
Jurnal Urine Drainase Management
Jurnal Urine Drainase Management
You might also like
- Manejo Pós-ProstatectomiaDocument8 pagesManejo Pós-Prostatectomiapg230532No ratings yet
- A Review of Natural Orifice Translumenal Endoscopic Surgery (NOTES) For Intra-Abdominal SurgeryDocument20 pagesA Review of Natural Orifice Translumenal Endoscopic Surgery (NOTES) For Intra-Abdominal SurgerylifeofnameNo ratings yet
- World Journal of Emergency Surgery: Emergency Laparoscopy - Current Best PracticeDocument9 pagesWorld Journal of Emergency Surgery: Emergency Laparoscopy - Current Best PracticeHendra JojoNo ratings yet
- Reoperative Antireflux Surgery For Failed Fundoplication: An Analysis of Outcomes in 275 PatientsDocument8 pagesReoperative Antireflux Surgery For Failed Fundoplication: An Analysis of Outcomes in 275 PatientsDiego Andres VasquezNo ratings yet
- To Staple or Not To Staple The Symptomatic Rectocele: P. A. Lehur B. Pravini D. ChristoforidisDocument3 pagesTo Staple or Not To Staple The Symptomatic Rectocele: P. A. Lehur B. Pravini D. ChristoforidisHafidh HanifuddinNo ratings yet
- Robot-Assisted Laparoscopic Extravesical Ureteral Reimplantation - Technique Modifications Contribute To Optimized OutcomesDocument6 pagesRobot-Assisted Laparoscopic Extravesical Ureteral Reimplantation - Technique Modifications Contribute To Optimized OutcomesJulio GomezNo ratings yet
- J.ucl.2004.06.01120160802 7045 1jkcm4t With Cover Page v2Document18 pagesJ.ucl.2004.06.01120160802 7045 1jkcm4t With Cover Page v2Enika Natalia Christi TilaarNo ratings yet
- Complications of Enterocystoplastycase SeriesDocument5 pagesComplications of Enterocystoplastycase SeriesIJAR JOURNALNo ratings yet
- Urinary Diversion After Pelvic Exenteration For Gynecologic MalignanciesDocument10 pagesUrinary Diversion After Pelvic Exenteration For Gynecologic MalignanciesRara Aulia IINo ratings yet
- Systematic Review Go WakaDocument8 pagesSystematic Review Go WakaNoemi Di FucciaNo ratings yet
- Anesthesia For Major Urologic Surgery: James O.B. Cockcroft,, Colin B. Berry,, John S. Mcgrath,, Mark O. DaughertyDocument8 pagesAnesthesia For Major Urologic Surgery: James O.B. Cockcroft,, Colin B. Berry,, John S. Mcgrath,, Mark O. DaughertyJEFFERSON MUÑOZNo ratings yet
- Laparoscopic Entry TechniquesDocument9 pagesLaparoscopic Entry TechniquesDougNo ratings yet
- International Journal of Surgery: SciencedirectDocument7 pagesInternational Journal of Surgery: SciencedirectFerdian PriantoNo ratings yet
- LaparoscopeDocument9 pagesLaparoscopedharmaNo ratings yet
- Urinary Lithiasis Conventional Open Surgery2020Revista Da Associacao Medica BrasileiraOpen AccessDocument5 pagesUrinary Lithiasis Conventional Open Surgery2020Revista Da Associacao Medica BrasileiraOpen Accessdev darma karinggaNo ratings yet
- Estenosis de Uretra Posterior2015Document12 pagesEstenosis de Uretra Posterior2015Salv L RomoNo ratings yet
- Jurnal Urologi 4Document6 pagesJurnal Urologi 4dhimas permanaNo ratings yet
- Clinical Efficacy of Enhanced Recovery After Surgery in Percutaneous Nephrolithotripsy: A Randomized Controlled TrialDocument8 pagesClinical Efficacy of Enhanced Recovery After Surgery in Percutaneous Nephrolithotripsy: A Randomized Controlled TrialfaundraNo ratings yet
- Tecnica de Clips Nefrectomia ParcialDocument8 pagesTecnica de Clips Nefrectomia ParcialAlfredo BalcázarNo ratings yet
- Anesthesia For Robot-Assisted Radical Prostatectomy A Challenge For AnesthesiologistDocument5 pagesAnesthesia For Robot-Assisted Radical Prostatectomy A Challenge For AnesthesiologistMonse ContrerasNo ratings yet
- 1 s2.0 S0039606020306759 MainDocument9 pages1 s2.0 S0039606020306759 MainKar RodriguezNo ratings yet
- 2021 Techniques of Esophageal Anastomosis For EsophagectomyDocument14 pages2021 Techniques of Esophageal Anastomosis For EsophagectomyykommNo ratings yet
- Risk Factor UtiDocument7 pagesRisk Factor UtiNovi RobiyantiNo ratings yet
- Pleural Procedures in Critically Ill PatientsDocument9 pagesPleural Procedures in Critically Ill PatientsFlávio VillaNo ratings yet
- 10.1007@s13304 020 00817 3Document8 pages10.1007@s13304 020 00817 3syeda rabikaNo ratings yet
- Open CholecystectomyDocument11 pagesOpen CholecystectomyDaywalker PedragozaNo ratings yet
- Laparoscopic Surgery in Gynaecologic OncologyDocument7 pagesLaparoscopic Surgery in Gynaecologic OncologyManan BoobNo ratings yet
- s13304 021 01115 2Document8 pagess13304 021 01115 2Fatma BalciNo ratings yet
- Pda Ev Ejtcs 04Document7 pagesPda Ev Ejtcs 04emmanuel le bretNo ratings yet
- Colo RectalDocument6 pagesColo RectalHilyatul UlaNo ratings yet
- Semi-Rigid Ureteroscopy: Indications, Tips, and Tricks: Lily A. Whitehurst Bhaskar K. SomaniDocument7 pagesSemi-Rigid Ureteroscopy: Indications, Tips, and Tricks: Lily A. Whitehurst Bhaskar K. SomaniUmar FarooqNo ratings yet
- Efficacy and Safety of Early Drain Removal FollowiDocument12 pagesEfficacy and Safety of Early Drain Removal FollowiPablo FarinelliNo ratings yet
- 1 s2.0 S0302283815001578 MainDocument7 pages1 s2.0 S0302283815001578 MainyuenkeithNo ratings yet
- Percutaneous Ultrasound Guided Versus Open Cut Down Access To Femoral Vessels For The Placement of A REBOA CatheterDocument7 pagesPercutaneous Ultrasound Guided Versus Open Cut Down Access To Femoral Vessels For The Placement of A REBOA CatheterNormanNo ratings yet
- Casali 2009Document6 pagesCasali 2009Giancarlo Maruri MunarettoNo ratings yet
- Preliminary Comparison of The Modified Extraperitoneal free-PORT Single Incision Technique and Transabdominal Multi-Incision Robot-Assisted Laparoscopic Radical ProstatectomyDocument8 pagesPreliminary Comparison of The Modified Extraperitoneal free-PORT Single Incision Technique and Transabdominal Multi-Incision Robot-Assisted Laparoscopic Radical ProstatectomyVeciGugiNo ratings yet
- Shifting Paradigms in Minimally Invasive SurgeryDocument13 pagesShifting Paradigms in Minimally Invasive Surgeryflorence suyiNo ratings yet
- 1 s2.0 S1879522615003929 MainDocument4 pages1 s2.0 S1879522615003929 MainsagaNo ratings yet
- Articol ExtensoDocument5 pagesArticol ExtensoDavid CalinNo ratings yet
- 1 s2.0 S1015958421002621 MainDocument6 pages1 s2.0 S1015958421002621 MainLuiz Antônio PeratoneNo ratings yet
- 2020ICU - Icu 62 569Document8 pages2020ICU - Icu 62 569andryzell1987No ratings yet
- Urology Guidelines For Urethral StricturesDocument12 pagesUrology Guidelines For Urethral StricturesCh PrasadNo ratings yet
- Surgical Approaches To Esophageal CancerDocument6 pagesSurgical Approaches To Esophageal CancerYacine Tarik AizelNo ratings yet
- DereviDocument6 pagesDereviDerevie Hendryan MoulinaNo ratings yet
- Surgeons' Dilem M A Laparoscopic or Open Surgery?: Invited PaperDocument4 pagesSurgeons' Dilem M A Laparoscopic or Open Surgery?: Invited Papersuherman paleleNo ratings yet
- Management of Anastomotic Leaks After Esophagectomy and Gastric Pull-UpDocument9 pagesManagement of Anastomotic Leaks After Esophagectomy and Gastric Pull-UpSergio Sitta TarquiniNo ratings yet
- Ac 30 165Document10 pagesAc 30 165Zest IanNo ratings yet
- Retrograde Intrarenal Surgery An Expanding Role inDocument10 pagesRetrograde Intrarenal Surgery An Expanding Role inNenny HariyantoNo ratings yet
- Laparoscopic AdrenalectomyDocument12 pagesLaparoscopic AdrenalectomyTay SalinasNo ratings yet
- Current Status in Female Urology and GynDocument6 pagesCurrent Status in Female Urology and GynConsultorio Ginecología y ObstetriciaNo ratings yet
- Ampullary Carcinoma: Treatment and PrognosisDocument24 pagesAmpullary Carcinoma: Treatment and PrognosisHugo Alves100% (1)
- Retroperitoneal HeminephrectomyDocument4 pagesRetroperitoneal HeminephrectomyIoannis ValioulisNo ratings yet
- J Eururo 2016 05 020Document12 pagesJ Eururo 2016 05 020jedan185No ratings yet
- Single Mesh Lap HerniaDocument13 pagesSingle Mesh Lap HerniaRicky HarveyNo ratings yet
- Manejo de Estenosis Recidivante2016Document8 pagesManejo de Estenosis Recidivante2016Salv L RomoNo ratings yet
- Techniques and Outcomes of Bronchoplastic and Sleeve Resection: An 8-Year Single-Center ExperienceDocument11 pagesTechniques and Outcomes of Bronchoplastic and Sleeve Resection: An 8-Year Single-Center ExperienceJovelyn SagangNo ratings yet
- Roux-en-Y Reconstruction After PancreaticoduodenectomyDocument5 pagesRoux-en-Y Reconstruction After Pancreaticoduodenectomyyacine26No ratings yet
- Article - Risk Factor For Anastomotic Leak After Colon Resection For Cancer. 2015Document10 pagesArticle - Risk Factor For Anastomotic Leak After Colon Resection For Cancer. 2015Trí Cương NguyễnNo ratings yet
- Guidelines For The Clinical Application of Laparoscopic Biliary Tract SurgeryDocument37 pagesGuidelines For The Clinical Application of Laparoscopic Biliary Tract SurgeryTerence SalazarNo ratings yet
- Keys to Successful Orthotopic Bladder SubstitutionFrom EverandKeys to Successful Orthotopic Bladder SubstitutionUrs E. StuderNo ratings yet
- Central Venous Pressure Monitoring.: DR Jyothsna Chairperson DR Sunil ChhabriaDocument24 pagesCentral Venous Pressure Monitoring.: DR Jyothsna Chairperson DR Sunil ChhabriaPriyanka MaiyaNo ratings yet
- Orif ReportDocument5 pagesOrif ReportduypalaNo ratings yet
- HX400D6R AFJE3E 355CC-125 400-3-50 DatasheetDocument1 pageHX400D6R AFJE3E 355CC-125 400-3-50 DatasheetNduP78No ratings yet
- Writing Task 2Document50 pagesWriting Task 2Khanh Chi Pham100% (1)
- Microorganisms 11 01308Document26 pagesMicroorganisms 11 01308Alvaro SalinasNo ratings yet
- Employment Rights For Victims of Domestic or Sexual ViolenceDocument36 pagesEmployment Rights For Victims of Domestic or Sexual ViolenceLegal Momentum100% (2)
- List Obat ApotekDocument17 pagesList Obat ApotekAnonymous NIuKdo2xqtNo ratings yet
- 2020 JAADCR Araoye-Aguh CCCA Response To Topical MetforminDocument3 pages2020 JAADCR Araoye-Aguh CCCA Response To Topical MetforminKumar SukhdeoNo ratings yet
- One Lung Ventilation PDFDocument79 pagesOne Lung Ventilation PDFAnnetNo ratings yet
- Instruction Manual: E48W13A-AUDocument2 pagesInstruction Manual: E48W13A-AUDanilo100% (1)
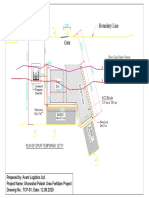
- Boundary Line: Plan of Gpuff Temporary JettyDocument1 pageBoundary Line: Plan of Gpuff Temporary Jettyshafiq_05No ratings yet
- List of NABL Accredited Labs PDFDocument47 pagesList of NABL Accredited Labs PDFAdarsh Kumar ManwalNo ratings yet
- Strategic Focus On 3R Principles Reveals Major Reductions in The Use of Animals in Pharmaceutical Toxicity TestingDocument12 pagesStrategic Focus On 3R Principles Reveals Major Reductions in The Use of Animals in Pharmaceutical Toxicity Testingapi-272484999No ratings yet
- Development of Normal Occlusion Part 2 Copy 2Document49 pagesDevelopment of Normal Occlusion Part 2 Copy 2MSA universityNo ratings yet
- Feel The Difference Owner'S Handbook: FordrangerDocument156 pagesFeel The Difference Owner'S Handbook: FordrangerGammy ZhammyNo ratings yet
- Phytochemical Screening and Antimicrobial Assay of Various SeedsDocument9 pagesPhytochemical Screening and Antimicrobial Assay of Various SeedsWendy FXNo ratings yet
- 240 IELTS Speaking Topics @IELTSDocument78 pages240 IELTS Speaking Topics @IELTShussy hussyNo ratings yet
- Viruses Wanted PosterDocument2 pagesViruses Wanted Posterapi-318809591No ratings yet
- SJNHC 212 431-434Document4 pagesSJNHC 212 431-434DAICY CULTURANo ratings yet
- Eatiing DisordersDocument69 pagesEatiing DisordersMasa MasaNo ratings yet
- People Vs Genosa - ParricideDocument8 pagesPeople Vs Genosa - ParricidegeorjalynjoyNo ratings yet
- Topic: Allowances: Delay AllowanceDocument35 pagesTopic: Allowances: Delay AllowanceharpominderNo ratings yet
- PRC Ready ReckonerDocument2 pagesPRC Ready Reckonersparthan300No ratings yet
- Boiler Thermal CalculationDocument83 pagesBoiler Thermal Calculation9913489806100% (1)
- Entrep - Product ProposalDocument4 pagesEntrep - Product ProposalPrincess ArabelaNo ratings yet
- UNIT#2 Power SourceDocument49 pagesUNIT#2 Power SourceRTPS CCRNo ratings yet
- EE311A 2021 AV Slides L23Document13 pagesEE311A 2021 AV Slides L23Ananya AgarwalNo ratings yet
- Toksikologi PDFDocument134 pagesToksikologi PDFPurwani Ni NyomanNo ratings yet
- Gogol's Wife LandolfiDocument6 pagesGogol's Wife LandolfiEbrahim Asadi100% (1)























































































Download as pdf or txt
You might also like
- Manejo Pós-ProstatectomiaDocument8 pagesManejo Pós-Prostatectomiapg230532No ratings yet
- A Review of Natural Orifice Translumenal Endoscopic Surgery (NOTES) For Intra-Abdominal SurgeryDocument20 pagesA Review of Natural Orifice Translumenal Endoscopic Surgery (NOTES) For Intra-Abdominal SurgerylifeofnameNo ratings yet
- World Journal of Emergency Surgery: Emergency Laparoscopy - Current Best PracticeDocument9 pagesWorld Journal of Emergency Surgery: Emergency Laparoscopy - Current Best PracticeHendra JojoNo ratings yet
- Reoperative Antireflux Surgery For Failed Fundoplication: An Analysis of Outcomes in 275 PatientsDocument8 pagesReoperative Antireflux Surgery For Failed Fundoplication: An Analysis of Outcomes in 275 PatientsDiego Andres VasquezNo ratings yet
- To Staple or Not To Staple The Symptomatic Rectocele: P. A. Lehur B. Pravini D. ChristoforidisDocument3 pagesTo Staple or Not To Staple The Symptomatic Rectocele: P. A. Lehur B. Pravini D. ChristoforidisHafidh HanifuddinNo ratings yet
- Robot-Assisted Laparoscopic Extravesical Ureteral Reimplantation - Technique Modifications Contribute To Optimized OutcomesDocument6 pagesRobot-Assisted Laparoscopic Extravesical Ureteral Reimplantation - Technique Modifications Contribute To Optimized OutcomesJulio GomezNo ratings yet
- J.ucl.2004.06.01120160802 7045 1jkcm4t With Cover Page v2Document18 pagesJ.ucl.2004.06.01120160802 7045 1jkcm4t With Cover Page v2Enika Natalia Christi TilaarNo ratings yet
- Complications of Enterocystoplastycase SeriesDocument5 pagesComplications of Enterocystoplastycase SeriesIJAR JOURNALNo ratings yet
- Urinary Diversion After Pelvic Exenteration For Gynecologic MalignanciesDocument10 pagesUrinary Diversion After Pelvic Exenteration For Gynecologic MalignanciesRara Aulia IINo ratings yet
- Systematic Review Go WakaDocument8 pagesSystematic Review Go WakaNoemi Di FucciaNo ratings yet
- Anesthesia For Major Urologic Surgery: James O.B. Cockcroft,, Colin B. Berry,, John S. Mcgrath,, Mark O. DaughertyDocument8 pagesAnesthesia For Major Urologic Surgery: James O.B. Cockcroft,, Colin B. Berry,, John S. Mcgrath,, Mark O. DaughertyJEFFERSON MUÑOZNo ratings yet
- Laparoscopic Entry TechniquesDocument9 pagesLaparoscopic Entry TechniquesDougNo ratings yet
- International Journal of Surgery: SciencedirectDocument7 pagesInternational Journal of Surgery: SciencedirectFerdian PriantoNo ratings yet
- LaparoscopeDocument9 pagesLaparoscopedharmaNo ratings yet
- Urinary Lithiasis Conventional Open Surgery2020Revista Da Associacao Medica BrasileiraOpen AccessDocument5 pagesUrinary Lithiasis Conventional Open Surgery2020Revista Da Associacao Medica BrasileiraOpen Accessdev darma karinggaNo ratings yet
- Estenosis de Uretra Posterior2015Document12 pagesEstenosis de Uretra Posterior2015Salv L RomoNo ratings yet
- Jurnal Urologi 4Document6 pagesJurnal Urologi 4dhimas permanaNo ratings yet
- Clinical Efficacy of Enhanced Recovery After Surgery in Percutaneous Nephrolithotripsy: A Randomized Controlled TrialDocument8 pagesClinical Efficacy of Enhanced Recovery After Surgery in Percutaneous Nephrolithotripsy: A Randomized Controlled TrialfaundraNo ratings yet
- Tecnica de Clips Nefrectomia ParcialDocument8 pagesTecnica de Clips Nefrectomia ParcialAlfredo BalcázarNo ratings yet
- Anesthesia For Robot-Assisted Radical Prostatectomy A Challenge For AnesthesiologistDocument5 pagesAnesthesia For Robot-Assisted Radical Prostatectomy A Challenge For AnesthesiologistMonse ContrerasNo ratings yet
- 1 s2.0 S0039606020306759 MainDocument9 pages1 s2.0 S0039606020306759 MainKar RodriguezNo ratings yet
- 2021 Techniques of Esophageal Anastomosis For EsophagectomyDocument14 pages2021 Techniques of Esophageal Anastomosis For EsophagectomyykommNo ratings yet
- Risk Factor UtiDocument7 pagesRisk Factor UtiNovi RobiyantiNo ratings yet
- Pleural Procedures in Critically Ill PatientsDocument9 pagesPleural Procedures in Critically Ill PatientsFlávio VillaNo ratings yet
- 10.1007@s13304 020 00817 3Document8 pages10.1007@s13304 020 00817 3syeda rabikaNo ratings yet
- Open CholecystectomyDocument11 pagesOpen CholecystectomyDaywalker PedragozaNo ratings yet
- Laparoscopic Surgery in Gynaecologic OncologyDocument7 pagesLaparoscopic Surgery in Gynaecologic OncologyManan BoobNo ratings yet
- s13304 021 01115 2Document8 pagess13304 021 01115 2Fatma BalciNo ratings yet
- Pda Ev Ejtcs 04Document7 pagesPda Ev Ejtcs 04emmanuel le bretNo ratings yet
- Colo RectalDocument6 pagesColo RectalHilyatul UlaNo ratings yet
- Semi-Rigid Ureteroscopy: Indications, Tips, and Tricks: Lily A. Whitehurst Bhaskar K. SomaniDocument7 pagesSemi-Rigid Ureteroscopy: Indications, Tips, and Tricks: Lily A. Whitehurst Bhaskar K. SomaniUmar FarooqNo ratings yet
- Efficacy and Safety of Early Drain Removal FollowiDocument12 pagesEfficacy and Safety of Early Drain Removal FollowiPablo FarinelliNo ratings yet
- 1 s2.0 S0302283815001578 MainDocument7 pages1 s2.0 S0302283815001578 MainyuenkeithNo ratings yet
- Percutaneous Ultrasound Guided Versus Open Cut Down Access To Femoral Vessels For The Placement of A REBOA CatheterDocument7 pagesPercutaneous Ultrasound Guided Versus Open Cut Down Access To Femoral Vessels For The Placement of A REBOA CatheterNormanNo ratings yet
- Casali 2009Document6 pagesCasali 2009Giancarlo Maruri MunarettoNo ratings yet
- Preliminary Comparison of The Modified Extraperitoneal free-PORT Single Incision Technique and Transabdominal Multi-Incision Robot-Assisted Laparoscopic Radical ProstatectomyDocument8 pagesPreliminary Comparison of The Modified Extraperitoneal free-PORT Single Incision Technique and Transabdominal Multi-Incision Robot-Assisted Laparoscopic Radical ProstatectomyVeciGugiNo ratings yet
- Shifting Paradigms in Minimally Invasive SurgeryDocument13 pagesShifting Paradigms in Minimally Invasive Surgeryflorence suyiNo ratings yet
- 1 s2.0 S1879522615003929 MainDocument4 pages1 s2.0 S1879522615003929 MainsagaNo ratings yet
- Articol ExtensoDocument5 pagesArticol ExtensoDavid CalinNo ratings yet
- 1 s2.0 S1015958421002621 MainDocument6 pages1 s2.0 S1015958421002621 MainLuiz Antônio PeratoneNo ratings yet
- 2020ICU - Icu 62 569Document8 pages2020ICU - Icu 62 569andryzell1987No ratings yet
- Urology Guidelines For Urethral StricturesDocument12 pagesUrology Guidelines For Urethral StricturesCh PrasadNo ratings yet
- Surgical Approaches To Esophageal CancerDocument6 pagesSurgical Approaches To Esophageal CancerYacine Tarik AizelNo ratings yet
- DereviDocument6 pagesDereviDerevie Hendryan MoulinaNo ratings yet
- Surgeons' Dilem M A Laparoscopic or Open Surgery?: Invited PaperDocument4 pagesSurgeons' Dilem M A Laparoscopic or Open Surgery?: Invited Papersuherman paleleNo ratings yet
- Management of Anastomotic Leaks After Esophagectomy and Gastric Pull-UpDocument9 pagesManagement of Anastomotic Leaks After Esophagectomy and Gastric Pull-UpSergio Sitta TarquiniNo ratings yet
- Ac 30 165Document10 pagesAc 30 165Zest IanNo ratings yet
- Retrograde Intrarenal Surgery An Expanding Role inDocument10 pagesRetrograde Intrarenal Surgery An Expanding Role inNenny HariyantoNo ratings yet
- Laparoscopic AdrenalectomyDocument12 pagesLaparoscopic AdrenalectomyTay SalinasNo ratings yet
- Current Status in Female Urology and GynDocument6 pagesCurrent Status in Female Urology and GynConsultorio Ginecología y ObstetriciaNo ratings yet
- Ampullary Carcinoma: Treatment and PrognosisDocument24 pagesAmpullary Carcinoma: Treatment and PrognosisHugo Alves100% (1)
- Retroperitoneal HeminephrectomyDocument4 pagesRetroperitoneal HeminephrectomyIoannis ValioulisNo ratings yet
- J Eururo 2016 05 020Document12 pagesJ Eururo 2016 05 020jedan185No ratings yet
- Single Mesh Lap HerniaDocument13 pagesSingle Mesh Lap HerniaRicky HarveyNo ratings yet
- Manejo de Estenosis Recidivante2016Document8 pagesManejo de Estenosis Recidivante2016Salv L RomoNo ratings yet
- Techniques and Outcomes of Bronchoplastic and Sleeve Resection: An 8-Year Single-Center ExperienceDocument11 pagesTechniques and Outcomes of Bronchoplastic and Sleeve Resection: An 8-Year Single-Center ExperienceJovelyn SagangNo ratings yet
- Roux-en-Y Reconstruction After PancreaticoduodenectomyDocument5 pagesRoux-en-Y Reconstruction After Pancreaticoduodenectomyyacine26No ratings yet
- Article - Risk Factor For Anastomotic Leak After Colon Resection For Cancer. 2015Document10 pagesArticle - Risk Factor For Anastomotic Leak After Colon Resection For Cancer. 2015Trí Cương NguyễnNo ratings yet
- Guidelines For The Clinical Application of Laparoscopic Biliary Tract SurgeryDocument37 pagesGuidelines For The Clinical Application of Laparoscopic Biliary Tract SurgeryTerence SalazarNo ratings yet
- Keys to Successful Orthotopic Bladder SubstitutionFrom EverandKeys to Successful Orthotopic Bladder SubstitutionUrs E. StuderNo ratings yet
- Central Venous Pressure Monitoring.: DR Jyothsna Chairperson DR Sunil ChhabriaDocument24 pagesCentral Venous Pressure Monitoring.: DR Jyothsna Chairperson DR Sunil ChhabriaPriyanka MaiyaNo ratings yet
- Orif ReportDocument5 pagesOrif ReportduypalaNo ratings yet
- HX400D6R AFJE3E 355CC-125 400-3-50 DatasheetDocument1 pageHX400D6R AFJE3E 355CC-125 400-3-50 DatasheetNduP78No ratings yet
- Writing Task 2Document50 pagesWriting Task 2Khanh Chi Pham100% (1)
- Microorganisms 11 01308Document26 pagesMicroorganisms 11 01308Alvaro SalinasNo ratings yet
- Employment Rights For Victims of Domestic or Sexual ViolenceDocument36 pagesEmployment Rights For Victims of Domestic or Sexual ViolenceLegal Momentum100% (2)
- List Obat ApotekDocument17 pagesList Obat ApotekAnonymous NIuKdo2xqtNo ratings yet
- 2020 JAADCR Araoye-Aguh CCCA Response To Topical MetforminDocument3 pages2020 JAADCR Araoye-Aguh CCCA Response To Topical MetforminKumar SukhdeoNo ratings yet
- One Lung Ventilation PDFDocument79 pagesOne Lung Ventilation PDFAnnetNo ratings yet
- Instruction Manual: E48W13A-AUDocument2 pagesInstruction Manual: E48W13A-AUDanilo100% (1)
- Boundary Line: Plan of Gpuff Temporary JettyDocument1 pageBoundary Line: Plan of Gpuff Temporary Jettyshafiq_05No ratings yet
- List of NABL Accredited Labs PDFDocument47 pagesList of NABL Accredited Labs PDFAdarsh Kumar ManwalNo ratings yet
- Strategic Focus On 3R Principles Reveals Major Reductions in The Use of Animals in Pharmaceutical Toxicity TestingDocument12 pagesStrategic Focus On 3R Principles Reveals Major Reductions in The Use of Animals in Pharmaceutical Toxicity Testingapi-272484999No ratings yet
- Development of Normal Occlusion Part 2 Copy 2Document49 pagesDevelopment of Normal Occlusion Part 2 Copy 2MSA universityNo ratings yet
- Feel The Difference Owner'S Handbook: FordrangerDocument156 pagesFeel The Difference Owner'S Handbook: FordrangerGammy ZhammyNo ratings yet
- Phytochemical Screening and Antimicrobial Assay of Various SeedsDocument9 pagesPhytochemical Screening and Antimicrobial Assay of Various SeedsWendy FXNo ratings yet
- 240 IELTS Speaking Topics @IELTSDocument78 pages240 IELTS Speaking Topics @IELTShussy hussyNo ratings yet
- Viruses Wanted PosterDocument2 pagesViruses Wanted Posterapi-318809591No ratings yet
- SJNHC 212 431-434Document4 pagesSJNHC 212 431-434DAICY CULTURANo ratings yet
- Eatiing DisordersDocument69 pagesEatiing DisordersMasa MasaNo ratings yet
- People Vs Genosa - ParricideDocument8 pagesPeople Vs Genosa - ParricidegeorjalynjoyNo ratings yet
- Topic: Allowances: Delay AllowanceDocument35 pagesTopic: Allowances: Delay AllowanceharpominderNo ratings yet
- PRC Ready ReckonerDocument2 pagesPRC Ready Reckonersparthan300No ratings yet
- Boiler Thermal CalculationDocument83 pagesBoiler Thermal Calculation9913489806100% (1)
- Entrep - Product ProposalDocument4 pagesEntrep - Product ProposalPrincess ArabelaNo ratings yet
- UNIT#2 Power SourceDocument49 pagesUNIT#2 Power SourceRTPS CCRNo ratings yet
- EE311A 2021 AV Slides L23Document13 pagesEE311A 2021 AV Slides L23Ananya AgarwalNo ratings yet
- Toksikologi PDFDocument134 pagesToksikologi PDFPurwani Ni NyomanNo ratings yet
- Gogol's Wife LandolfiDocument6 pagesGogol's Wife LandolfiEbrahim Asadi100% (1)