
Handand Wrist Exammaster
Handand Wrist Exammaster
You might also like
- Detroit Receiving Hospital Emergency Medicine Handbook 5th EdnDocument341 pagesDetroit Receiving Hospital Emergency Medicine Handbook 5th EdnElham Alsamahi100% (1)
- Basic Orthopedic HardwareDocument13 pagesBasic Orthopedic HardwareJennifer C. SumadsadNo ratings yet
- 43 - Zlowodzki - Flexor Tendon Injuries of The HandDocument94 pages43 - Zlowodzki - Flexor Tendon Injuries of The HandGobinath KannanNo ratings yet
- Mnemonic For Forearm Muscles and BoneDocument2 pagesMnemonic For Forearm Muscles and BoneLaura Tapia89% (28)
- Examination of Hand & Common Hand InjuriesDocument165 pagesExamination of Hand & Common Hand InjuriesPriya GK100% (1)
- 9 Orthopaedic EmergenciesDocument68 pages9 Orthopaedic EmergenciesAndrew WdsmithNo ratings yet
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Trigger Finger, A Simple Guide to The Condition, Treatment And Related DisordersFrom EverandTrigger Finger, A Simple Guide to The Condition, Treatment And Related DisordersNo ratings yet
- Reduction, Relocation and Splinting in Emergency Room (RASER)From EverandReduction, Relocation and Splinting in Emergency Room (RASER)No ratings yet
- DeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Claw Hand, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandClaw Hand, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 4 out of 5 stars4/5 (1)
- A Simple Guide to Extensor Tendonitis, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Extensor Tendonitis, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Flexor Tendon Injuries SeminarDocument75 pagesFlexor Tendon Injuries SeminarAmit GoyalNo ratings yet
- IvdpDocument89 pagesIvdpFelix Sabu100% (1)
- SG3 Ortho PresentationDocument199 pagesSG3 Ortho PresentationPrincess Noreen SavellanoNo ratings yet
- Evaluation of The Hand!Document84 pagesEvaluation of The Hand!Ahmad A. Fannoon100% (1)
- Hand and WristDocument5 pagesHand and WristcpNo ratings yet
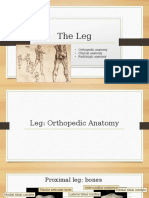
- The Leg: - Orthopedic Anatomy - Clinical Anatomy - Radiologic AnatomyDocument50 pagesThe Leg: - Orthopedic Anatomy - Clinical Anatomy - Radiologic Anatomyspeedy.catNo ratings yet
- Gpe - 017.1 - Orthopaedic ExaminationDocument3 pagesGpe - 017.1 - Orthopaedic ExaminationImiey Eleena HanumNo ratings yet
- Anterior Cruciate Ligament Reconstruction: Mardani Kivi M. M.D. Presentation Designed For Nurses EducationDocument31 pagesAnterior Cruciate Ligament Reconstruction: Mardani Kivi M. M.D. Presentation Designed For Nurses EducationNurul FajriNo ratings yet
- Achilles Tendon RuptureDocument6 pagesAchilles Tendon RuptureBn Wahyu AjiNo ratings yet
- Orthopaedic Instruments and ImplantsDocument21 pagesOrthopaedic Instruments and ImplantsgibreilNo ratings yet
- Distal Femur (Sandeep Sir)Document22 pagesDistal Femur (Sandeep Sir)Kirubakaran Saraswathy PattabiramanNo ratings yet
- Knee PathoDocument32 pagesKnee PathoAilee Gliezl Milanie MontemayorNo ratings yet
- Hip Joint: 5 December 2016 Anatomy Lecture By: DR Anita RaniDocument38 pagesHip Joint: 5 December 2016 Anatomy Lecture By: DR Anita RaniDr'Dinesh MishraNo ratings yet
- Tennis ElbowDocument13 pagesTennis ElbowPadma PadalNo ratings yet
- Shoulder ExamDocument12 pagesShoulder Examckyew64No ratings yet
- Patellar InstabilityDocument16 pagesPatellar InstabilitydrjorgewtorresNo ratings yet
- Neurological Complications in Lumbar Spine SurgeryDocument9 pagesNeurological Complications in Lumbar Spine SurgeryMimi SyakilaNo ratings yet
- Flexor Tendon Injuries: DR Manoj Kumar OrtopaedicsDocument50 pagesFlexor Tendon Injuries: DR Manoj Kumar OrtopaedicsManoj Kumar100% (1)
- A Regional Approach To Foot and Ankle MRIDocument17 pagesA Regional Approach To Foot and Ankle MRInior100% (1)
- Practical Techniques in Injury Management: Casts and SplintsDocument30 pagesPractical Techniques in Injury Management: Casts and SplintsBodescu Adrian100% (1)
- B 756 Vertebris GB III10Document44 pagesB 756 Vertebris GB III10Lukasz Bartochowski100% (1)
- Total Knee Replacement: The Path ToDocument6 pagesTotal Knee Replacement: The Path ToMoses DhinakarNo ratings yet
- Spondylolysis SpondylolisthesisDocument89 pagesSpondylolysis SpondylolisthesisAh ZhangNo ratings yet
- Postoperative Management of Flexor Tendon InjuriesDocument232 pagesPostoperative Management of Flexor Tendon InjuriesAhmad A. Fannoon100% (3)
- Special Tests in Shoulder ExaminationDocument28 pagesSpecial Tests in Shoulder Examinationthwiseman100% (1)
- Ankle Stability and MovementDocument40 pagesAnkle Stability and MovementBogdan GeangosNo ratings yet
- Rotator Cuff InjuryDocument29 pagesRotator Cuff InjuryArko duttaNo ratings yet
- Crozer-Keystone Ex Tern Ship ManualDocument187 pagesCrozer-Keystone Ex Tern Ship ManualRihamary CruzNo ratings yet
- Handout Lat Elbow Pain PDFDocument47 pagesHandout Lat Elbow Pain PDFgemichan26No ratings yet
- 1 Evidence Based Examination and Intervention of The Hip JointDocument10 pages1 Evidence Based Examination and Intervention of The Hip JointRicha GahuniaNo ratings yet
- Orthopaedic SlidesDocument163 pagesOrthopaedic SlidesVivian ChepkemeiNo ratings yet
- Orthopaedic Physical ExaminationDocument94 pagesOrthopaedic Physical ExaminationPriza RazunipNo ratings yet
- Shoulder Arthroscopy Presentation v0.4Document20 pagesShoulder Arthroscopy Presentation v0.4Mohammad Nasfikur Rahman KhanNo ratings yet
- Computer Aided Diagnosis System For Lumbar Spinal Stenosis Using X-Ray ImagesDocument45 pagesComputer Aided Diagnosis System For Lumbar Spinal Stenosis Using X-Ray Imagesroky100% (1)
- Elbow Fractures in PediatricsDocument57 pagesElbow Fractures in PediatricsKalaichelviRegunathan100% (1)
- Hand PDFDocument179 pagesHand PDFRadenSiwi Bagus HadhiningratNo ratings yet
- Shoulder Arthroscopy Patient Education Packet RayappaDocument5 pagesShoulder Arthroscopy Patient Education Packet Rayappaapi-549337910No ratings yet
- Lower Limb FracturesDocument124 pagesLower Limb Fracturesmau tau100% (1)
- Distal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurDocument76 pagesDistal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurToàn Đặng Phan VĩnhNo ratings yet
- Traction in OrthopaedicDocument32 pagesTraction in OrthopaedicFarry Doank100% (1)
- Spine Examination: Mario Johan Heryputra 11.2012.208Document29 pagesSpine Examination: Mario Johan Heryputra 11.2012.208Mario Johan Heryputra100% (1)
- Week 2 Ortho Tests Figure NoDocument14 pagesWeek 2 Ortho Tests Figure Noapi-468597987100% (1)
- The Anatomy and Surgical Approach of ForearmDocument25 pagesThe Anatomy and Surgical Approach of Forearmamel015100% (1)
- C SpineDocument33 pagesC SpineKarthickNo ratings yet
- Low Back PainDocument8 pagesLow Back PainLev KalikaNo ratings yet
- Ankle Fractures - A Logical Approach To Their FixationDocument48 pagesAnkle Fractures - A Logical Approach To Their FixationRoman MosneagaNo ratings yet
- Wrist Drop Claw Hand Median Nerve Palsy: Dr. Srivatsa.NDocument46 pagesWrist Drop Claw Hand Median Nerve Palsy: Dr. Srivatsa.NMurali KarthikkNo ratings yet
- Peripheral Nerve Injuries: Nerve Connective Tissue Nervous SystemDocument70 pagesPeripheral Nerve Injuries: Nerve Connective Tissue Nervous SystemRupika SodhiNo ratings yet
- Dr. Ankit Gujarathi DMH PuneDocument32 pagesDr. Ankit Gujarathi DMH PuneAnkit GujarathiNo ratings yet
- Electrotherapy: Clinical CasesDocument18 pagesElectrotherapy: Clinical CasesjothiNo ratings yet
- Presented By: DR - Shilpa K PrajapatiDocument46 pagesPresented By: DR - Shilpa K PrajapatijothiNo ratings yet
- Bedside Clinics IVDocument10 pagesBedside Clinics IVjothi100% (2)
- 2-Lab Activities - Electrotherapy Application ProceduresDocument13 pages2-Lab Activities - Electrotherapy Application ProceduresjothiNo ratings yet
- Medium Frequency: Interferential TherapyDocument31 pagesMedium Frequency: Interferential TherapyjothiNo ratings yet
- DR - Sanyal Kumar JR Dept of PMRDocument25 pagesDR - Sanyal Kumar JR Dept of PMRjothiNo ratings yet
- Assistive Technology Presentation Braille 1226057512134632 8Document12 pagesAssistive Technology Presentation Braille 1226057512134632 8jothiNo ratings yet
- Evaluating Core Stability: Reliability and Validity of Hand-Held Dynamometry in Measuring Core StrengthDocument50 pagesEvaluating Core Stability: Reliability and Validity of Hand-Held Dynamometry in Measuring Core StrengthjothiNo ratings yet
- Peripheral Nerve Injuries: DR - Prateek Singh Intern Dept. of Orthopaedics BpkihsDocument29 pagesPeripheral Nerve Injuries: DR - Prateek Singh Intern Dept. of Orthopaedics BpkihsjothiNo ratings yet
- Pre and Post Operative Physiotherapy Management in Tendon Transfer of HandDocument59 pagesPre and Post Operative Physiotherapy Management in Tendon Transfer of HandjothiNo ratings yet
- Journal of BiomechanicsDocument11 pagesJournal of BiomechanicsjothiNo ratings yet
- Journal of BiomechanicsDocument10 pagesJournal of BiomechanicsjothiNo ratings yet
- Physeal Injuries: Dr. Bassey, A E Orthopaedic & Trauma Surgery U.A.T.H, AbujaDocument30 pagesPhyseal Injuries: Dr. Bassey, A E Orthopaedic & Trauma Surgery U.A.T.H, AbujajothiNo ratings yet
- Therapeutic Exercise NotesDocument288 pagesTherapeutic Exercise NotesMarysav100% (1)
- Qdoc - Tips - Muscles of The Upper Limb Made EasyDocument7 pagesQdoc - Tips - Muscles of The Upper Limb Made EasyAkomolede AbosedeNo ratings yet
- Osteology BonesDocument48 pagesOsteology BonesÂhmęd ĐoolaNo ratings yet
- 13-Hand & WristDocument10 pages13-Hand & Wristzain juttNo ratings yet
- 2k19 Anatomy CA 1Document10 pages2k19 Anatomy CA 1Tofunmi AdegokeNo ratings yet
- Kewenangan Klinis Dr. Ayiq, Sp. OTDocument12 pagesKewenangan Klinis Dr. Ayiq, Sp. OTGestiNo ratings yet
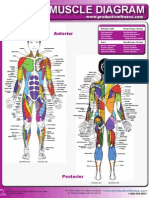
- Female Muscle DiagramDocument1 pageFemale Muscle DiagrammakukikiNo ratings yet
- Module 6 - Muscular System Part 4 StudentDocument41 pagesModule 6 - Muscular System Part 4 StudentLaw HacksNo ratings yet
- Anatomy (Stockoe) For Mini NotesDocument86 pagesAnatomy (Stockoe) For Mini NotesIvy Dianne PascualNo ratings yet
- Some Good MnemonicsDocument6 pagesSome Good MnemonicsMehdi BaigNo ratings yet
- Diseases of The Horse's Foot by Reeks, Harry CaultonDocument282 pagesDiseases of The Horse's Foot by Reeks, Harry CaultonGutenberg.org100% (1)
- Locomotor - Hand Clinical Mark SheetDocument7 pagesLocomotor - Hand Clinical Mark SheetDrShamshad KhanNo ratings yet
- 27 Feature Extraction and Classifier in The Development of Exoskeleton Based On Emg Signal Control A ReviewDocument7 pages27 Feature Extraction and Classifier in The Development of Exoskeleton Based On Emg Signal Control A ReviewTriwiyanto TriwiyantoNo ratings yet
- Single Choice Questions in ORTHOPAEDICS Mahmood A Sulaiman: January 2019Document186 pagesSingle Choice Questions in ORTHOPAEDICS Mahmood A Sulaiman: January 2019Kiran Kumar100% (1)
- Tendon TransfersDocument194 pagesTendon Transferschinthaka_wijedasa100% (4)
- Decoding Arm Movements by Myoeletric Signals and Artificial Neural NetworksDocument6 pagesDecoding Arm Movements by Myoeletric Signals and Artificial Neural NetworksAnurag SharmaNo ratings yet
- Anatomia de PiermatteiDocument5 pagesAnatomia de PiermatteiFernando Melo GarciaNo ratings yet
- Donald A. Neumann - Kinesiology of The Musculoskeletal System 3rd Edition (2018, ELSEVIER) - Libgen - Li-P Íginas-9Document40 pagesDonald A. Neumann - Kinesiology of The Musculoskeletal System 3rd Edition (2018, ELSEVIER) - Libgen - Li-P Íginas-9ritaalmeida98No ratings yet
- 4 - Surgical Approaches To The Elbow 2012 Orthopaedics and TraumaDocument6 pages4 - Surgical Approaches To The Elbow 2012 Orthopaedics and TraumaProfesseur Christian DumontierNo ratings yet
- 1 Anatomy-MSKDocument86 pages1 Anatomy-MSKashim tiwariNo ratings yet
- TARO 2018 Corrigido e Com Referencias Final 1Document31 pagesTARO 2018 Corrigido e Com Referencias Final 1Isabella de OliveiraNo ratings yet
- Atlas of Orthopedic Surgical Procedures of The Dog and CatDocument244 pagesAtlas of Orthopedic Surgical Procedures of The Dog and Catשאול רייס100% (4)
- BooksDocument388 pagesBooksMayank GoyalNo ratings yet
- Exam Table For Hand Wrist ForearmDocument22 pagesExam Table For Hand Wrist ForearmLouie OkayNo ratings yet
- Buku-Anatomi Osteologi PDFDocument56 pagesBuku-Anatomi Osteologi PDFmuhammad firdausNo ratings yet
- Dr. Paredes: Upper Extremity of MSKDocument18 pagesDr. Paredes: Upper Extremity of MSKJose Emmanuel DolorNo ratings yet
- Osteology I: Bones of The Upper LimbDocument26 pagesOsteology I: Bones of The Upper LimbNaufalNo ratings yet
- Chapter 18Document182 pagesChapter 18ryllerylle05No ratings yet





































































































Download as pdf or txt
You might also like
- Detroit Receiving Hospital Emergency Medicine Handbook 5th EdnDocument341 pagesDetroit Receiving Hospital Emergency Medicine Handbook 5th EdnElham Alsamahi100% (1)
- Basic Orthopedic HardwareDocument13 pagesBasic Orthopedic HardwareJennifer C. SumadsadNo ratings yet
- 43 - Zlowodzki - Flexor Tendon Injuries of The HandDocument94 pages43 - Zlowodzki - Flexor Tendon Injuries of The HandGobinath KannanNo ratings yet
- Mnemonic For Forearm Muscles and BoneDocument2 pagesMnemonic For Forearm Muscles and BoneLaura Tapia89% (28)
- Examination of Hand & Common Hand InjuriesDocument165 pagesExamination of Hand & Common Hand InjuriesPriya GK100% (1)
- 9 Orthopaedic EmergenciesDocument68 pages9 Orthopaedic EmergenciesAndrew WdsmithNo ratings yet
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Trigger Finger, A Simple Guide to The Condition, Treatment And Related DisordersFrom EverandTrigger Finger, A Simple Guide to The Condition, Treatment And Related DisordersNo ratings yet
- Reduction, Relocation and Splinting in Emergency Room (RASER)From EverandReduction, Relocation and Splinting in Emergency Room (RASER)No ratings yet
- DeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Claw Hand, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandClaw Hand, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 4 out of 5 stars4/5 (1)
- A Simple Guide to Extensor Tendonitis, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Extensor Tendonitis, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Flexor Tendon Injuries SeminarDocument75 pagesFlexor Tendon Injuries SeminarAmit GoyalNo ratings yet
- IvdpDocument89 pagesIvdpFelix Sabu100% (1)
- SG3 Ortho PresentationDocument199 pagesSG3 Ortho PresentationPrincess Noreen SavellanoNo ratings yet
- Evaluation of The Hand!Document84 pagesEvaluation of The Hand!Ahmad A. Fannoon100% (1)
- Hand and WristDocument5 pagesHand and WristcpNo ratings yet
- The Leg: - Orthopedic Anatomy - Clinical Anatomy - Radiologic AnatomyDocument50 pagesThe Leg: - Orthopedic Anatomy - Clinical Anatomy - Radiologic Anatomyspeedy.catNo ratings yet
- Gpe - 017.1 - Orthopaedic ExaminationDocument3 pagesGpe - 017.1 - Orthopaedic ExaminationImiey Eleena HanumNo ratings yet
- Anterior Cruciate Ligament Reconstruction: Mardani Kivi M. M.D. Presentation Designed For Nurses EducationDocument31 pagesAnterior Cruciate Ligament Reconstruction: Mardani Kivi M. M.D. Presentation Designed For Nurses EducationNurul FajriNo ratings yet
- Achilles Tendon RuptureDocument6 pagesAchilles Tendon RuptureBn Wahyu AjiNo ratings yet
- Orthopaedic Instruments and ImplantsDocument21 pagesOrthopaedic Instruments and ImplantsgibreilNo ratings yet
- Distal Femur (Sandeep Sir)Document22 pagesDistal Femur (Sandeep Sir)Kirubakaran Saraswathy PattabiramanNo ratings yet
- Knee PathoDocument32 pagesKnee PathoAilee Gliezl Milanie MontemayorNo ratings yet
- Hip Joint: 5 December 2016 Anatomy Lecture By: DR Anita RaniDocument38 pagesHip Joint: 5 December 2016 Anatomy Lecture By: DR Anita RaniDr'Dinesh MishraNo ratings yet
- Tennis ElbowDocument13 pagesTennis ElbowPadma PadalNo ratings yet
- Shoulder ExamDocument12 pagesShoulder Examckyew64No ratings yet
- Patellar InstabilityDocument16 pagesPatellar InstabilitydrjorgewtorresNo ratings yet
- Neurological Complications in Lumbar Spine SurgeryDocument9 pagesNeurological Complications in Lumbar Spine SurgeryMimi SyakilaNo ratings yet
- Flexor Tendon Injuries: DR Manoj Kumar OrtopaedicsDocument50 pagesFlexor Tendon Injuries: DR Manoj Kumar OrtopaedicsManoj Kumar100% (1)
- A Regional Approach To Foot and Ankle MRIDocument17 pagesA Regional Approach To Foot and Ankle MRInior100% (1)
- Practical Techniques in Injury Management: Casts and SplintsDocument30 pagesPractical Techniques in Injury Management: Casts and SplintsBodescu Adrian100% (1)
- B 756 Vertebris GB III10Document44 pagesB 756 Vertebris GB III10Lukasz Bartochowski100% (1)
- Total Knee Replacement: The Path ToDocument6 pagesTotal Knee Replacement: The Path ToMoses DhinakarNo ratings yet
- Spondylolysis SpondylolisthesisDocument89 pagesSpondylolysis SpondylolisthesisAh ZhangNo ratings yet
- Postoperative Management of Flexor Tendon InjuriesDocument232 pagesPostoperative Management of Flexor Tendon InjuriesAhmad A. Fannoon100% (3)
- Special Tests in Shoulder ExaminationDocument28 pagesSpecial Tests in Shoulder Examinationthwiseman100% (1)
- Ankle Stability and MovementDocument40 pagesAnkle Stability and MovementBogdan GeangosNo ratings yet
- Rotator Cuff InjuryDocument29 pagesRotator Cuff InjuryArko duttaNo ratings yet
- Crozer-Keystone Ex Tern Ship ManualDocument187 pagesCrozer-Keystone Ex Tern Ship ManualRihamary CruzNo ratings yet
- Handout Lat Elbow Pain PDFDocument47 pagesHandout Lat Elbow Pain PDFgemichan26No ratings yet
- 1 Evidence Based Examination and Intervention of The Hip JointDocument10 pages1 Evidence Based Examination and Intervention of The Hip JointRicha GahuniaNo ratings yet
- Orthopaedic SlidesDocument163 pagesOrthopaedic SlidesVivian ChepkemeiNo ratings yet
- Orthopaedic Physical ExaminationDocument94 pagesOrthopaedic Physical ExaminationPriza RazunipNo ratings yet
- Shoulder Arthroscopy Presentation v0.4Document20 pagesShoulder Arthroscopy Presentation v0.4Mohammad Nasfikur Rahman KhanNo ratings yet
- Computer Aided Diagnosis System For Lumbar Spinal Stenosis Using X-Ray ImagesDocument45 pagesComputer Aided Diagnosis System For Lumbar Spinal Stenosis Using X-Ray Imagesroky100% (1)
- Elbow Fractures in PediatricsDocument57 pagesElbow Fractures in PediatricsKalaichelviRegunathan100% (1)
- Hand PDFDocument179 pagesHand PDFRadenSiwi Bagus HadhiningratNo ratings yet
- Shoulder Arthroscopy Patient Education Packet RayappaDocument5 pagesShoulder Arthroscopy Patient Education Packet Rayappaapi-549337910No ratings yet
- Lower Limb FracturesDocument124 pagesLower Limb Fracturesmau tau100% (1)
- Distal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurDocument76 pagesDistal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurToàn Đặng Phan VĩnhNo ratings yet
- Traction in OrthopaedicDocument32 pagesTraction in OrthopaedicFarry Doank100% (1)
- Spine Examination: Mario Johan Heryputra 11.2012.208Document29 pagesSpine Examination: Mario Johan Heryputra 11.2012.208Mario Johan Heryputra100% (1)
- Week 2 Ortho Tests Figure NoDocument14 pagesWeek 2 Ortho Tests Figure Noapi-468597987100% (1)
- The Anatomy and Surgical Approach of ForearmDocument25 pagesThe Anatomy and Surgical Approach of Forearmamel015100% (1)
- C SpineDocument33 pagesC SpineKarthickNo ratings yet
- Low Back PainDocument8 pagesLow Back PainLev KalikaNo ratings yet
- Ankle Fractures - A Logical Approach To Their FixationDocument48 pagesAnkle Fractures - A Logical Approach To Their FixationRoman MosneagaNo ratings yet
- Wrist Drop Claw Hand Median Nerve Palsy: Dr. Srivatsa.NDocument46 pagesWrist Drop Claw Hand Median Nerve Palsy: Dr. Srivatsa.NMurali KarthikkNo ratings yet
- Peripheral Nerve Injuries: Nerve Connective Tissue Nervous SystemDocument70 pagesPeripheral Nerve Injuries: Nerve Connective Tissue Nervous SystemRupika SodhiNo ratings yet
- Dr. Ankit Gujarathi DMH PuneDocument32 pagesDr. Ankit Gujarathi DMH PuneAnkit GujarathiNo ratings yet
- Electrotherapy: Clinical CasesDocument18 pagesElectrotherapy: Clinical CasesjothiNo ratings yet
- Presented By: DR - Shilpa K PrajapatiDocument46 pagesPresented By: DR - Shilpa K PrajapatijothiNo ratings yet
- Bedside Clinics IVDocument10 pagesBedside Clinics IVjothi100% (2)
- 2-Lab Activities - Electrotherapy Application ProceduresDocument13 pages2-Lab Activities - Electrotherapy Application ProceduresjothiNo ratings yet
- Medium Frequency: Interferential TherapyDocument31 pagesMedium Frequency: Interferential TherapyjothiNo ratings yet
- DR - Sanyal Kumar JR Dept of PMRDocument25 pagesDR - Sanyal Kumar JR Dept of PMRjothiNo ratings yet
- Assistive Technology Presentation Braille 1226057512134632 8Document12 pagesAssistive Technology Presentation Braille 1226057512134632 8jothiNo ratings yet
- Evaluating Core Stability: Reliability and Validity of Hand-Held Dynamometry in Measuring Core StrengthDocument50 pagesEvaluating Core Stability: Reliability and Validity of Hand-Held Dynamometry in Measuring Core StrengthjothiNo ratings yet
- Peripheral Nerve Injuries: DR - Prateek Singh Intern Dept. of Orthopaedics BpkihsDocument29 pagesPeripheral Nerve Injuries: DR - Prateek Singh Intern Dept. of Orthopaedics BpkihsjothiNo ratings yet
- Pre and Post Operative Physiotherapy Management in Tendon Transfer of HandDocument59 pagesPre and Post Operative Physiotherapy Management in Tendon Transfer of HandjothiNo ratings yet
- Journal of BiomechanicsDocument11 pagesJournal of BiomechanicsjothiNo ratings yet
- Journal of BiomechanicsDocument10 pagesJournal of BiomechanicsjothiNo ratings yet
- Physeal Injuries: Dr. Bassey, A E Orthopaedic & Trauma Surgery U.A.T.H, AbujaDocument30 pagesPhyseal Injuries: Dr. Bassey, A E Orthopaedic & Trauma Surgery U.A.T.H, AbujajothiNo ratings yet
- Therapeutic Exercise NotesDocument288 pagesTherapeutic Exercise NotesMarysav100% (1)
- Qdoc - Tips - Muscles of The Upper Limb Made EasyDocument7 pagesQdoc - Tips - Muscles of The Upper Limb Made EasyAkomolede AbosedeNo ratings yet
- Osteology BonesDocument48 pagesOsteology BonesÂhmęd ĐoolaNo ratings yet
- 13-Hand & WristDocument10 pages13-Hand & Wristzain juttNo ratings yet
- 2k19 Anatomy CA 1Document10 pages2k19 Anatomy CA 1Tofunmi AdegokeNo ratings yet
- Kewenangan Klinis Dr. Ayiq, Sp. OTDocument12 pagesKewenangan Klinis Dr. Ayiq, Sp. OTGestiNo ratings yet
- Female Muscle DiagramDocument1 pageFemale Muscle DiagrammakukikiNo ratings yet
- Module 6 - Muscular System Part 4 StudentDocument41 pagesModule 6 - Muscular System Part 4 StudentLaw HacksNo ratings yet
- Anatomy (Stockoe) For Mini NotesDocument86 pagesAnatomy (Stockoe) For Mini NotesIvy Dianne PascualNo ratings yet
- Some Good MnemonicsDocument6 pagesSome Good MnemonicsMehdi BaigNo ratings yet
- Diseases of The Horse's Foot by Reeks, Harry CaultonDocument282 pagesDiseases of The Horse's Foot by Reeks, Harry CaultonGutenberg.org100% (1)
- Locomotor - Hand Clinical Mark SheetDocument7 pagesLocomotor - Hand Clinical Mark SheetDrShamshad KhanNo ratings yet
- 27 Feature Extraction and Classifier in The Development of Exoskeleton Based On Emg Signal Control A ReviewDocument7 pages27 Feature Extraction and Classifier in The Development of Exoskeleton Based On Emg Signal Control A ReviewTriwiyanto TriwiyantoNo ratings yet
- Single Choice Questions in ORTHOPAEDICS Mahmood A Sulaiman: January 2019Document186 pagesSingle Choice Questions in ORTHOPAEDICS Mahmood A Sulaiman: January 2019Kiran Kumar100% (1)
- Tendon TransfersDocument194 pagesTendon Transferschinthaka_wijedasa100% (4)
- Decoding Arm Movements by Myoeletric Signals and Artificial Neural NetworksDocument6 pagesDecoding Arm Movements by Myoeletric Signals and Artificial Neural NetworksAnurag SharmaNo ratings yet
- Anatomia de PiermatteiDocument5 pagesAnatomia de PiermatteiFernando Melo GarciaNo ratings yet
- Donald A. Neumann - Kinesiology of The Musculoskeletal System 3rd Edition (2018, ELSEVIER) - Libgen - Li-P Íginas-9Document40 pagesDonald A. Neumann - Kinesiology of The Musculoskeletal System 3rd Edition (2018, ELSEVIER) - Libgen - Li-P Íginas-9ritaalmeida98No ratings yet
- 4 - Surgical Approaches To The Elbow 2012 Orthopaedics and TraumaDocument6 pages4 - Surgical Approaches To The Elbow 2012 Orthopaedics and TraumaProfesseur Christian DumontierNo ratings yet
- 1 Anatomy-MSKDocument86 pages1 Anatomy-MSKashim tiwariNo ratings yet
- TARO 2018 Corrigido e Com Referencias Final 1Document31 pagesTARO 2018 Corrigido e Com Referencias Final 1Isabella de OliveiraNo ratings yet
- Atlas of Orthopedic Surgical Procedures of The Dog and CatDocument244 pagesAtlas of Orthopedic Surgical Procedures of The Dog and Catשאול רייס100% (4)
- BooksDocument388 pagesBooksMayank GoyalNo ratings yet
- Exam Table For Hand Wrist ForearmDocument22 pagesExam Table For Hand Wrist ForearmLouie OkayNo ratings yet
- Buku-Anatomi Osteologi PDFDocument56 pagesBuku-Anatomi Osteologi PDFmuhammad firdausNo ratings yet
- Dr. Paredes: Upper Extremity of MSKDocument18 pagesDr. Paredes: Upper Extremity of MSKJose Emmanuel DolorNo ratings yet
- Osteology I: Bones of The Upper LimbDocument26 pagesOsteology I: Bones of The Upper LimbNaufalNo ratings yet
- Chapter 18Document182 pagesChapter 18ryllerylle05No ratings yet