Download as docx, pdf, or txt
You might also like
- PALS Systematic Approach Summary: Initial ImpressionDocument2 pagesPALS Systematic Approach Summary: Initial ImpressionMark Vergel II100% (3)
- Acccn Paed Interactive Manual 2018Document108 pagesAcccn Paed Interactive Manual 2018Seb KirbyNo ratings yet
- ALS Manual PDFDocument74 pagesALS Manual PDFBlack Owell100% (1)
- Care of Tracheostomy ProcedureDocument5 pagesCare of Tracheostomy ProcedureRuchika Kaushal100% (5)
- Tracheostomy CareDocument10 pagesTracheostomy CareSharifa Al AmerNo ratings yet
- Suctioning 160714115618Document18 pagesSuctioning 160714115618jothi100% (2)
- ABCDE Approach To The Critically Ill Patient - Nick SmithDocument40 pagesABCDE Approach To The Critically Ill Patient - Nick SmithBadrul Hisyam Alias100% (1)
- Rennel Jehan B. Egbalic Bsn-Iv: 1. Airway ObstructionDocument15 pagesRennel Jehan B. Egbalic Bsn-Iv: 1. Airway ObstructionDinarkram Rabreca EculNo ratings yet
- St. Paul University Dumaguete College of Nursing A.Y. 1st SEMESTER 2020-2021Document17 pagesSt. Paul University Dumaguete College of Nursing A.Y. 1st SEMESTER 2020-2021Mary Rose Silva GargarNo ratings yet
- NSTP Basic First Aid DownloadsDocument13 pagesNSTP Basic First Aid DownloadsJohnjohn MateoNo ratings yet
- First Aid and Emergency Medical ServicesDocument17 pagesFirst Aid and Emergency Medical ServicesChristia Isabelle TorresSantos SytamcoNo ratings yet
- Sutureworkshop Handout PDFDocument8 pagesSutureworkshop Handout PDFViharaDewiMahendraNo ratings yet
- Tgs Chelsa Individu Mr. BingsDocument4 pagesTgs Chelsa Individu Mr. Bingsjeffriwahyudi91No ratings yet
- AdordionisioRM ASS1Document5 pagesAdordionisioRM ASS1Forky DorkyNo ratings yet
- SuctioningDocument31 pagesSuctioningmelanie silvaNo ratings yet
- Medical and Surgical AsepsisDocument5 pagesMedical and Surgical AsepsisRae Marie AquinoNo ratings yet
- First Aid ManualDocument32 pagesFirst Aid Manualreachpunnya5538No ratings yet
- Suctioning ProceduresDocument10 pagesSuctioning ProceduresShiangNo ratings yet
- Hypertonic SolutionsDocument4 pagesHypertonic SolutionsVanessa PaguiriganNo ratings yet
- Tracheostomy Care: Thanuja Eleena MathewDocument20 pagesTracheostomy Care: Thanuja Eleena MathewOng Karl100% (3)
- Cleaning The WoundDocument10 pagesCleaning The WoundFelix ZabanalNo ratings yet
- Oral and Nasal SuctioningDocument6 pagesOral and Nasal SuctioningaafrinNo ratings yet
- First Aid in Electronic IndustryDocument6 pagesFirst Aid in Electronic IndustryRan BaltazarNo ratings yet
- Injection & Infusion: Chirathawornkhun, Parinda Meimban, Giuzeppe Edrel VeniegasDocument42 pagesInjection & Infusion: Chirathawornkhun, Parinda Meimban, Giuzeppe Edrel VeniegasNdor Baribolo100% (4)
- Practical Procedures: Seldinger Intercostal Drain InsertionDocument3 pagesPractical Procedures: Seldinger Intercostal Drain InsertionppgpcsNo ratings yet
- ET TubeDocument4 pagesET TuberumasadraunaNo ratings yet
- Apply Basic Aid-Common First Aid Emergencies and TreatmentsDocument35 pagesApply Basic Aid-Common First Aid Emergencies and Treatmentsjessicaminaj2024No ratings yet
- Et CareDocument15 pagesEt CarePaulo GarciaNo ratings yet
- First Aid: Wounds Sprain FractureDocument104 pagesFirst Aid: Wounds Sprain FractureKaye CorNo ratings yet
- Peer Assessment Insertion ICDDocument2 pagesPeer Assessment Insertion ICDRichardNo ratings yet
- C CC CCCC CCC CCC CCCCCCC CDocument5 pagesC CC CCCC CCC CCC CCCCCCC CRosalie Valdez EspirituNo ratings yet
- SuctioningDocument6 pagesSuctioningCriselda Ultado100% (2)
- Dressing and Bandaging in First Aid: Wound Healing BandageDocument8 pagesDressing and Bandaging in First Aid: Wound Healing BandageRosalouise P. UngabNo ratings yet
- Tracheostomy CareDocument17 pagesTracheostomy Caresam100% (2)
- Record Mo ToDocument5 pagesRecord Mo ToAce WoodsNo ratings yet
- Nasogastric Tube InsertionDocument8 pagesNasogastric Tube InsertionPaulo ManitiNo ratings yet
- Intercostal Chest DrainageDocument6 pagesIntercostal Chest DrainageNovalis CrazyNo ratings yet
- Surgical AsepsisDocument29 pagesSurgical AsepsisRyan Llanto100% (1)
- Presentation DEEPTHIDocument17 pagesPresentation DEEPTHIsarathchandran deepthiNo ratings yet
- First Aid Basic Course: Disaster Management Cell Shantikunj, Haridwar (Uttrakhand)Document47 pagesFirst Aid Basic Course: Disaster Management Cell Shantikunj, Haridwar (Uttrakhand)Yogesh Kumar DewanganNo ratings yet
- Emergency Care: Eletric ShockDocument9 pagesEmergency Care: Eletric ShockSyahidd Al-HatimNo ratings yet
- First Aid: FIRST AID: Immediate and Temporary Treatment Administered To An Injured or Sick PersonDocument4 pagesFirst Aid: FIRST AID: Immediate and Temporary Treatment Administered To An Injured or Sick PersonPaul NallaNo ratings yet
- First Aid EngDocument5 pagesFirst Aid EngRavikant PandeyNo ratings yet
- Tracheostomy Care: When Is A Tracheostomy Considered?Document7 pagesTracheostomy Care: When Is A Tracheostomy Considered?issaiahnicolleNo ratings yet
- Tracheostomy CareDocument31 pagesTracheostomy CareUday KumarNo ratings yet
- Incision & Drainage of Abscess Group 9 4bDocument5 pagesIncision & Drainage of Abscess Group 9 4bGUDISELA ramyaNo ratings yet
- Intravenous, Subcutan and Intracutan Injection: Dr. A.A.A. Lila Paramasatiari, M.Biomed Fkik Universitas WarmadewaDocument45 pagesIntravenous, Subcutan and Intracutan Injection: Dr. A.A.A. Lila Paramasatiari, M.Biomed Fkik Universitas Warmadewayogi pramanaNo ratings yet
- FIRST AID of Common Resort Injuries: by DR NaazDocument37 pagesFIRST AID of Common Resort Injuries: by DR NaazdnaaziiNo ratings yet
- Summary OsceDocument5 pagesSummary OsceAshley IshikaNo ratings yet
- Dressing and Bandaging WoundsDocument28 pagesDressing and Bandaging WoundsGemma Mondero ColladoNo ratings yet
- Wound Care: Preventing Infection: Download PDFDocument4 pagesWound Care: Preventing Infection: Download PDFzulaikha zulkepliNo ratings yet
- SuctioningDocument30 pagesSuctioningbajaoc60% (5)
- CTT CareDocument76 pagesCTT CareMarites Santos AquinoNo ratings yet
- Poison, Nosebleeds, Sucking Chest Wound, Abdominal EvisceratioDocument46 pagesPoison, Nosebleeds, Sucking Chest Wound, Abdominal EvisceratioYumeko JabamiNo ratings yet
- Cannula-Insertion NewDocument6 pagesCannula-Insertion Newلوريس أبو الفتوحNo ratings yet
- HemorrhageDocument15 pagesHemorrhageMariegreat Piscos BisnarNo ratings yet
- Starting An Intravenous InfusionDocument20 pagesStarting An Intravenous InfusionDoj Deej Mendoza Gamble100% (1)
- Airway ManagementDocument16 pagesAirway ManagementSuganthi ParthibanNo ratings yet
- Procedure Checklist For Suctioning NCM 112 SL Done Not DoneDocument4 pagesProcedure Checklist For Suctioning NCM 112 SL Done Not DoneIrish Eunice Felix100% (1)
- Suctioning Et SuctioningDocument7 pagesSuctioning Et SuctioningKoochi PoojithaNo ratings yet
- MedSurg RecitDocument3 pagesMedSurg RecitnicoleNo ratings yet
- PEDIATRIC FIRST AID: How to respond quickly when your child is in dangerFrom EverandPEDIATRIC FIRST AID: How to respond quickly when your child is in dangerNo ratings yet
- Survival Skills: How to Survive Anything and Anywhere in the World (A Comprehensive Guide to Preparing for and Overcoming Challenges of Earthquakes)From EverandSurvival Skills: How to Survive Anything and Anywhere in the World (A Comprehensive Guide to Preparing for and Overcoming Challenges of Earthquakes)No ratings yet
- Diphtheria how to recognize the disease, how to keep from catching it, how to treat those who do catch itFrom EverandDiphtheria how to recognize the disease, how to keep from catching it, how to treat those who do catch itNo ratings yet
- Saint Paul University Dumaguete College of Nursing A.Y. 2020 - 2021Document1 pageSaint Paul University Dumaguete College of Nursing A.Y. 2020 - 2021Dinarkram Rabreca EculNo ratings yet
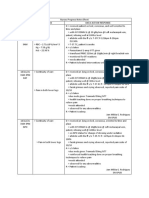
- Nurses Progress NotesDocument1 pageNurses Progress NotesDinarkram Rabreca EculNo ratings yet
- 4 Progress NotesDocument6 pages4 Progress NotesDinarkram Rabreca EculNo ratings yet
- GROUP 3 - CASE STUDY - TraumaDocument5 pagesGROUP 3 - CASE STUDY - TraumaDinarkram Rabreca EculNo ratings yet
- NCP - October 10Document10 pagesNCP - October 10Dinarkram Rabreca EculNo ratings yet
- St. Paul University Dumaguete St. Paul University System College of Nursing ISO 9001Document16 pagesSt. Paul University Dumaguete St. Paul University System College of Nursing ISO 9001Dinarkram Rabreca EculNo ratings yet
- ALOC Can Be Caused by A Head Injury, Medicines, Alcohol or Drugs, Dehydration, or Some Diseases, Such As DiabetesDocument9 pagesALOC Can Be Caused by A Head Injury, Medicines, Alcohol or Drugs, Dehydration, or Some Diseases, Such As DiabetesDinarkram Rabreca EculNo ratings yet
- NCP - October 10Document6 pagesNCP - October 10Dinarkram Rabreca EculNo ratings yet
- In Partial Fulfillment of The Requirements in NCM 102: Saint Paul University Dumaguete College of NursingDocument4 pagesIn Partial Fulfillment of The Requirements in NCM 102: Saint Paul University Dumaguete College of NursingDinarkram Rabreca EculNo ratings yet
- (RODRIGUEZ) Scenario Based ERDocument3 pages(RODRIGUEZ) Scenario Based ERDinarkram Rabreca EculNo ratings yet
- Problem Statement and A Purpose Statement Serves To Narrow The Focus of The Research Into ADocument4 pagesProblem Statement and A Purpose Statement Serves To Narrow The Focus of The Research Into ADinarkram Rabreca EculNo ratings yet
- Micu CasesDocument2 pagesMicu CasesDinarkram Rabreca EculNo ratings yet
- Age and Sex DistributionDocument4 pagesAge and Sex DistributionDinarkram Rabreca EculNo ratings yet
- Intracerebral Hemorrhage Right Sided StrokeDocument2 pagesIntracerebral Hemorrhage Right Sided StrokeDinarkram Rabreca EculNo ratings yet
- (Rodriguez) Scenario 1Document3 pages(Rodriguez) Scenario 1Dinarkram Rabreca EculNo ratings yet
- Teach The Client and Family About The Need For Hand HygieneDocument3 pagesTeach The Client and Family About The Need For Hand HygieneDinarkram Rabreca EculNo ratings yet
- Emergency OGs at HWCDocument98 pagesEmergency OGs at HWCcmvaraprasadNo ratings yet
- First Aid in Electric ShockDocument6 pagesFirst Aid in Electric ShockmacishereNo ratings yet
- Perform Basic First Aid ProceduresDocument76 pagesPerform Basic First Aid ProceduresGlenn ClementeNo ratings yet
- NCM 101 Lecture Nurses Role During Health Assessment in The Nursing PracticeDocument18 pagesNCM 101 Lecture Nurses Role During Health Assessment in The Nursing PracticeTHEA KERSTI ECOTNo ratings yet
- Activit-1-For-Trauma-Care Assessment.Document3 pagesActivit-1-For-Trauma-Care Assessment.amal abdulrahmanNo ratings yet
- Draft For FAT L1 Course AkzonobelDocument8 pagesDraft For FAT L1 Course AkzonobelHung DinhNo ratings yet
- Abcde Erp39p44Document6 pagesAbcde Erp39p44Elizabeth Toapanta VrnNo ratings yet
- ER تجميعة 2Document8 pagesER تجميعة 2lclkNo ratings yet
- NSTP 2 Midterm ReviewerDocument6 pagesNSTP 2 Midterm ReviewerTrexy NorialNo ratings yet
- RESUS 8904 Special CircsDocument68 pagesRESUS 8904 Special CircsCroBranNo ratings yet
- Module Health 9 q3 Week 7 8Document44 pagesModule Health 9 q3 Week 7 8jamaicaantonio87No ratings yet
- Health Assessment Chapter 27 EmergencyDocument24 pagesHealth Assessment Chapter 27 Emergencyaderonke123No ratings yet
- RMSS Midterm-ReviewerDocument3 pagesRMSS Midterm-ReviewerNoime AlbaoNo ratings yet
- Emergency Care Training Manual For CHO at AB-HWCDocument82 pagesEmergency Care Training Manual For CHO at AB-HWCmohammed raziNo ratings yet
- Physical Examination of The Critically Injured AthleteDocument25 pagesPhysical Examination of The Critically Injured Athletebrida.bluesNo ratings yet
- Jason Wolfe's ATLS Trauma Moulage Page: (Thoughts On The Management of The Multiply Injured Patient)Document18 pagesJason Wolfe's ATLS Trauma Moulage Page: (Thoughts On The Management of The Multiply Injured Patient)gogopal100% (6)
- Injury Identification and Recognition For Coaches: Sports MedicineDocument2 pagesInjury Identification and Recognition For Coaches: Sports MedicineKevin JordanNo ratings yet
- Clinical ToxicologyDocument36 pagesClinical ToxicologyMuhammad FawadNo ratings yet
- GetCWExternalDocument SDS Carbon RemoverDocument15 pagesGetCWExternalDocument SDS Carbon RemoverAVINASH ANAND RAONo ratings yet
- Bahan Ajar INITIAL ASSESMENT AND MANAGEMENT UMJ - PPTX Terbaru BangetDocument49 pagesBahan Ajar INITIAL ASSESMENT AND MANAGEMENT UMJ - PPTX Terbaru Bangetteuku rizqonNo ratings yet
- Dementia and Prehospital ImplicationsDocument11 pagesDementia and Prehospital ImplicationsIlyes FerenczNo ratings yet
- European Resuscitation Council Algorithm PostersDocument9 pagesEuropean Resuscitation Council Algorithm Postersmisohorne100% (2)
- International JournalDocument5 pagesInternational JournalPutri Nur HandayaniNo ratings yet
- Acol FirstaidDocument4 pagesAcol FirstaidkieNo ratings yet
- SLIPPS SimDocument17 pagesSLIPPS SimFrancis Jay EnriquezNo ratings yet
- First Aid KitDocument15 pagesFirst Aid KitRuthNo ratings yet