Download as docx, pdf, or txt
You might also like
- Amniotic Fluid EmbolismDocument10 pagesAmniotic Fluid EmbolismRebecca ApeladoNo ratings yet
- Aguinaldo Elementary School A: Ction Plan On Provision of Psychological Support To Learners and School PersonnelDocument1 pageAguinaldo Elementary School A: Ction Plan On Provision of Psychological Support To Learners and School PersonnelRheanne Aurielle JansenNo ratings yet
- Bob Beck Protocol - Natural Cancer Treatments at CancerTutorDocument4 pagesBob Beck Protocol - Natural Cancer Treatments at CancerTutorThiago NunesNo ratings yet
- Surgical Management For Lung CancerDocument45 pagesSurgical Management For Lung CancerarifgteguhNo ratings yet
- Measles and Scarlet Fever Kawasaki Disease: Fatin & EileenDocument30 pagesMeasles and Scarlet Fever Kawasaki Disease: Fatin & EileenbyteNo ratings yet
- Tca 5Document8 pagesTca 5api-3822433No ratings yet
- MCN Lect Hypertensive Disorders in PregnancyDocument4 pagesMCN Lect Hypertensive Disorders in PregnancyAmethystNo ratings yet
- High Risk NewbornDocument4 pagesHigh Risk NewbornWenn Joyrenz ManeclangNo ratings yet
- Amniotic Fluid and Placenta AbnormalitiesDocument60 pagesAmniotic Fluid and Placenta AbnormalitiesMicah Lou CalambaNo ratings yet
- HEMAREPORT1Document6 pagesHEMAREPORT1Sarah Grace KamlaniNo ratings yet
- Introduction To ObstetricsDocument13 pagesIntroduction To ObstetricsRosselle PabloNo ratings yet
- Early Diagnosis of MalignancyDocument29 pagesEarly Diagnosis of Malignancyokwadha simionNo ratings yet
- EndometriosisDocument8 pagesEndometriosisMuhammadR1No ratings yet
- Neonatal-Child DseDocument37 pagesNeonatal-Child Dselaude.francesNo ratings yet
- RespiratoryDocument12 pagesRespiratorySmileNo ratings yet
- Biosynthesis and Physiologic Effects of Estrogen and Pathophysiologic Effects of Estrogen Deficiency: A ReviewDocument4 pagesBiosynthesis and Physiologic Effects of Estrogen and Pathophysiologic Effects of Estrogen Deficiency: A Reviewsurya antoNo ratings yet
- Drug Study Format 1Document3 pagesDrug Study Format 1Janeenne Fe Nicole SilvanoNo ratings yet
- Hydro Cep Hal UsDocument35 pagesHydro Cep Hal UsJanderlie AspaNo ratings yet
- Amniotic Fluid and Placenta AbnormalitiesDocument60 pagesAmniotic Fluid and Placenta AbnormalitiesMonique BorresNo ratings yet
- Pink OctoberDocument5 pagesPink OctoberlaylasantosleaoNo ratings yet
- Sweating in Advanced Cancer (R. Twycross)Document11 pagesSweating in Advanced Cancer (R. Twycross)docbinNo ratings yet
- Post Partum InfectionsDocument39 pagesPost Partum InfectionsAngela Kim T. DaragNo ratings yet
- OB Gyne ReviewerDocument52 pagesOB Gyne ReviewerRaffy Lucmans100% (1)
- NCM 109 Midterms - Infertility L2Document7 pagesNCM 109 Midterms - Infertility L2Leigh Angelika Dela CruzNo ratings yet
- A Miasmatic Approach To Endometriosis-1Document34 pagesA Miasmatic Approach To Endometriosis-1Suriya OsmanNo ratings yet
- Unit 5: Disease and Protection Against Disease: Nur Afiqah SallehDocument14 pagesUnit 5: Disease and Protection Against Disease: Nur Afiqah SallehAhmad albabNo ratings yet
- Polycystic OvariesDocument19 pagesPolycystic OvariesSanjeev Harry BudhooramNo ratings yet
- Case Study Drug AnaDocument7 pagesCase Study Drug AnaMagdaraog Gabrielle A.No ratings yet
- DiseasesDocument150 pagesDiseasessandip nagareNo ratings yet
- ToxoplasmosisDocument28 pagesToxoplasmosisFeby HidasariNo ratings yet
- DRUG-STUDY - BALLON, Karlo CDocument6 pagesDRUG-STUDY - BALLON, Karlo CMelinda Cariño BallonNo ratings yet
- GB Syndrome..Document13 pagesGB Syndrome..Shitaljit Irom100% (1)
- Obstetrics Prenatal Diagnosis Fetal Therapy and UltrasoundDocument14 pagesObstetrics Prenatal Diagnosis Fetal Therapy and UltrasoundRodrerick De lafuentesNo ratings yet
- Female Genital TractDocument5 pagesFemale Genital TractSagiNo ratings yet
- Emergency Managment of EclampsiaDocument38 pagesEmergency Managment of EclampsiaMemento MagicNo ratings yet
- Generic NameDocument3 pagesGeneric NameSittie Nashieva A. UsmanNo ratings yet
- TCA7 CLassnotesDocument6 pagesTCA7 CLassnotesapi-3822433No ratings yet
- POLYHYDRAMNIOSDocument2 pagesPOLYHYDRAMNIOSyxly imperialNo ratings yet
- Secondary AmenorrheaDocument3 pagesSecondary AmenorrheageldeveraNo ratings yet
- Drug Study OxytocinDocument3 pagesDrug Study OxytocinSheena Marie M. TarleNo ratings yet
- Pharmacology NotesDocument15 pagesPharmacology NotesSjerwin Anthony GiananNo ratings yet
- Amenorrhea - DrPrekshyaDocument44 pagesAmenorrhea - DrPrekshyaasdfNo ratings yet
- MCP Pedia Prelim - EndtermDocument19 pagesMCP Pedia Prelim - EndtermKM PanganibanNo ratings yet
- Ob2 Sas 13Document8 pagesOb2 Sas 13Ralph Louie ManagoNo ratings yet
- Menopause Dan KlimakteriumDocument20 pagesMenopause Dan KlimakteriumAlfix AnugrahNo ratings yet
- BrochureDocument2 pagesBrochuredverraNo ratings yet
- Gynaecology and Obstetrics PDFDocument50 pagesGynaecology and Obstetrics PDFabdulmoiz92No ratings yet
- Care of Couples With Infertility ProblemsDocument3 pagesCare of Couples With Infertility ProblemsLORNA ARTUGUENo ratings yet
- Parasitology ReviewerDocument5 pagesParasitology ReviewerMari Gayle PerezNo ratings yet
- Complications of Pregnancy: Jose, Leana Louisse D. BSN 2BDocument14 pagesComplications of Pregnancy: Jose, Leana Louisse D. BSN 2BLiana Louisse JoseNo ratings yet
- Weird SyndromsDocument13 pagesWeird SyndromsNeno TrabilsiNo ratings yet
- Asfixia Perinatal, CompendiumDocument7 pagesAsfixia Perinatal, CompendiumClaudia LópezNo ratings yet
- OBII - 16 Postterm Pregnancy - PDF Version 1Document6 pagesOBII - 16 Postterm Pregnancy - PDF Version 1Felina CabadingNo ratings yet
- #2-NCM 109 - TransesDocument19 pages#2-NCM 109 - TransesJaimie BanaagNo ratings yet
- Menopause: By: Namita Arya PDMSNCDocument58 pagesMenopause: By: Namita Arya PDMSNCnamitaNo ratings yet
- Cornell's Note 4Document5 pagesCornell's Note 4Angel BriboneriaNo ratings yet
- Obstetric Medication ProfileDocument7 pagesObstetric Medication Profilejulie.wilkNo ratings yet
- OBII - 17 Fetal Growth Disorders - PDF Version 1Document6 pagesOBII - 17 Fetal Growth Disorders - PDF Version 1Felina CabadingNo ratings yet
- AMENORRHOEADocument35 pagesAMENORRHOEAnyangaraNo ratings yet
- MalariaDocument23 pagesMalariaAryan RajNo ratings yet
- GynaecologyDocument158 pagesGynaecologySyahrul ShaaraniNo ratings yet
- Infertility 001Document257 pagesInfertility 001Habtamu Nigussie100% (1)
- Abnormal Uterine Bleeding: Understanding, Diagnosis, and TreatmentFrom EverandAbnormal Uterine Bleeding: Understanding, Diagnosis, and TreatmentNo ratings yet
- Kissing Spine SyndromeDocument4 pagesKissing Spine SyndromeMarcel Quario OrinaNo ratings yet
- Perianal Abscess Long Fish BoneDocument3 pagesPerianal Abscess Long Fish BoneMarcel Quario OrinaNo ratings yet
- Renal or Urinary Tract DisorderDocument6 pagesRenal or Urinary Tract DisorderMarcel Quario OrinaNo ratings yet
- Physical Assessment: Respiratory DisordersDocument3 pagesPhysical Assessment: Respiratory DisordersMarcel Quario OrinaNo ratings yet
- Journal ArticleDocument8 pagesJournal ArticleMarcel Quario OrinaNo ratings yet
- RS45 NE 19th Century Social Encyclicals 1Document29 pagesRS45 NE 19th Century Social Encyclicals 1Marcel Quario OrinaNo ratings yet
- Stroke KidneyDocument3 pagesStroke KidneyMarcel Quario OrinaNo ratings yet
- Burns RRLDocument5 pagesBurns RRLMarcel Quario OrinaNo ratings yet
- Paley Design ArgumentDocument15 pagesPaley Design ArgumentMarcel Quario OrinaNo ratings yet
- Hyperthyroidism: NCM 116 Lec Mrs. Ma Jesseca P. MonsantoDocument6 pagesHyperthyroidism: NCM 116 Lec Mrs. Ma Jesseca P. MonsantoMarcel Quario OrinaNo ratings yet
- Technical Writing Guidelines GuideDocument3 pagesTechnical Writing Guidelines GuideMarcel Quario OrinaNo ratings yet
- Year End 2Document4 pagesYear End 2Marcel Quario OrinaNo ratings yet
- Orina, Marcel Bachelor of Science in Nursing 2 Year Xavier University-Ateneo de Cagayan 1 SEM SY 2019-20Document3 pagesOrina, Marcel Bachelor of Science in Nursing 2 Year Xavier University-Ateneo de Cagayan 1 SEM SY 2019-20Marcel Quario OrinaNo ratings yet
- Sagabal, Angelyn Grade 8 - Brilliance Aposkahoy National High School SY 2018-19 Year-End Accomplishment Report Month Activity RemarksDocument1 pageSagabal, Angelyn Grade 8 - Brilliance Aposkahoy National High School SY 2018-19 Year-End Accomplishment Report Month Activity RemarksMarcel Quario OrinaNo ratings yet
- UEMS Rheumatology Specialist Core Curriculum 2003Document5 pagesUEMS Rheumatology Specialist Core Curriculum 2003Amer WasimNo ratings yet
- How To Overcome Perfectionism Personal Excellence EbookDocument43 pagesHow To Overcome Perfectionism Personal Excellence EbookDeepak SinghNo ratings yet
- Form Risk Assessment QEHSDocument2 pagesForm Risk Assessment QEHSArie Wicaksono100% (1)
- Artesunato MefloquinaDocument11 pagesArtesunato MefloquinaDavid CerrónNo ratings yet
- MSDS-Acumer 3100Document8 pagesMSDS-Acumer 3100daniNo ratings yet
- Cerebro Vascular Accident (CVA) - A Medical Case Study: Sophia GDocument13 pagesCerebro Vascular Accident (CVA) - A Medical Case Study: Sophia GAkash HalsanaNo ratings yet
- 2 Topical Fluoride For Caries Prevention 2013 UpdateDocument118 pages2 Topical Fluoride For Caries Prevention 2013 UpdateHub SciNo ratings yet
- Brosura Echipamente FitnessDocument265 pagesBrosura Echipamente FitnessDan DragutescuNo ratings yet
- Cost Utility Analysis: Mohammed A Mohammed B.pharm, M.clinpharm Clinical Pharmacist and LecturerDocument42 pagesCost Utility Analysis: Mohammed A Mohammed B.pharm, M.clinpharm Clinical Pharmacist and LecturerDr. Zirwa AsimNo ratings yet
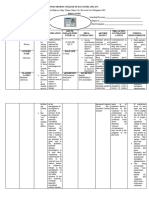
- Era University College of Nursing Lucknow: Submitted To-: Submitted byDocument7 pagesEra University College of Nursing Lucknow: Submitted To-: Submitted byAru Verma100% (1)
- 9 Condor Assessment SignoffDocument8 pages9 Condor Assessment SignoffAbhishek SrivastavaNo ratings yet
- The Benefits of Medical Marijuana For Cancer PatientsDocument4 pagesThe Benefits of Medical Marijuana For Cancer PatientsSheryl DiazNo ratings yet
- Lesson 3 Q2Document32 pagesLesson 3 Q2John michael SumagaysayNo ratings yet
- Resume of Periodontist, Prof. Dr. Ninad MoonDocument8 pagesResume of Periodontist, Prof. Dr. Ninad MoonProf. Dr. Ninad MoonNo ratings yet
- Diabetes in Elderly Adults: Graydon S. Meneilly and Daniel TessierDocument9 pagesDiabetes in Elderly Adults: Graydon S. Meneilly and Daniel Tessierdita prameswariNo ratings yet
- Infometiz EM Questions - 2023Document21 pagesInfometiz EM Questions - 2023lovelysihan22No ratings yet
- Harvard Clinical Psych Syllabus 2018Document4 pagesHarvard Clinical Psych Syllabus 2018PK MK SocNo ratings yet
- Hse360 2023 - NewDocument19 pagesHse360 2023 - Newadrian.zurawieckiNo ratings yet
- INvision Nov-2020 v2Document5 pagesINvision Nov-2020 v2Indiana Family to FamilyNo ratings yet
- B.ed DetailsDocument89 pagesB.ed DetailstanuNo ratings yet
- Dermatological Signs in Wilson's DiseaseDocument4 pagesDermatological Signs in Wilson's DiseaseGingerWiseNo ratings yet
- The Global Use of Medicine in 2019 and Outlook To 2023Document60 pagesThe Global Use of Medicine in 2019 and Outlook To 2023santiNo ratings yet
- Nandini KadabiDocument6 pagesNandini KadabiNandiniNo ratings yet
- Meeting Room Hazard Inspection ChecklistDocument3 pagesMeeting Room Hazard Inspection ChecklistAshishKiran SinghNo ratings yet
- Trauma Atls 2009Document2 pagesTrauma Atls 2009Jennifer IdrisNo ratings yet
- DTP Poblacion Annex-E-2 FinalDocument7 pagesDTP Poblacion Annex-E-2 FinalMario N. MariNo ratings yet
- PL-PBI-HSE 001 Project HSE PlanDocument22 pagesPL-PBI-HSE 001 Project HSE PlanTadaya KasaharaNo ratings yet