Download as pdf or txt
You might also like
- Sinclair Method AlcoholDocument24 pagesSinclair Method AlcoholToni ErdfeldNo ratings yet
- Assessment Inferen CE Plannin G Interve Ntion Rationa LE Evalua TionDocument4 pagesAssessment Inferen CE Plannin G Interve Ntion Rationa LE Evalua TionBg Celo33% (3)
- Nursing Care Plan AppendicitisDocument2 pagesNursing Care Plan Appendicitisderic95% (57)
- Crede's ProphyaxisDocument12 pagesCrede's ProphyaxisNikki M. Arapol100% (1)
- Tetanus: Andrew Michael Taylor FRCADocument4 pagesTetanus: Andrew Michael Taylor FRCAILHAM AMIENNo ratings yet
- Afshar 2011Document8 pagesAfshar 2011Kami LyaNo ratings yet
- Brook 2008Document10 pagesBrook 2008Kami LyaNo ratings yet
- Tetanus in Developing Countries: A Review and Case Series: Ingole KV, Mundhada SG, Powar RMDocument5 pagesTetanus in Developing Countries: A Review and Case Series: Ingole KV, Mundhada SG, Powar RMRizka ApNo ratings yet
- TetanusDocument35 pagesTetanusJulie FurioNo ratings yet
- Questions and Answers: TetanusDocument4 pagesQuestions and Answers: TetanusRhodjan RescoNo ratings yet
- K6 SLIDE-MANAGEMENT OF TETANUS IN PEDIATRIC-baruDocument69 pagesK6 SLIDE-MANAGEMENT OF TETANUS IN PEDIATRIC-baruRaja Alfian IrawanNo ratings yet
- Questions and Answers: TetanusDocument4 pagesQuestions and Answers: TetanusJahanzaib NiaziNo ratings yet
- Questions and Answers: TetanusDocument4 pagesQuestions and Answers: TetanuszippyzevenNo ratings yet
- Microbiology of Clostridium Tetani and Wound ClassificationDocument3 pagesMicrobiology of Clostridium Tetani and Wound ClassificationAZIZAH ARDINALNo ratings yet
- Clostridium Tetani: Scientific ClassificationDocument4 pagesClostridium Tetani: Scientific ClassificationGael Forbes RealNo ratings yet
- 388tetanus For WebsiteDocument51 pages388tetanus For Websitehafiz ikhsanNo ratings yet
- Management and Prevention of Tetanus: Abstract: THDocument16 pagesManagement and Prevention of Tetanus: Abstract: THFabian FabiansyahNo ratings yet
- Lovely Professional University: Term Paper of Advanced MicrobiologyDocument11 pagesLovely Professional University: Term Paper of Advanced Microbiology27AlokKumarNo ratings yet
- Tetanus: Maria Banica & Sophie NamDocument19 pagesTetanus: Maria Banica & Sophie NamSuwantin Indra SariNo ratings yet
- Tetanus Pathophysiology, Clinical Signs, DiagnosisDocument9 pagesTetanus Pathophysiology, Clinical Signs, DiagnosisJuris Isaac Perez VianaNo ratings yet
- Neonatal TetanusDocument44 pagesNeonatal TetanusJake MillerNo ratings yet
- TetanusDocument3 pagesTetanusmake_jajoeNo ratings yet
- TetanusDocument12 pagesTetanustinkerbell03No ratings yet
- The Pa Tho Physiology of TetanusDocument3 pagesThe Pa Tho Physiology of Tetanusmai_serpicNo ratings yet
- Brief: Tetanus Disease, Treatment, ManagementDocument5 pagesBrief: Tetanus Disease, Treatment, ManagementchindiaNo ratings yet
- Clostridia in CattleDocument6 pagesClostridia in Cattleamamùra maamarNo ratings yet
- Clostridium Tetan1Document4 pagesClostridium Tetan1Jul SkynEtNo ratings yet
- Tetanus: A Potential Public Health Threat in Times of DisasterDocument4 pagesTetanus: A Potential Public Health Threat in Times of DisasterNasriNo ratings yet
- Toxoplasmosis: A Global Infection, So Widespread, So NeglectedDocument6 pagesToxoplasmosis: A Global Infection, So Widespread, So NeglectedIndah Yulinda PramestyNo ratings yet
- Tetanu S: By: Reno WaisyahDocument18 pagesTetanu S: By: Reno WaisyahReno WaisyahNo ratings yet
- Status InternusDocument12 pagesStatus InternusPriscaNo ratings yet
- The GENUS ClostridiumDocument28 pagesThe GENUS ClostridiumrohishaakNo ratings yet
- Tetanus: "Lock Jaw"Document10 pagesTetanus: "Lock Jaw"Atoillah IsvandiaryNo ratings yet
- TETANUSDocument17 pagesTETANUST. Chang100% (1)
- Tetanus PDFDocument10 pagesTetanus PDFVina MuspitaNo ratings yet
- !tetanus MDocument22 pages!tetanus MWendo yayahNo ratings yet
- Tetanus: Ma. Theresa Dj. YumangDocument28 pagesTetanus: Ma. Theresa Dj. YumangJean SarocamNo ratings yet
- Tetanus in Animals - Summary of Knowledge Malinovská, Z., Čonková, E., Váczi, PDocument7 pagesTetanus in Animals - Summary of Knowledge Malinovská, Z., Čonková, E., Váczi, PSophieNo ratings yet
- Tetanus 9 eDocument10 pagesTetanus 9 ea.hooker114No ratings yet
- Tetanus EmedicineDocument19 pagesTetanus EmedicineSapto SutardiNo ratings yet
- Group 2 TetanusDocument43 pagesGroup 2 TetanusDaymon, Ma. TeresaNo ratings yet
- Tetanus and BotulismDocument40 pagesTetanus and BotulismPatriceNo ratings yet
- Clinical Bacteriology: by Fawad Mahmood M.Phil. Medical Laboratory SciencesDocument26 pagesClinical Bacteriology: by Fawad Mahmood M.Phil. Medical Laboratory SciencesFawad SawabiNo ratings yet
- TetanusDocument4 pagesTetanuseagame gamersNo ratings yet
- TETAPOTADocument2 pagesTETAPOTArealme 6iNo ratings yet
- Pa Tho GenesisDocument11 pagesPa Tho GenesisBeth AvelinoNo ratings yet
- Tetanus: BackgroundDocument19 pagesTetanus: BackgroundYovita Devi KornelinNo ratings yet
- Clostridium Tetani: Infections in Newborn Infants: A Tetanus Neonatorum ReviewDocument8 pagesClostridium Tetani: Infections in Newborn Infants: A Tetanus Neonatorum ReviewNurul HikmahNo ratings yet
- Tetanus - The DiseaseDocument6 pagesTetanus - The Diseasemanjunath mamathaNo ratings yet
- Tetanus (Harrison's Principle of Internal Medicine)Document4 pagesTetanus (Harrison's Principle of Internal Medicine)Renz Mervin Rivera100% (1)
- Preventing Fetal Exposure To TETRATOGENSDocument6 pagesPreventing Fetal Exposure To TETRATOGENSEuna Patricia AguilarNo ratings yet
- Tetanus: C. L. ThwaitesDocument8 pagesTetanus: C. L. ThwaitesnurdiansyahNo ratings yet
- Acute Medicine Surgery - 2023 - Yamaguchi - The Threat of A New Tetanus Outbreak Due To Urban Flooding Disaster RequiresDocument9 pagesAcute Medicine Surgery - 2023 - Yamaguchi - The Threat of A New Tetanus Outbreak Due To Urban Flooding Disaster Requiresfitri dwiyantiNo ratings yet
- PEDIA Bacterial Infections Part 2 Dr. E. Lim FinalDocument5 pagesPEDIA Bacterial Infections Part 2 Dr. E. Lim FinalClaire DuNo ratings yet
- TetanusDocument23 pagesTetanusRiska PriyaniNo ratings yet
- TetanusDocument79 pagesTetanusSan MohapatraNo ratings yet
- Streptococcus Pneumoniae 2. Hemophilus Influenzae 3. Neisseria MeningitidesDocument4 pagesStreptococcus Pneumoniae 2. Hemophilus Influenzae 3. Neisseria Meningitidesa i r i e sNo ratings yet
- Tetanus Toxoid: Section TwoDocument1 pageTetanus Toxoid: Section TwoRaulimar Hernandez RamosNo ratings yet
- TTVDocument5 pagesTTVGlorious Tufon Neba EmmanuelNo ratings yet
- Zoonotic Infections 10Document21 pagesZoonotic Infections 10Chaudhary AjayNo ratings yet
- Brucellosis: The Short Textbook of PediatricsDocument3 pagesBrucellosis: The Short Textbook of PediatricsHosny M IsseNo ratings yet
- Tetanu S: Dr. MaslianiDocument74 pagesTetanu S: Dr. MaslianiHengky HanggaraNo ratings yet
- Cats and Toxoplasma: A Comprehensive Guide to Feline ToxoplasmosisFrom EverandCats and Toxoplasma: A Comprehensive Guide to Feline ToxoplasmosisNo ratings yet
- Familial Mediterranean FeverFrom EverandFamilial Mediterranean FeverMarco GattornoNo ratings yet
- JRCM 8 32Document4 pagesJRCM 8 32eagame gamersNo ratings yet
- Erythrasma Revisited: Diagnosis, Differential Diagnoses, and Comprehensive Review of TreatmentDocument7 pagesErythrasma Revisited: Diagnosis, Differential Diagnoses, and Comprehensive Review of Treatmenteagame gamersNo ratings yet
- Gastritis ManuscriptpresentationDocument12 pagesGastritis Manuscriptpresentationeagame gamersNo ratings yet
- Guillain-Barré Syndrome: Clinical ManifestationsDocument7 pagesGuillain-Barré Syndrome: Clinical Manifestationseagame gamersNo ratings yet
- Tetanus NeonatorumDocument1 pageTetanus Neonatorumeagame gamersNo ratings yet
- TetanusDocument4 pagesTetanuseagame gamersNo ratings yet
- Tetanus NeonatorumDocument6 pagesTetanus Neonatorumeagame gamersNo ratings yet
- Hyperbaric Oxygen in Critical CareDocument4 pagesHyperbaric Oxygen in Critical Careeagame gamersNo ratings yet
- Diving MedicineDocument14 pagesDiving Medicineeagame gamersNo ratings yet
- Atypical Antipsychotics and Newer AntidepressantsDocument21 pagesAtypical Antipsychotics and Newer Antidepressantseagame gamersNo ratings yet
- The Periodontal Index: A. L. Russell ExaminingDocument7 pagesThe Periodontal Index: A. L. Russell ExaminingVivek PatelNo ratings yet
- Poultry DiseasesDocument5 pagesPoultry DiseasesAnjum IslamNo ratings yet
- Level of Disease PreventionDocument16 pagesLevel of Disease Preventionenam professorNo ratings yet
- Reverse TrendelenburgDocument1 pageReverse TrendelenburgJamielyn BassigNo ratings yet
- Composite Vs Amalgam PowerpointDocument17 pagesComposite Vs Amalgam Powerpointapi-322463366100% (1)
- Colon, Rectum and Anus-Dr. SigitDocument121 pagesColon, Rectum and Anus-Dr. SigitYuliana Latif100% (1)
- Informed Consent: Lena Haygood (R) RT Radiology Instructor: Arizona Western Community College SourceDocument18 pagesInformed Consent: Lena Haygood (R) RT Radiology Instructor: Arizona Western Community College SourceJerry AbleNo ratings yet
- Acute AppendicitisDocument50 pagesAcute AppendicitisDeslia SupriyadiNo ratings yet
- AIIMS PG Jan 2015Document50 pagesAIIMS PG Jan 2015AnweshaBoseNo ratings yet
- Written Assignment Unit 2 EDUC 5420Document7 pagesWritten Assignment Unit 2 EDUC 5420RimaNo ratings yet
- Establishment Licenses Issued Under MDR, 2017 - FORM 4Document41 pagesEstablishment Licenses Issued Under MDR, 2017 - FORM 4AmberSattiNo ratings yet
- Department of Education: Annual Gender and Development (Gad) Plan and BudgetDocument6 pagesDepartment of Education: Annual Gender and Development (Gad) Plan and BudgetJaymar Padayao0% (1)
- BAXIE (M-UE-22) : Eight PathogensDocument1 pageBAXIE (M-UE-22) : Eight Pathogensray72roNo ratings yet
- School Form 2 Daily Attendance Report of Learners For Senior High School (SF2-SHS)Document3 pagesSchool Form 2 Daily Attendance Report of Learners For Senior High School (SF2-SHS)Jemarjo SalandananNo ratings yet
- Suicide in Children and Adolescents Cambridge Child and Adolescent PsychiatryDocument333 pagesSuicide in Children and Adolescents Cambridge Child and Adolescent PsychiatryFlorin Tudose100% (1)
- Autoimmune Hemolytic AnemiaDocument7 pagesAutoimmune Hemolytic AnemiaHoopmen SilaenNo ratings yet
- Control and RandomizationDocument18 pagesControl and RandomizationRARCHITA SHARMANo ratings yet
- Health Problem Family Nursing Problem Goal of Care Objectives of Care Intervention Plan Resources Required EvaluationDocument2 pagesHealth Problem Family Nursing Problem Goal of Care Objectives of Care Intervention Plan Resources Required EvaluationLuis WashingtonNo ratings yet
- Guidelines For Preventing Workplace Violence For Healthcare and Social Service WorkersDocument60 pagesGuidelines For Preventing Workplace Violence For Healthcare and Social Service WorkersSafety and Health magazineNo ratings yet
- Stroke Hemoragik: Yusi Rizky N 1 6 1 0 2 1 1 0 5 1Document19 pagesStroke Hemoragik: Yusi Rizky N 1 6 1 0 2 1 1 0 5 1Yusi RizkyNo ratings yet
- National Nursing Audit Ministry of Health Malaysia Version 3 April 2019 P5VSDocument4 pagesNational Nursing Audit Ministry of Health Malaysia Version 3 April 2019 P5VSmhd hasnanNo ratings yet
- Redacted Complaint Beaudoin V Baker FinalDocument25 pagesRedacted Complaint Beaudoin V Baker FinalKyle BeckerNo ratings yet
- Neonatal Mechanical Ventilation Predictors of Mortality and OutcomesDocument8 pagesNeonatal Mechanical Ventilation Predictors of Mortality and OutcomesAthenaeum Scientific PublishersNo ratings yet
- Lecture - Nutrition and Diet TherapyDocument9 pagesLecture - Nutrition and Diet TherapyLalaine Marie BianzonNo ratings yet
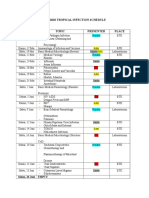
- Imo Tropical Infection ScheduleDocument3 pagesImo Tropical Infection ScheduleHendroMaleNo ratings yet
- Andrew Tran ResumeDocument2 pagesAndrew Tran Resumeapi-465054778No ratings yet