Download as pdf or txt
You might also like
- FULL Download Ebook PDF Huszars Ecg and 12 Lead Interpretation 5th Edition PDF EbookDocument41 pagesFULL Download Ebook PDF Huszars Ecg and 12 Lead Interpretation 5th Edition PDF Ebookcody.cherry20098% (40)
- BLS Pretest All Questions AnswersDocument7 pagesBLS Pretest All Questions AnswersFatMania63% (24)
- Case Studies in Clinical Cardiac Electrophysiology (PDFDrive)Document432 pagesCase Studies in Clinical Cardiac Electrophysiology (PDFDrive)aafagih100% (1)
- MSN Project Template Su21Document47 pagesMSN Project Template Su21api-577186606No ratings yet
- Kessler 2005Document11 pagesKessler 2005mccg1478No ratings yet
- Dubin ECG Reference SheetsDocument13 pagesDubin ECG Reference SheetsEllie100% (1)
- Mortality in The United States, 2013 Db178Document8 pagesMortality in The United States, 2013 Db178Smith MikeNo ratings yet
- 58820-66 SlidesDocument79 pages58820-66 SlidesEusebius01No ratings yet
- Racial and Ethnic Health Disparities in Miami-DadeDocument56 pagesRacial and Ethnic Health Disparities in Miami-DadeCynthia EvansNo ratings yet
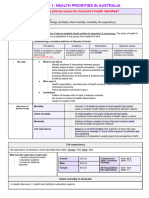
- Core-1 - PDHPE Health Priorities in AustraliaDocument13 pagesCore-1 - PDHPE Health Priorities in Australiaamberwallis999No ratings yet
- Health and Food and Nutrition Consumption ErasmusDocument52 pagesHealth and Food and Nutrition Consumption ErasmusNur AzizahNo ratings yet
- HPV Lay LectureDocument32 pagesHPV Lay LectureGene LynNo ratings yet
- South Carolina Maternal Morbidity and Mortality Review CommitteeDocument4 pagesSouth Carolina Maternal Morbidity and Mortality Review CommitteeABC15 NewsNo ratings yet
- HSC PDHPE - Core OneDocument7 pagesHSC PDHPE - Core Onenatecant15No ratings yet
- Hi PDFDocument74 pagesHi PDFNur HazimahNo ratings yet
- Pharmacy: Prescribing Patterns of Antihypertensive Medications in US Ambulatory Care SettingsDocument7 pagesPharmacy: Prescribing Patterns of Antihypertensive Medications in US Ambulatory Care SettingsSandhya kumarNo ratings yet
- Thesis FinalDocument46 pagesThesis FinalenasNo ratings yet
- 2021aug Hiv Sti 101 2018 Stats v1Document66 pages2021aug Hiv Sti 101 2018 Stats v1Narendra GowdaNo ratings yet
- Pdhpe Notes FullDocument79 pagesPdhpe Notes FullFarhad HakimiNo ratings yet
- Overview of Generalized Anxiety DisorderDocument6 pagesOverview of Generalized Anxiety Disordernandaas887No ratings yet
- Epidemiology - Class 1 & 2Document28 pagesEpidemiology - Class 1 & 2drshivangishomoeopathyNo ratings yet
- Global Perspectives On Mental HealthDocument21 pagesGlobal Perspectives On Mental Health4127297No ratings yet
- Mortality and MorbilityDocument26 pagesMortality and MorbilityR.vijay100% (3)
- Bma Covid 19 Risk Assessment Tool February 2021Document2 pagesBma Covid 19 Risk Assessment Tool February 2021GinoFTNo ratings yet
- 2-Zaatari Health Information System - Profile Report Quarter 3 2023Document2 pages2-Zaatari Health Information System - Profile Report Quarter 3 2023BATOOLALAMRINo ratings yet
- Child Health Programme: 4.2.2 Causes of Child Mortality in IndiaDocument24 pagesChild Health Programme: 4.2.2 Causes of Child Mortality in IndiaSolomon JosephNo ratings yet
- Risk Factor For DementiaDocument11 pagesRisk Factor For DementiaBambang SutrisnoNo ratings yet
- 2020 Infant Mortality Annual ReportDocument56 pages2020 Infant Mortality Annual ReportTitus WuNo ratings yet
- MentalHealth-profile-2020 Trinidad&Tobago Country Report FinalDocument2 pagesMentalHealth-profile-2020 Trinidad&Tobago Country Report FinalG BhagiratheeNo ratings yet
- Marital Status and 5-Year Mortality: A Population-Based Prospective Cohort StudyDocument4 pagesMarital Status and 5-Year Mortality: A Population-Based Prospective Cohort StudyEstefania AriasNo ratings yet
- Health Indicators: Global and National PerspectiveDocument20 pagesHealth Indicators: Global and National PerspectiveZainabNo ratings yet
- Global Chronic DisDocument6 pagesGlobal Chronic Disujangketul62No ratings yet
- Module 7 - Pharmacotherapy For Endocrine and Exocrine DisordersDocument306 pagesModule 7 - Pharmacotherapy For Endocrine and Exocrine Disordersgeekay79No ratings yet
- Alleviating The Access Abyss in Palliative Care and Pain Relief.Document37 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief.Presentaciones_FKNo ratings yet
- LUNDBERG Et Al-1997-Journal of Internal MedicineDocument8 pagesLUNDBERG Et Al-1997-Journal of Internal MedicineamanNo ratings yet
- Alzheimer's Disease: 2017 Facts and FiguresDocument88 pagesAlzheimer's Disease: 2017 Facts and FiguresGina SmithNo ratings yet
- Fazel 2014 CORRECTE PDFDocument11 pagesFazel 2014 CORRECTE PDFMargaNo ratings yet
- The Depression ReportDocument20 pagesThe Depression Reportprincesscat1No ratings yet
- Xu 2018Document7 pagesXu 2018ZUNENo ratings yet
- Screening For Cardiovascular Disease and Risk Factors (Patient Version) - Mar 2011Document12 pagesScreening For Cardiovascular Disease and Risk Factors (Patient Version) - Mar 2011ahmad gunturNo ratings yet
- Prevalence of Eating Disorders Over The 2000-2018 PeriodDocument12 pagesPrevalence of Eating Disorders Over The 2000-2018 PeriodloloasbNo ratings yet
- Bipolar MedicationDocument5 pagesBipolar MedicationindarNo ratings yet
- Lecture 4Document32 pagesLecture 4Rahul RawatNo ratings yet
- Suicide PreventionDocument34 pagesSuicide PreventionanirudhNo ratings yet
- Sas 1 60 Multiple Choice Converted CompressedDocument153 pagesSas 1 60 Multiple Choice Converted CompressedRoswell Almodiel EscaranNo ratings yet
- Global Burden of DiseaseDocument41 pagesGlobal Burden of DiseaseshailaNo ratings yet
- Biogen at JPM 2022 WebcastDocument30 pagesBiogen at JPM 2022 WebcastJoseph Adinolfi Jr.No ratings yet
- Cost Benefit by Age Analysis The COVID VACCINES KILL MOREPEOPLEDocument14 pagesCost Benefit by Age Analysis The COVID VACCINES KILL MOREPEOPLETUTO TUTONo ratings yet
- Federal Efforts To Research Alzheimer's and DementiaDocument57 pagesFederal Efforts To Research Alzheimer's and DementiaNational Press FoundationNo ratings yet
- SlidesDocument48 pagesSlidesMarrkNo ratings yet
- Global Burden of DiseaseDocument42 pagesGlobal Burden of Diseasesantoshipoudel08No ratings yet
- Demencia EvaluacionDocument8 pagesDemencia EvaluacionMatias Felipe Contreras EspinozaNo ratings yet
- Presentation and Character For Adult Patients With Diabetes in LibyaDocument8 pagesPresentation and Character For Adult Patients With Diabetes in LibyaMediterr J Pharm Pharm SciNo ratings yet
- TP 5Document3 pagesTP 5Rebeca FrancoNo ratings yet
- hh9 lt1 006Document1 pagehh9 lt1 006marthavalenciaNo ratings yet
- PERSPEKTIF KEPERAWATAN ANAK - IndonesiaDocument13 pagesPERSPEKTIF KEPERAWATAN ANAK - IndonesiaAgus MardiansyahNo ratings yet
- Nej MC 2009787Document3 pagesNej MC 2009787Nini KvantalianiNo ratings yet
- DohDocument103 pagesDohRapSamputonNo ratings yet
- 1 - NCD in MalaysiaDocument17 pages1 - NCD in Malaysiaedkktm pkdmNo ratings yet
- PP Eka Konika HematoDocument15 pagesPP Eka Konika HematopermatamoNo ratings yet
- Facts About Suicide and DepressionDocument5 pagesFacts About Suicide and DepressionAmy PollardNo ratings yet
- Diabetes in The UK 2010Document21 pagesDiabetes in The UK 2010jrjsdNo ratings yet
- In Excellent Health: Setting the Record Straight on America's Health CareFrom EverandIn Excellent Health: Setting the Record Straight on America's Health CareRating: 5 out of 5 stars5/5 (3)
- Allergy Prevention in Children: The Role of Partially Hydrolyzed FormulaDocument35 pagesAllergy Prevention in Children: The Role of Partially Hydrolyzed FormulawidyadariNo ratings yet
- Fassbender 2020Document10 pagesFassbender 2020widyadariNo ratings yet
- Advanced Prehospital Stroke Care: Mobile Stroke Treatment UnitDocument3 pagesAdvanced Prehospital Stroke Care: Mobile Stroke Treatment UnitwidyadariNo ratings yet
- Reference SystemDocument26 pagesReference SystemwidyadariNo ratings yet
- s2 Keperawatan 2016 Penanganan Bencana (Bag.1)Document84 pagess2 Keperawatan 2016 Penanganan Bencana (Bag.1)widyadariNo ratings yet
- Dessens, F.M Et Al. 2020Document8 pagesDessens, F.M Et Al. 2020widyadariNo ratings yet
- Imaging, Intervention, and Work Ow in Acute Ischemic Stroke: The Calgary ApproachDocument7 pagesImaging, Intervention, and Work Ow in Acute Ischemic Stroke: The Calgary ApproachwidyadariNo ratings yet
- Assis 2017Document19 pagesAssis 2017widyadariNo ratings yet
- Journal Pre-Proof: Nurse Education in PracticeDocument25 pagesJournal Pre-Proof: Nurse Education in PracticewidyadariNo ratings yet
- Venema E, Et Al. 2018Document6 pagesVenema E, Et Al. 2018widyadariNo ratings yet
- Adult Emergency Nurse Protocol HEAD INJURY (Closed)Document3 pagesAdult Emergency Nurse Protocol HEAD INJURY (Closed)widyadariNo ratings yet
- Fitriani, Et AlDocument14 pagesFitriani, Et AlwidyadariNo ratings yet
- Shane P. Prejean, MD, Munaib Din, BSC, Eliana Reyes, MD, PHD, and Fadi G. Hage, MD, FasncDocument8 pagesShane P. Prejean, MD, Munaib Din, BSC, Eliana Reyes, MD, PHD, and Fadi G. Hage, MD, FasncwidyadariNo ratings yet
- Pengaruh Kompres Aloe Vera THDP Flebitis Pemasangan InfusDocument8 pagesPengaruh Kompres Aloe Vera THDP Flebitis Pemasangan InfuswidyadariNo ratings yet
- Science: Respiratory and Circulatory SystemsDocument31 pagesScience: Respiratory and Circulatory SystemsEjelmae Olaivar TutorNo ratings yet
- Pugazhendhi Vijayaraman Cardiac Conduction SystemDocument30 pagesPugazhendhi Vijayaraman Cardiac Conduction SystemMariaVirginiaNo ratings yet
- Severe Residual Pulmonary Stenosis After Surgical Repair of Tetralogy of Fallot: What's Our Next Strategy?Document11 pagesSevere Residual Pulmonary Stenosis After Surgical Repair of Tetralogy of Fallot: What's Our Next Strategy?International Journal of Innovative Science and Research TechnologyNo ratings yet
- Coronary Artery DiseaseDocument6 pagesCoronary Artery DiseaseDivya PriyaNo ratings yet
- اسنان باطنة Clinical FinalDocument40 pagesاسنان باطنة Clinical FinalShady AnwarNo ratings yet
- Electrocardiogram (ECG or EKG) : What Is An Electrocardiogram?Document2 pagesElectrocardiogram (ECG or EKG) : What Is An Electrocardiogram?عـَــٻاس مَـــشتاق عـَــليNo ratings yet
- Pda 1678358689Document14 pagesPda 1678358689Divyanshi KomalNo ratings yet
- Turquoise Heart Vector Medical Brochure PDFDocument2 pagesTurquoise Heart Vector Medical Brochure PDFAlex CastellanosNo ratings yet
- Unclear Outcomes of Heart Rate Variability Following A Concussion: A Systematic ReviewDocument15 pagesUnclear Outcomes of Heart Rate Variability Following A Concussion: A Systematic ReviewMahdi HosseiniNo ratings yet
- Comparison of The Efficacy of Rosuvastatin Versus Atorvastatin, Simvastatin, and Pravastatin in Achieving Lipid Goals: Results From The STELLAR TrialDocument11 pagesComparison of The Efficacy of Rosuvastatin Versus Atorvastatin, Simvastatin, and Pravastatin in Achieving Lipid Goals: Results From The STELLAR Trialamit khanNo ratings yet
- Care of Clients With Cardiovascular DisordersDocument67 pagesCare of Clients With Cardiovascular DisordersMatt Lao DionelaNo ratings yet
- Cardiopulmonary ResuscitationDocument82 pagesCardiopulmonary ResuscitationPraveen RadhakrishnanNo ratings yet
- Daftar PustakaDocument6 pagesDaftar PustakaDewy VerenNo ratings yet
- ELSO Interim Guidelines For Venoarterial.2Document18 pagesELSO Interim Guidelines For Venoarterial.2BiancaPancuNo ratings yet
- Lecture 20-21 Electrical Safety: PBS&D - Fall 2004 - PolikarDocument40 pagesLecture 20-21 Electrical Safety: PBS&D - Fall 2004 - PolikarQuantiks WertisNo ratings yet
- Practical Notes On Internal Medicine (TZTM)Document255 pagesPractical Notes On Internal Medicine (TZTM)Aung Zaya KyawNo ratings yet
- 5 Step EKG InterpretationDocument1 page5 Step EKG InterpretationSibel ErtuğrulNo ratings yet
- Brochure Xario 200GDocument12 pagesBrochure Xario 200GDuy LêNo ratings yet
- Arterial CatheterizationDocument5 pagesArterial CatheterizationSREEDEVI T SURESHNo ratings yet
- CE ImDocument72 pagesCE ImMisael LariosNo ratings yet
- Chapter 9 - Adrenergic AgonistsDocument4 pagesChapter 9 - Adrenergic AgonistsJoseph Campos SanchezNo ratings yet
- Delivered.: ConfidenceDocument7 pagesDelivered.: ConfidenceMed AkrimNo ratings yet
- Mitral Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Resident (Internal Medicine) (P-A) Chattogram Medical CollegeDocument16 pagesMitral Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Resident (Internal Medicine) (P-A) Chattogram Medical CollegeAsrafur RahmanNo ratings yet
- Sunday Academic Meet-15Document8 pagesSunday Academic Meet-15Srinivas PingaliNo ratings yet
- Jadwal Sympo Edit1Document3 pagesJadwal Sympo Edit1reyNo ratings yet
- Manual Cardiovascular SystemDocument5 pagesManual Cardiovascular SystemVynz Morales CosepNo ratings yet