocument1 pageHospital Organizational ChartAlexander Santiago ParelNo ratings yet
- Group 8Document15 pagesGroup 8Alexander Santiago ParelNo ratings yet
- Treatment of Tuberculosis .2Document59 pagesTreatment of Tuberculosis .2Alexander Santiago Parel0% (1)
- Pathophysiology of Tuberculosis: Group 5 Latosa, Selene Lee, Guk Lim, Johanna Magalona, Stephen Mendoza, ColeenDocument22 pagesPathophysiology of Tuberculosis: Group 5 Latosa, Selene Lee, Guk Lim, Johanna Magalona, Stephen Mendoza, ColeenAlexander Santiago ParelNo ratings yet
- Thesis Manuscript - UIGANDocument110 pagesThesis Manuscript - UIGANAlexander Santiago Parel100% (1)
- Bio Medical Instrumentation EE045Document8 pagesBio Medical Instrumentation EE045Varun ManoharanNo ratings yet
- Standardized Echo Report Rev1Document38 pagesStandardized Echo Report Rev1dgina8800100% (1)
- Electrical Safety A Guide To The Causes and Prevention of Electrical Hazards by Adams, J. MaxwellDocument204 pagesElectrical Safety A Guide To The Causes and Prevention of Electrical Hazards by Adams, J. Maxwellasdqwe999No ratings yet
- A Head Nurse Oversees Nursing Activities in A Range of Health Care SettingsDocument8 pagesA Head Nurse Oversees Nursing Activities in A Range of Health Care SettingsMitch MaLagambaNo ratings yet
- aLL MCQS AMALI WEEKLYDocument58 pagesaLL MCQS AMALI WEEKLYWajiha ZahraNo ratings yet
- Severe Residual Pulmonary Stenosis After Surgical Repair of Tetralogy of Fallot: What's Our Next Strategy?Document11 pagesSevere Residual Pulmonary Stenosis After Surgical Repair of Tetralogy of Fallot: What's Our Next Strategy?International Journal of Innovative Science and Research TechnologyNo ratings yet
- Wiggers Diagram SlidesDocument15 pagesWiggers Diagram SlidesKuro ShiroNo ratings yet
- Mechanical Function of The HeartDocument28 pagesMechanical Function of The HeartKarmilahNNo ratings yet
- Point of Care Ultrasound For The ClinicalDocument14 pagesPoint of Care Ultrasound For The Clinical凌晓敏No ratings yet
- Module 18 Respiratory FinalDocument15 pagesModule 18 Respiratory FinalJayR MendonesNo ratings yet
- MCQ'S BankDocument38 pagesMCQ'S BankAishwarya Bharath100% (1)
- Xcelera Brochure Updated (English)Document24 pagesXcelera Brochure Updated (English)Pablo Rosas100% (1)
- TransportationDocument58 pagesTransportatione-SayutiNo ratings yet
- Contemporary Perioperative Haemodynamic MonitoringDocument12 pagesContemporary Perioperative Haemodynamic MonitoringrjerezrNo ratings yet
- Cardiovascular System - Printable Pages - MariebDocument6 pagesCardiovascular System - Printable Pages - MariebChristal Rae Tac-anNo ratings yet
- RRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRDocument2 pagesRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRSaginesh MkNo ratings yet
- January 2018 (IAL) QP - Unit 1 Edexcel Biology A-LevelDocument24 pagesJanuary 2018 (IAL) QP - Unit 1 Edexcel Biology A-LevelGhaziaNo ratings yet
- Chapter 6 Q. P.1Document28 pagesChapter 6 Q. P.1RawanMazen SharifNo ratings yet
- Bio4 6Document17 pagesBio4 6HarmonyChui100% (1)
- Bmi-2 MarksDocument16 pagesBmi-2 MarksmohanapriyaNo ratings yet
- Yuson, Jasmine Kaye C. BA Political Science-3 Zoo Lec MWF 1-2pmDocument3 pagesYuson, Jasmine Kaye C. BA Political Science-3 Zoo Lec MWF 1-2pmJasmine YusonNo ratings yet
- Ultrasound in Obstet Gyne - 2022 - PaladiniDocument8 pagesUltrasound in Obstet Gyne - 2022 - PaladiniKarim Muñoz NiñoNo ratings yet
- Unit 6Document32 pagesUnit 6Bharat ThapaNo ratings yet
- Cap 5 - Monitorización CardiovascularDocument53 pagesCap 5 - Monitorización CardiovascularMonserrath ReséndizNo ratings yet
- Chapter: Body Fluids and Circulation: BIOLOGY - AssignmentDocument8 pagesChapter: Body Fluids and Circulation: BIOLOGY - Assignmentyogesh ahireNo ratings yet
- Introduction To First Aid & The Humand BodyDocument50 pagesIntroduction To First Aid & The Humand BodyEmil Vince T. CumilangNo ratings yet
- Does Obesity Influence Early Target Organ Damage in Hypertensive PatientsDocument8 pagesDoes Obesity Influence Early Target Organ Damage in Hypertensive PatientsHenri TantyokoNo ratings yet
- Pig Heart Dissection LabDocument6 pagesPig Heart Dissection LabLAUREN JENELLE ABLANG100% (1)
- CardiovascularDocument16 pagesCardiovascularMilena VargasNo ratings yet