Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Inquiries, Investigations and Immersion: Quarter 3 - Module 3Document24 pagesInquiries, Investigations and Immersion: Quarter 3 - Module 3Mlyn78% (49)
- Enfermedades Metabólicas Del NeonatoDocument254 pagesEnfermedades Metabólicas Del NeonatoMaria Del Mar Marulanda GrizalesNo ratings yet
- Markerless Measurement and Evaluation of General Movements in InfantsDocument13 pagesMarkerless Measurement and Evaluation of General Movements in InfantsMaria Del Mar Marulanda GrizalesNo ratings yet
- Food Chemistry: A A A B A ADocument8 pagesFood Chemistry: A A A B A AMaria Del Mar Marulanda GrizalesNo ratings yet
- The General Movement Checklista Guide To The Assessment of General Movements During Preterm and Term AgeDocument8 pagesThe General Movement Checklista Guide To The Assessment of General Movements During Preterm and Term AgeMaria Del Mar Marulanda GrizalesNo ratings yet
- Addition of Kinesio Taping of The Orbicularis Oris Muscles To Speech Therapy Rapidly Improves Drooling in Children With Neurological Disorders, 2019Document7 pagesAddition of Kinesio Taping of The Orbicularis Oris Muscles To Speech Therapy Rapidly Improves Drooling in Children With Neurological Disorders, 2019Maria Del Mar Marulanda GrizalesNo ratings yet
- Early Human Development: SciencedirectDocument7 pagesEarly Human Development: SciencedirectMaria Del Mar Marulanda GrizalesNo ratings yet
- Effects of Kinesio Taping in Rectus Femoris Activity and Sit-To-Stand Movement in Children With Unilateral Cerebral Palsy - Placebo-Controlled, Repeated-Measure Design 2018Document12 pagesEffects of Kinesio Taping in Rectus Femoris Activity and Sit-To-Stand Movement in Children With Unilateral Cerebral Palsy - Placebo-Controlled, Repeated-Measure Design 2018Maria Del Mar Marulanda GrizalesNo ratings yet
- NeuropsicologiaDocument10 pagesNeuropsicologiaMaria Del Mar Marulanda GrizalesNo ratings yet
- Articulo AutismoDocument28 pagesArticulo AutismoMaria Del Mar Marulanda GrizalesNo ratings yet
- Southern Nevada Health District Coronavirus GuidelinesDocument2 pagesSouthern Nevada Health District Coronavirus GuidelinesLas Vegas Review-JournalNo ratings yet
- Covid 19 Was A 360-Degree ChangeDocument1 pageCovid 19 Was A 360-Degree ChangeValeria GiraldoNo ratings yet
- Philippine College of Occupational Medicine, Inc.: Phil M. Pangilinan, MD, Mha, FPSMS, Dpcom, PafpDocument3 pagesPhilippine College of Occupational Medicine, Inc.: Phil M. Pangilinan, MD, Mha, FPSMS, Dpcom, PafpANNLNo ratings yet
- WHO MOOC Clinical Management Course 1 Module 6Document20 pagesWHO MOOC Clinical Management Course 1 Module 6MariaNo ratings yet
- Annual Report 2066 67Document581 pagesAnnual Report 2066 67Rajeev NepalNo ratings yet
- Sample Id: 18344783 Icmr Specimen Referral Form For Covid-19 (Sars-Cov2)Document2 pagesSample Id: 18344783 Icmr Specimen Referral Form For Covid-19 (Sars-Cov2)Asupalli SirishaNo ratings yet
- Corona Virus (COVID 19) Natural SupplementsDocument28 pagesCorona Virus (COVID 19) Natural SupplementscwoolNo ratings yet
- Marijuana Businesses COVID LetterDocument3 pagesMarijuana Businesses COVID LetterMarijuana Moment100% (1)
- Long-COVID-international Guidelines-2023Document201 pagesLong-COVID-international Guidelines-2023Zezinho zéNo ratings yet
- The Impact of The COVID-19 Pandemic Crisis On The Travel and Tourism Sector - UK EvidenceDocument19 pagesThe Impact of The COVID-19 Pandemic Crisis On The Travel and Tourism Sector - UK EvidenceMohammadOmarFaruq67% (3)
- Impact of The COVID-19 Pandemic On Mental Health and Quality of Life Among Local Residents in Liaoning Province, China: A Cross-Sectional StudyDocument12 pagesImpact of The COVID-19 Pandemic On Mental Health and Quality of Life Among Local Residents in Liaoning Province, China: A Cross-Sectional StudyieykatalibNo ratings yet
- Botanicals For Upper Respiratory Conditions: Key PointsDocument6 pagesBotanicals For Upper Respiratory Conditions: Key PointslouisaNo ratings yet
- 21 02 26-CSCS Assessment Summary-Written-ReportDocument27 pages21 02 26-CSCS Assessment Summary-Written-ReportTesfayeNo ratings yet
- Notice of Decision - FOI 2338Document10 pagesNotice of Decision - FOI 2338paulfarrellNo ratings yet
- Health and Safety Guidelines Governing The Operations of Accommodation Establishments Under The New NormalDocument9 pagesHealth and Safety Guidelines Governing The Operations of Accommodation Establishments Under The New NormalRyann Zandueta ElumbaNo ratings yet
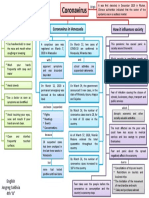
- Mapa Mental Coronavirus en InglesDocument1 pageMapa Mental Coronavirus en InglestavimayrNo ratings yet
- Ssop Covid Cleaning and Sanitizing Frequently Touched Surfaces 04232020Document3 pagesSsop Covid Cleaning and Sanitizing Frequently Touched Surfaces 04232020ING.PUICON2981No ratings yet
- 2020-05-04 The Herald Scotland PDFDocument26 pages2020-05-04 The Herald Scotland PDFpeternewhousesNo ratings yet
- Risk Managment Contingemncy Plan.Document16 pagesRisk Managment Contingemncy Plan.Ahmed HannoNo ratings yet
- Office of Collector and District Magistrate Visakhapatnamdistrict - Andhra Pradesh Travel Entry Pass - Covid-19Document2 pagesOffice of Collector and District Magistrate Visakhapatnamdistrict - Andhra Pradesh Travel Entry Pass - Covid-19devsNo ratings yet
- 2021-04-01 St. Mary's County TimesDocument32 pages2021-04-01 St. Mary's County TimesSouthern Maryland OnlineNo ratings yet
- Semester Test Writing II Jannati MaswahDocument2 pagesSemester Test Writing II Jannati MaswahJannahNo ratings yet
- PoemDocument3 pagesPoemShaina Jane CieloNo ratings yet
- Jurnal Kesmas Jumal HusniDocument9 pagesJurnal Kesmas Jumal HusniHumam_Aziz_2281No ratings yet
- Knowledge Attitudes and Practices Toward COVID-19Document9 pagesKnowledge Attitudes and Practices Toward COVID-19Nurin AdlinNo ratings yet
- Health Care in India in The Prevailing COVID-19 Pandemic ScenarioDocument6 pagesHealth Care in India in The Prevailing COVID-19 Pandemic ScenarioHimanshu ShahNo ratings yet
- Prevention and Treatment of COVID-19 in Elderly People: September 2020Document8 pagesPrevention and Treatment of COVID-19 in Elderly People: September 2020Dra. Adialys Guevara GonzalezNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Atul mishraNo ratings yet
- What Do We Want To Change?: 3.4 Criminal Record Checks For Dot Com DriversDocument5 pagesWhat Do We Want To Change?: 3.4 Criminal Record Checks For Dot Com DriversMTNo ratings yet