Professional Documents
Culture Documents
Obesity and The Brain: How Convincing Is The Addiction Model?
Obesity and The Brain: How Convincing Is The Addiction Model?
Uploaded by
Moose KeOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Obesity and The Brain: How Convincing Is The Addiction Model?
Obesity and The Brain: How Convincing Is The Addiction Model?
Uploaded by
Moose KeCopyright:
Available Formats
See discussions, stats, and author profiles for this publication at: https://www.researchgate.
net/publication/221892901
Obesity and the brain: How convincing is the addiction model?
Article in Nature Reviews Neuroscience · March 2012
DOI: 10.1038/nrn3212 · Source: PubMed
CITATIONS READS
321 4,752
3 authors, including:
Hisham Ziauddeen Sadaf Farooqi
University of Cambridge University of Cambridge
66 PUBLICATIONS 1,631 CITATIONS 340 PUBLICATIONS 32,974 CITATIONS
SEE PROFILE SEE PROFILE
Some of the authors of this publication are also working on these related projects:
Orphan receptor characterisation View project
obesity View project
All content following this page was uploaded by Hisham Ziauddeen on 17 December 2013.
The user has requested enhancement of the downloaded file.
PERSPECTIVES
Obesity and addiction: two views
OPINION
The addiction model has been applied
to obesity in a number of ways. Central to
Obesity and the brain: how each is the idea that someone can become
a ‘food addict’. What might this mean? Two
convincing is the addiction model? broad ideas have been discussed. The first
is that certain foods (those high in fat, salt
and sugar 6–8) are akin to addictive sub-
Hisham Ziauddeen, I. Sadaf Farooqi and Paul C. Fletcher stances insofar as they engage brain sys-
tems and produce behavioural adaptations
Abstract | An increasingly influential perspective conceptualizes both obesity and comparable to those engendered by drugs
overeating as a food addiction accompanied by corresponding brain changes. of abuse. This in itself is not surprising,
Because there are far-reaching implications for clinical practice and social policy if it given that current addiction models sug-
becomes widely accepted, a critical evaluation of this model is important. We gest that addictive drugs hijack the brain
examine the current evidence for the link between addiction and obesity, identifying circuitry subserving the motivation for and
enjoyment of, among other things, food9,10.
several fundamental shortcomings in the model, as well as weaknesses and
What the putatively addictive foods are has
inconsistencies in the empirical support for it from human neuroscientific research. yet to be fully defined. The case has been
made that processed foods — as opposed
Obesity, which has a profound impact on arguments for phenotypic similarity between to unrefined foods — are addictive because
personal well-being and on the demand for overeating and addiction — and questions they have nutrient profiles, such as very
health care, is at pandemic levels1. Central over whether such a model can generate real- high sugar content or combinations of high
to weight gain is the development of an istic goals for policymakers3 — one area that sugar and high fat, that are not found in
energy imbalance, a situation that arises as has not yet been critically scrutinized is the naturally occurring foods3,6. However, this
a result of complex interactions between an human neuroscience work that is often cited classification (processed versus unrefined
individual’s biology and environmental fac- in support of the addiction model and that foods) is very broad and imprecise, and it
tors1,2. Clinicians, researchers and politicians provides a pervasive framework for design would ultimately be important to specify in
recognize the importance of understanding and inference in human studies of overeating. more detail a particular substance or a level
how the brain interacts with an obesogenic In this Perspective article, we describe of nutrient (for example, a fat percentage)
environment and the corresponding poten- how the addiction model has been applied that would distinguish an addictive food
tial for neuroscience to develop our under- to obesity and overeating and critically from a non-addictive one. Sugar addic-
standing of the causes and consequences of review each of the five main lines of research tion, for example, has been demonstrated
obesity. The messages now emerging from that are usually invoked to support this in animals, but not in humans. Indeed,
the neuroscientific research community may conflation. At the outset, it is important to the validity of sugar addiction as a con-
therefore have an unprecedented impact on acknowledge that the food-addiction litera- cept that could apply to humans has been
policy development. ture has largely adopted the clinical model criticized11.
A fast-growing consensus is that obesity of addiction as defined by the DSM-IV. A second view is that food addiction is
might be understood within the same Although this model has clinical validity, in a behavioural phenotype that is seen in a
neurobiological framework as addiction and the addiction research literature it has been subgroup of people with obesity and resem-
that research, investigations, treatments supplemented, and to an extent superseded, bles drug addiction. This view draws on
and policy should be shaped accordingly 3. by powerful neurobiological models that the parallels between the DSM-IV criteria
Essentially, the view is that obesity results have decomposed the clinical syndrome in for a substance-dependence syndrome and
from an addiction to food that strongly terms of its core cognitive processes and observed patterns of overeating (TABLE 1).
resembles addiction to drugs, both behav- their possible neural substrates (BOX 1). A quantitative measure of the features of
iourally and in terms of underlying neural This approach, which is based on a growing the syndrome has recently been developed
processes. This idea is exerting a tremendous understanding of the neurobiology of in the form of the Yale Food Addiction
influence on the field of obesity research and addiction, is welcome and — as we discuss Scale (YFAS)5,12–14. However, although
has driven cogent, although unsuccessful, — may offer new ways of identifying overlap there seem to be some similarities between
arguments for the inclusion of obesity or between obesity and addiction. However, these two phenotypes, the overlap is only
overeating as a category in the fifth edition this article is primarily concerned with the partial (TABLE 1). A related, but narrower,
of the Diagnostic and Statistical Manual of existing arguments in favour of addiction as view asserts that a food-addiction pheno-
Mental Disorders (DSM‑V)4,5. Although a model for obesity, arguments that draw on type is most apparent in individuals with
there has been debate about the validity of clinical definitions. binge-eating disorder (BED), which is
NATURE REVIEWS | NEUROSCIENCE VOLUME 13 | APRIL 2012 | 279
© 2012 Macmillan Publishers Limited. All rights reserved
PERSPECTIVES
Box 1 | The addiction model for drugs of abuse
as addiction, is very subtle in most of
the obese population. Moreover, in con-
Influential models of drug dependence have divided the Diagnostic and Statistical Manual of sidering unhealthy food choices and
Mental Disorders IV (DSM-IV) behavioural syndrome into several core processes that are involved consumption, we cannot ignore social
in the transition from drug-taking to drug dependence in the subgroup of individuals who circumstances. For example, limited fam-
develop the syndrome. This transition involves a shift from voluntary drug-taking, under ventral
ily budgets direct choice to more obeso-
striatal and prefrontal control, to habitual and compulsive drug-seeking, driven predominantly by
the dorsal striatum, with loss of executive control over this behaviour75. Trait impulsivity, which
genic foods18. However, as we note above,
relates to lower levels of striatal D2 dopamine receptors (D2Rs), has been shown to increase the although obesity per se is often linked to
vulnerability to this process44,76. Lower levels of striatal D2Rs may indicate a reward-deficiency addiction, a more nuanced view suggests
state that leads to greater drug-taking in an attempt to achieve the same level of reward. The that if food addiction produces obesity, it
transition from initial impulsivity to later compulsivity has been proposed to progress through is likely to do so only in certain individu-
a three-stage model of anticipation and/or preoccupation; binge and/or intoxication; and als with disordered eating behaviours
withdrawal and/or negative effect77. Furthermore, drugs of abuse are also thought to sensitize such as BED15,19,20. Here, we consider both
the mesolimbic dopaminergic systems, leading to an enhanced salience of, and consequent perspectives.
motivation towards, drug-related cues as well as to cravings induced by such cues78. Increasing There are five key pieces of evidence
drug intake leads to neural adaptations in the striatum (further decrease of D2Rs) that promote
cited in support of the addiction model:
compulsive drug-seeking and impaired inhibitory control79, whereas adaptations in the amygdala
counter the negative states of dysphoria and withdrawal related to drug use77. These adaptations
first, a clinical overlap between obesity
serve to perpetuate the syndrome. (or, more specifically, BED) and drug
addiction15; second, evidence of shared
vulnerability to both obesity and substance
characterized by recurrent episodes (binges) A closer look at the evidence addiction; third, evidence of tolerance,
of uncontrolled, often rapid consumption of At a population level, one of the main withdrawal and compulsive food-seeking
large amounts of food, usually in isolation, drivers of the rise in prevalence of obesity in animal models of overexposure to high-
even in the absence of hunger. This eating seems to be increased availability of food, sugar and/or high-fat diets21; fourth, evi-
persists despite physical discomfort, and with a consequent imbalance between dence of lower levels of striatal dopamine
binges are associated with marked distress energy intake and expenditure1. A modest receptors (similar to findings in patients
and feelings of guilt and disgust 15. Once energy imbalance over a sustained period with drug addiction) in obese humans22; and
again, there is an important caveat: although of time can account for the observed fifth, evidence of altered brain responses to
BED is associated with obesity 16, a substantial changes in the body mass index (BMI) food-related stimuli in obese individuals
number of people who show binge-eating distributions of populations2,17. This sug- compared with non-obese controls in func-
behaviour are not obese and most obese gests that any loss of control of eating, tional imaging studies. Below, we consider
people do not have BED. which is important to the idea of obesity each of these in turn.
Table 1 | Modelling food addiction on substance dependence
DSM-IV criteria for substance dependence Proposed food-addiction equivalent* Comment
Tolerance: increasing amounts of drug are required to Tolerance: increasing amounts of food are Not a convincing equivalent to
reach intoxication required to reach satiety drug tolerance because it assumes
an equivalence between satiety
and intoxication. In addition, key
characteristics of binges are eating in
the absence of hunger and to the point
of physical discomfort (beyond satiety)
Withdrawal symptoms on drug discontinuation, Distress and dysphoria during dieting No convincing evidence of a human
including dysphoria and autonomic symptoms such as withdrawal syndrome for foods
shakes and sweats
Persistent desire for and unsuccessful attempts to cut Persistent desire for food and unsuccessful This criterion requires the application
drug use attempts to curtail the amount of food eaten of severity and impairment thresholds
to be meaningful
Larger amounts of drug taken than intended Larger amounts of food eaten than intended This criterion requires the application
of severity and impairment thresholds
to be meaningful
A great deal of time is spent on getting the drug, using A great deal of time is spent eating It is difficult to apply this criterion
the substance or recovering from it because of the easy availability of foods
in most developed societies
Important social, occupational or recreational activities Activities are given up through fear of rejection A strict equivalence would require
are given up or reduced because of substance abuse because of obesity engagement in eating to the exclusion
of other activities
Substance use is continued despite knowledge of having Overeating is maintained despite knowledge of This criterion requires the application
a persistent or recurrent physical or psychological adverse physical and psychological consequences of severity and impairment thresholds
problem caused or exacerbated by the drug caused by excessive food consumption to be meaningful
*Data in second column are taken from REFS 5,14. DSM-IV, Diagnostic and Statistical Manual of Mental Disorders IV.
280 | APRIL 2012 | VOLUME 13 www.nature.com/reviews/neuro
© 2012 Macmillan Publishers Limited. All rights reserved
PERSPECTIVES
Clinical overlap. Substance dependence is Box 2 | Towards a food-addiction model?
defined in the DSM-IV by the presence of
characteristic patterns of behaviour (TABLE 1), We have argued that attempts to develop the food-addiction model by relating obesity to the
and it has been suggested that similar patterns current clinical definition of addiction (in the Diagnostic and Statistical Manual of Mental Disorders
characterize obesity 5,6,14. Although some fea- IV (DSM-IV)) have been unconvincing. A possible future direction that we feel offers more hope of
identifying a convincing, useful clinical entity is to separate the consideration of a putative
tures (persistent desire, unsuccessful attempts
food-addiction model from both obesity and the DSM-IV criteria of substance dependence. This
to cut down and continued use despite nega- separation must be made for two reasons. First, food addiction, if it exists, may be a cause, a
tive consequences) translate reasonably well co-morbidity or possibly a consequence of obesity. Accordingly, food addiction may prevail in
from substance abuse to overeating 6,14, others non-obese and not-yet-obese individuals. Therefore, obesity, particularly when assessed solely
do not. Tolerance and withdrawal are not cross-sectionally by body-mass index (BMI), will be an unsatisfactory phenotype for food addiction.
convincingly observed in the human eating Second, the DSM-IV criteria for substance dependence translate poorly to food-related
literature14. Furthermore, food, unlike drugs, behaviours (TABLE 1) and, more importantly, these criteria aggregate core features (such as
is necessary for survival, is easy to obtain maintained use despite negative consequences) with markers of long-term use (such as tolerance)
openly and does not (generally) provoke and severity of impairment (such as time spent in acquiring substance).
social opprobrium. As a result, it is difficult to Future research into the possibility of food addiction would gain by becoming more focused and
neuroscientifically driven in the following ways:
apply criteria that relate to efforts expended
• By creating a more precise neurobehavioural definition of food addiction in which a core set of
in acquiring and consuming: such criteria are
measurable behaviours is clearly defined (inability to control consumption, increased motivation
useful in addiction to separate use from abuse to consume and persistent consumption despite negative consequences75,80). This would capture
for purposes of a DSM-IV diagnosis, but have a range of problem-eating behaviours, including, but not restricted to, binge eating.
little value with respect to food.
• By incorporating impulsivity, compulsivity and specific patterns of cognitive response as markers
As shown in TABLE 1, three criteria translate of vulnerability to and endophenotypes of the addiction81.
reasonably well from substance dependence
• By applying current models of addiction that are based on recent empirical neuroscientific work.
to overeating. Crucially, drug dependence For example, demonstrating a transition from goal-directed food-seeking under voluntary
can be diagnosed if any three criteria are met. control to compulsive habitual seeking and consumption driven by environmental cues75.
Extending this to food, an individual who ate • By relating more precise behavioural and cognitive phenotypes, rather than BMI, to
more than intended (loss of control), dieted neuroimaging findings and outcomes.
frequently and unsuccessfully (persistent
With these principles in mind, we believe that future work on food addiction could obviate the
attempts to cut down) and continued eating
problems that have so far led to an inconsistent and contradictory literature.
despite significant weight gain (continued
use despite negative consequences) would
meet the requisite criteria and be deemed a
food addict. The YFAS has applied severity Shared vulnerabilities. Another observa- Obese individuals with BED have also
and impairment thresholds that must be met tion linking obesity to drug addiction been reported to have a higher prevalence
to satisfy the criteria13. Although this cer- comes from family studies indicating of a gain-of-function allele (A118G) of the
tainly may capture a pattern of eating behav- that there may be shared genetic suscep- μ-opioid receptor (OPRM1)33 that has been
iour that is abnormal, we question whether tibilities to the two conditions. A family associated with increased sensitivity to
such an approach is sufficiently rigorous to history of alcoholism is associated with reward, greater preference for sweet and fatty
constitute good grounds for assuming an an increased risk of obesity 24, and BED foods39 and substance addiction40,41. Indeed,
addictive basis for overeating in research is associated with increased levels of sensitivity to reward is a personality trait that
studies and in clinical policy decisions. substance-use disorder in relatives25. The has been associated with obesity and drug
If we narrow our application of the con- possible contribution of specific genetic addiction. It has been argued that, as
cept to individuals with BED15, who clearly variants has been explored26–28. The most in drug addiction, obese individuals have
have abnormal eating behaviour and a widely studied of these has been the Taq1A lower reward sensitivity (the reward-
high prevalence of obesity 16, the argument minor (A1) allele of the dopamine receptor deficiency hypothesis42), resulting in a
becomes more convincing. We can recognize D2 (DRD2) gene, which has been associ- compensatory overconsumption. However,
a behavioural syndrome more convincingly ated with alcoholism29; substance-misuse the relationship between BMI and reward
like that of drug addiction, entailing loss of disorders, including cocaine30, smoking 31 sensitivity is not straightforward, and in
control of eating, escalating consumption, and opioid dependence32; and obesity 33. some people overeating occurs in the setting
compulsivity, restriction of activities, time However, many studies, including large of an apparently enhanced sensitivity to the
spent in pursuing behaviour, and possibly meta-analyses that addressed concerns hedonic aspect of food43. Reward sensitivity
consuming to ameliorate dysphoric and about population stratification and sample may be mediated by the OPRM1 and Taq1A
negative effects23. It seems that the face value size, have failed to replicate these find- allele polymorphisms mentioned above.
of the food-addiction construct is strongest ings34–36. Moreover, this polymorphism is Another personality trait, impulsivity —
when it is applied to certain (although not located 10 kilobases downstream of the the tendency to initiate behaviour without
all) individuals with BED19. Perhaps this DRD2 gene, and convincing evidence of an adequate forethought of its consequences
highlights a key limitation of the current and effect on the expression or function of the — has been identified as a risk factor for
pervasive DSM-IV-based model relating receptor is lacking, although an association substance addictions44 (BOX 1). This trait has
over-consumption to addiction. The syn- with lower levels of D2 dopamine receptors shown a modest association with the Taq1A
drome as it is defined and measured captures (D2Rs) in the striatum, measured by posi- polymorphism45,46 and has been shown to
a phenotype that may be too imprecise to tron emission tomography (PET), has been be higher in obese and BED individuals,
evaluate rigorously (BOX 2). reported37,38. correlating with food intake47–49.
NATURE REVIEWS | NEUROSCIENCE VOLUME 13 | APRIL 2012 | 281
© 2012 Macmillan Publishers Limited. All rights reserved
PERSPECTIVES
It is possible, therefore, that there are the animal) increase and remain elevated occur as a consequence of, rather than a
some shared vulnerabilities between drug 2 weeks after cessation of the diet, indicat- cause of, increased BMI. More importantly,
addiction and obesity. However, this does not ing early and persistent alteration of reward subsequent PET studies have not produced
in itself strongly support an argument that thresholds54. These findings suggest the consistent findings.
the same processes occur in each condition. development of a reward-deficiency state In studies on normal-weight participants,
similar to that seen with drugs of abuse59,60. the act of consuming food was initially shown
Evidence from animal models. By far the Reductions in presynaptic dopamine have to be associated with a reduction in dopamine
strongest evidence for a food-addiction syn- also been shown in animals on cafeteria binding in the dorsal striatum to a degree that
drome comes from animal models50. Using diets, and their dopamine activity is reduced correlated with subjectively rated meal pleas-
highly palatable foods and highly structured in response to standard chow but not palat- antness66. However, in a subsequent study,
intermittent-access regimes, it has been able food61. A complementary finding is that the presence of food in the mouth was not
possible to induce an addiction-like pheno- obesity-prone animals have been shown to associated with a significant change in striatal
type in rats. Rats with intermittent access have lower baseline levels of dopamine62,63. dopamine binding, although high levels of
to high-sugar and high-fat foods develop In summary, highly controlled condi- dietary restraint were associated with greater
escalating, binge-like eating behaviours21,51, tions for short periods of time can produce food-induced alterations in dopamine-
a phenomenon that seems to be related to sugar dependence in rats, although this is receptor availability in the dorsal striatum67.
the palatability of the foods rather than their not associated with obesity. Conversely, the Furthermore, using an elegant combination
macronutrient composition52. However, this combination of high fat and high sugar can of drug challenge (methylphenidate com-
escalation of sugar and fat intake is offset produce a compulsive overeating syndrome, pared with placebo) and stimulus presenta-
by decreases in intake of their normal food accompanied by obesity and the develop- tion (food and neutral non-food stimuli), it
supply, so although these animals become ment of a negative anhedonic state. In both was shown that food stimulation alone does
‘addicted’, they do not become obese53. situations, there is a corresponding reduc- not always have an impact on D2R striatal
A different picture is seen when fat and tion in D2Rs. Notably, researchers who have binding and that, although food stimulation
sugar are combined (as in ‘cafeteria’ diets, carried out experiments evaluating food combined with a methylphenidate challenge
in which animals are fed on foods such as addiction in animals are at pains to point out is associated with reduced dopamine binding,
bacon, cheesecake and chocolate), where- that there are important differences between the same is true for the combination of meth-
upon increased consumption and weight the effects of foods and drugs (for example, ylphenidate and a neutral non-food stimulus
gain occur in the context of eating that dopamine release in response to drugs per- (and, moreover, binding changes produced
appears more compulsive54. sists across multiple administrations, whereas by the food–methylphenidate combination
In the case of sugar ‘addiction’, enforced dopamine release induced by palatable foods do not differ significantly from those found
abstinence is associated with enhanced ceases when the food is no longer novel or with a food–placebo combination)68. In
motivation towards food55. Moreover, a the animal is no longer hungry 21). The neces- short, PET data relating to dopamine bind-
withdrawal syndrome, which can be induced sity for highly specific food presentation in ing and food consumption in normal-weight
by challenge with the opioid antagonist order to engender addictive behaviours is people are inconsistent, although this may be
naloxone or by enforced abstinence, has also an important consideration64. Given that due, in part, to the different methodological
also been demonstrated56. The features of the environments of humans are much more approaches used, such as consuming versus
the syndrome — including teeth chattering, variable than those of laboratory animals, tasting food.
forepaw tremor and head shakes — along the degree to which models of food addiction Given the variability in dopamine respon-
with their induction by administration of in animals may extend to human obesity has sivity to food stimuli in normal-weight
an opioid antagonist, indicate an opioid- yet to be explored. humans, it is perhaps unsurprising that the
mediated effect of the high-sugar diet. In picture in obesity is also inconsistent. Even in
these withdrawal states, levels of dopamine Dopamine receptor studies in human obesity. the first study, which showed reduced D2R
in the accumbens fall and acetylcholine In 2001, a landmark PET study demon- availability in morbidly obese individuals
levels rise56. However, such a withdrawal strated reduced striatal D2R binding in a (BMI range 42–60), there was considerable
syndrome has not been demonstrated with group of obese individuals22. Importantly, overlap with binding measures in healthy-
high-fat and cafeteria diets51. D2R levels were negatively correlated with weight controls22. In a more recent study 69, a
How do these behavioural changes relate BMI. The ensuing inference, that obesity is comparable striatum-based analysis showed
to altered neural substrates? In animals characterized by striatal hypofunction, is no difference in baseline dopamine-binding
binge-eating on high-sugar diets, the dopa- consistent with a reward-deficiency account measures between overweight or obese
mine release that occurs with food exposure of overeating 22. The idea is that overeating individuals and normal-weight controls
fails to habituate with loss of novelty, even in arises because there is less hedonic value (although a subsequent voxel-wise analysis
those that are sham fed (food is consumed in food, leading to compensatory over- showed a thalamic difference that extended
orally but not digested because it is removed consumption. Complementing this was the into the striatum). The negative correlation
immediately by a gastric cannula)52,57. In observation that D2R binding correlated between BMI and striatal dopamine bind-
animals binge-eating on sugar and those fed with prefrontal metabolism65, suggesting ing was not replicated. There are, of course,
a cafeteria diet, striatal D2R levels fall54,58. that striatal hypofunction is compounded numerous reasons why one might expect dif-
Moreover, in the animals of the latter group, by reduced inhibitory control. This work ferences between the original sample, which
brain self-stimulation thresholds (the mini- has been important in developing the consisted of a group of people with a BMI of
mum intensity of electrical stimulation in addiction model of obesity, although such more than 40, and the more recent one, in
the lateral hypothalamus that will maintain correlative, cross-sectional observations which mean BMI was much less. For exam-
self-administration of the stimulation by do not tell us whether the receptor changes ple, peripheral metabolic profiles might be
282 | APRIL 2012 | VOLUME 13 www.nature.com/reviews/neuro
© 2012 Macmillan Publishers Limited. All rights reserved
PERSPECTIVES
quite different, as might food intake. But the also produced conflicting results, suggest- not the case. Although studies exploring
fact remains that reduced D2R binding ing both decreases and increases in recep- brain responses to food and food-related
is not a consistent correlate of BMI or tor binding subsequent to surgery 70,71. stimuli in normal-weight people have shown
obesity and, as such, this does not, as is In short, the message emerging from largely consistent activation in reward cir-
usually claimed, provide consistent evidence PET ligand studies is rather more complex cuitry (including the amygdala, insula and
in favour of the addiction hypothesis. than is frequently asserted. Although it has striatum), the pattern emerging from studies
Perhaps the inconsistency is a conse- been shown that dopamine ligand binding comparing obese individuals and binge-eaters
quence of the phenotypic complexity of is reduced in obese individuals, this finding with controls is most remarkable for its vari-
obesity. However, a study focusing specifi- has not been replicated, and studies involv- ability and inconsistency (TABLE 2). A more
cally on differences between binge eaters ing challenges with dopamine-stimulating specific prediction, based on the reward-
and BMI-matched controls20 demonstrated drugs and food-related stimuli produce deficiency hypothesis, is an enhancement
neither a correlation between receptor complex results that do not corroborate an of anticipatory responses and a reduction of
binding and BMI nor group differences addiction model. Nor does a narrowing of consummatory responses to food rewards
that accord with an addiction model. In the phenotypic question to BED do anything in obese individuals72. However, studies that
BED, the combination of a food stimulus to clarify matters. explicitly distinguish between anticipation-
and methylphenidate was associated with and consumption-related brain activity are
reduced dopamine binding in the caudate, Functional neuroimaging. Functional neuro rare, and their results are equivocal.
whereas in non-binge-eating obese indi- imaging is an important tool in testing the TABLE 2 summarizes key findings from
viduals only the combination of a non-food addiction model, which predicts that func- functional neuroimaging studies of children,
stimulus and methylphenidate produced a tional responses to foods and food-related adolescents and adults that explored brain
significant change. Other studies examin- stimuli in key reward-related brain regions responses to food-related stimuli (typically
ing the impact of bariatric surgery have should be consistently perturbed. This is images) and to anticipation and consumption
Table 2 | Summary of the findings of studies exploring altered brain responses in people with obesity or altered eating patterns
Brain region Response to cues signalling
Response to presentation of food imminent presentation of food/
images juice reward (anticipation) Response to consumption of reward
Obese BED BMI FA Obese BED BMI FA Obese BED BMI FA
Regions associated with the reward circuitry
Striatum 2 ↑83,84, 2 ↔87,88 1 ↑89, NA 1 ↑93, 1 ↔94 NA NA 1 ↑95 5 ↔93,94,96–98 1 ↓99, 1 ↓94 1 ↔95
1 ↓85, 1 ↓90, 1 ↔100
1 ↔86 3 ↔85,91,92
Midbrain 4 ↔83–86 2 ↔87,88 5 ↔85,89–92 NA 2 ↔93,94 NA NA 1 ↔95 1 ↑96, 2 ↔99,100 1 ↔94 1 ↔95
4 ↔93,94,97,98
PFC (orbital) 1 ↑86, 1 ↑87, 3 ↑90–92, NA 2 ↔93,94 NA NA 1 ↑95 1 ↑96, 1 ↓99, 1 ↔94 1 ↓95
3 ↔83–85 1 ↔88 1 ↓89, 4 ↔93,94,97,98 1 ↔100
1 ↔85
PFC (lateral) 3 ↑84–86, 2 ↔87,88 1 ↑85, NA 1 ↑93, 1 ↔94 1 ↑101 NA 1 ↔95 1 ↑93, 2 ↔99,100 1 ↔94 1 ↔95
1 ↔83 1 ↓92, 2 ↓97,98,
3 ↔89–91 2 ↔94,96
PFC (medial) 2 ↑84,86, 1 ↑87, 1 ↓92, NA 1 ↑94, 1 ↔93 NA NA 1 ↑95 5 ↔93,94,96–98 2 ↔99,100 1 ↔94 1 ↔95
1 ↓85, 1 ↔88 4 ↔85,89–91
1 ↔83
Amygdala 4 ↔83–86 2 ↔87,88 5 ↔85,89–92 NA 2 ↔93,94 NA NA 1 ↑95 1 ↑93, 1 ↓99, 1 ↔94 1 ↔95
4 ↔94,96–98 1 ↔100
Gustatory 1 ↑83, 1 ↑87, 3 ↑89,90,92, NA 1 ↑94, 1 ↔93 NA NA 1 ↔95 3 ↑93,94,96, 2 ↓99,100 1 ↔94 1 ↔95
cortex (AI/FO) 3 ↔84–86 1 ↓88 2 ↔85,91 2 ↔97,98
Hippocampus/ 2 ↑84,86, 2 ↔87,88 1 ↓85, NA 1 ↑93, 1 ↔94 NA NA 1 ↔95 5 ↔93,94,96–98 2 ↔99,100 1 ↔94 1 ↔95
PHG 1 ↓85, 4 ↔89–92
1 ↔83
Brain regions not associated with the reward circuitry
Thalamus 1 ↓85, 2 ↔87,88 5 ↔85,89–92 NA 2 ↔93,94 NA NA 1 ↔95 5 ↔93,94,96–98 2 ↔99,100 1 ↔94 1 ↔95
3 ↔83,84,86
Rolandic 4 ↔83–86 2 ↔87,88 5 ↔85,89–92 NA 2 ↑93,94 NA NA 1 ↔95 2 ↑93,94, 2 ↔99,100 1 ↔94 1 ↔95
operculum 3 ↔96–98
The table shows responses that were elevated (↑) or reduced (↓) in groups of obese individuals or those with binge-eating disorder (BED) relative to controls.
No group difference is signified by ‘↔’. Numbers before the arrows indicate the number of studies. The table also shows studies reporting positive (↑), negative (↓)
or no (↔) reported group difference between neural activity and body mass index (BMI) or food addiction (FA) scores. AI, anterior insula; FO, frontal operculum;
NA, no reports available (at the time of writing); PFC, prefrontal cortex; PHG, parahippocampal gyrus.
NATURE REVIEWS | NEUROSCIENCE VOLUME 13 | APRIL 2012 | 283
© 2012 Macmillan Publishers Limited. All rights reserved
PERSPECTIVES
Food environment
Energy
expenditure
Appetite
• Availability and satiety
• Palatability
• Energy density • Impaired satiety
• Fat-free mass
• Portion size signalling
• Physical activity
• Insensitivity to
hunger and fullness
• Eating rate
Physical • Food access
environment • Access to physical Energy balance
activity
• Early developmental
• Advertising programming
• TV watching • Genetic and epigenetic
• Parental and societal • Reward sensitivity factors
influences • Impulsivity
• Media • Abnormal eating Individual
• Food addiction predispositions
Environmental
influences
Personality and
reward circuitry
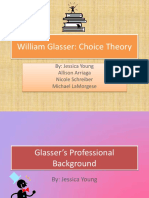
Figure 1 | Mediators of energy balance and body weight. The outer require further exploration and refinement. The data on which the figure
Nature Reviews | Neuroscience
ring represents the major classes of mediators, the inner ring some of the is based come from the Obesity Systems Map introduced by the UK
individual mediators in each class. We suggest that food addiction is one Foresight programme 2007, a multidisciplinary effort to plan the
of many factors in a more complex model of the obesity epidemic that UK response to obesity82.
of actual food stimuli (typically milkshake). Functional neuroimaging allows us to overeating, let alone support for the addic-
A number of approaches have been used to measure not only regional responses but tion model? We find it hard to believe that
explore obesity and altered eating patterns. also inter-regional relationships. Alterations such circuitry is unaltered. One possibility
Case–control studies comparing obese indi- in these system-wide patterns have been is that overeating and its consequences are
viduals with normal-weight controls are typi- assessed in association with external food just too complex to expect consistency when
cal and are complemented by analyses of the sensitivity — the extent to which external individuals are grouped simply according to
extent to which activity correlates with BMI food cues evoke the desire to eat 73 — and BMI, or to binge-eating or food-addiction
and, in one study, with food-addiction score. obesity 74. Although intriguing observations scores. Given that obesity and binge eating
Studies of binge eating (with bulimia nervosa have been made, particularly with respect are complex phenotypes emerging for a
or BED) have also been carried out. The to the regions described above (which host of genetic and environmental reasons,
findings shown in TABLE 2 indicate a striking constitute the ‘reward circuitry’), it is too in failing to account for this complexity
lack of consistency across studies. soon to judge whether connectivity studies our capacity to identify group or factor-
Of course, there are differences in tasks will show a consistency that eludes regional related differences is markedly reduced.
and stimuli across the studies and there are measures. Furthermore, both of these phenotypes
age and gender differences across the groups There are two clear messages emerging have often been measured cross-sectionally,
studied. But, given that the striatum, mid- from the functional neuroimaging literature without taking into account the natural his-
brain and prefrontal cortex are core compo- on obesity and overeating. First, a growing tory of these conditions (BOX 2). We clearly
nents of the dopaminergic-reinforcement body of work has not supported any single need more precise behavioural, temporal,
circuitry, the lack of consistent findings across view of obesity and overeating. Second, metabolic, genetic and cognitive profiling in
a large set of studies militates strongly against even when analysis is confined to sub- such investigations. Moreover, the growing
the addiction model. If we consider the region groups showing binge-eating behaviour, sophistication of cognitive neuroscientific
of the anterior insula and frontal operculum there has been no convincing or consist- models of addictive behaviours points
that is sometimes referred to as the gusta- ent pattern of abnormal responding in the to crucial process-specific alterations in
tory cortex, the inconsistency remains. Nor reward circuitry. If the addiction model regional responding. Dissecting out these
is observation of responses in the amygdala of overeating has currency beyond phe- processes will require more complex task-
helpful in distinguishing obese individuals notypic similarities (which, as we argue dependent measurements than are typically
from normal-weight controls. The over- above, are themselves weak), we would applied in overeating and obese individuals.
whelming message emerging from TABLE 2, expect functional neuroimaging studies to In the future, those imaging studies that
even allowing for technical and participant identify core similarities. Why have they attempt to distinguish subtle processes and
differences, is that functional neuroimaging failed to provide any consistent insight into simultaneously take into account individual
does not support the addiction model. the behaviour of brain reward circuitry in variability 27 will prove useful and important.
284 | APRIL 2012 | VOLUME 13 www.nature.com/reviews/neuro
© 2012 Macmillan Publishers Limited. All rights reserved
PERSPECTIVES
Conclusions and future directions Hisham Ziauddeen and Paul C. Fletcher are in the 25. Lilenfeld, L. R. R., Ringham, R., Kalarchian, M. A. &
Department of Psychiatry, University of Cambridge, Marcus, M. D. A family history study of binge-eating
The view that overeating and obesity are disorder. Compr. Psychiatry 49, 247–254 (2008).
Herchel Smith Building, Addenbrooke’s Hospital,
directly related to addiction has provided Cambridge CB2 0SZ, UK; and at the Cambridgeshire
26. Stice, E., Spoor, S., Bohon, C. & Small, D. M.
Relation between obesity and blunted striatal
impetus to a series of elegant studies testing and Peterborough NHS Foundation Trust, Fulbourn response to food is moderated by TaqIA A1 allele.
this proposed link. Somehow, the view has Hospital, Cambridge CB21 5EF, UK. Science 322, 449–452 (2008).
27. Stice, E., Yokum, S., Bohon, C., Marti, N. & Smolen, A.
emerged that, overall, these studies sup- Hisham Ziauddeen and I. Sadaf Farooqi are at the Reward circuitry responsivity to food predicts
port the link. We challenge this view and University of Cambridge Metabolic Research future increases in body mass: moderating effects
of DRD2 and DRD4. Neuroimage 50, 1618–1625
argue that the work tells us three important Laboratories, Institute of Metabolic Science,
(2010).
Addenbrooke’s Hospital, Cambridge CB2 0QQ, UK.
things. First, the vast majority of overweight 28. Felsted, J. A., Ren, X., Chouinard-Decorte, F. &
Correspondence to P.C.F. Small, D. M. Genetically determined differences in
individuals have not shown a convincing brain response to a primary food reward. J. Neurosci.
e-mail: pcf22@cam.ac.uk
behavioural or neurobiological profile that 30, 2428–2432 (2011).
doi:10.1038/nrn3212 29. Munafo, M. R., Matheson, I. J. & Flint, J. Association
resembles addiction. Indeed, the enormous Published online 14 March 2012 of the DRD2 gene Taq1A polymorphism and
inconsistency emerging from a review of alcoholism: a meta-analysis of case-control studies
1. Swinburn, B. A. et al. The global obesity pandemic: and evidence of publication bias. Mol. Psychiatry 12,
the neuroimaging literature tells us that shaped by global drivers and local environments. 454–461 (2007).
in this highly heterogenous disorder, the Lancet 378, 804–814 (2011). 30. Noble, E. P. et al. Allelic association of the D2
2. Hall, K. D. et al. Quantification of the effect of energy dopamine receptor gene with cocaine dependence.
application of a single model is likely to be imbalance on bodyweight. Lancet 378, 826–837 Drug Alcohol Depend. 33, 271–285 (1993).
more of a hindrance than a help to future (2011). 31. Zuo, Y. et al. DRD2‑related TaqIA polymorphism
3. Gearhardt, A. N., Grilo, C. M., Dileone, R. J., modulates motivation to smoke. Nicotine Tob. Res. 11,
research. Second, even when we refine the Brownell, K. D. & Potenza, M. N. Can food be 1321–1329 (2009).
phenotype to characterize individuals who addictive? Public health and policy implications. 32. Doehring, A. et al. Genetic variants altering dopamine
Addiction 106, 1208–1212 (2011). D2 receptor expression or function modulate the risk
show obesity caused by BED, the evidence 4. Devlin, M. J. Is there a place for obesity in DSM‑V? of opiate addiction and the dosage requirements of
for an overlap with addiction is inconsist- Int. J. Eat. Disord. 40, S83–S88 (2007). methadone substitution. Pharmacogenet. Genomics
5. Volkow, N. D. & O’Brien, C. P. Issues for DSM‑V: 19, 407–414 (2009).
ent and weak. Third, given the absence of should obesity be included as a brain disorder? 33. Davis, C. A. et al. Dopamine for “wanting” and opioids
good evidence, the ubiquitous influence Am. J. Psychiatry 164, 708–710 (2007). for “liking”: a comparison of obese adults with and
6. Ifland, J. R. et al. Refined food addiction: a classic without binge eating. Obesity 17, 1220–1225
of the addiction model of overeating and substance use disorder. Med. Hypotheses 72, (2009).
consequent obesity is remarkable. Now is a 518–526 (2009). 34. Smith, L., Watson, M., Gates, S., Ball, D. & Foxcroft, D.
7. Cocores, J. A. & Gold, M. S. The Salted Food Addiction Meta-analysis of the association of the Taq1A
good time to question it and to acknowledge Hypothesis may explain overeating and the obesity polymorphism with the risk of alcohol dependency:
that adherence to it in the face of data that epidemic. Med. Hypotheses 73, 892–899 (2009). a HuGE gene-disease association review.
8. Volkow, N. D., Wang, G.‑J. & Baler, R. D. Am. J. Epidemiol. 167, 125–138 (2008).
do not fit will lead to research that is too Reward, dopamine and the control of food intake: 35. Munafo, M. R., Timpson, N. J., David, S. P., Ebrahim, S.
narrowly focused and, ultimately, mislead- implications for obesity. Trends Cogn. Sci. 15, 37–46 & Lawlor, D. A. Association of the DRD2 gene Taq1A
(2011). polymorphism and smoking behavior: a meta-analysis
ing. Given the attention that is rightly paid 9. Volkow, N. D. & Wise, R. A. How can drug addiction and new data. Nicotine Tob. Res. 11, 64–76
to potential insights offered by neurosci- help us understand obesity? Nature Neurosci. 8, (2009).
555–560 (2005). 36. Fernandez-Castillo, N. et al. Association study
ence, there is an associated danger that 10. Kelley, A. E. & Berridge, K. C. The neuroscience of between the DAT1, DBH and DRD2 genes and cocaine
clinical and policy recommendations will natural rewards: relevance to addictive drugs. dependence in a Spanish sample. Psychiatr. Genet.
J. Neurosci. 22, 3306–3311 (2002). 20, 317–320 (2010).
be misguided. We suggest that alternative 11. Benton, D. The plausibility of sugar addiction and its 37. Pohjalainen, T. et al. The A1 allele of the human D2
approaches to exploring the brain’s con- role in obesity and eating disorders. Clin. Nutr. 29, dopamine receptor gene predicts low D2 receptor
288–303 (2010). availability in healthy volunteers. Mol. Psychiatry 3,
tributions to obesity be explored. Central 12. American Psychiatric Association. Diagnostic and 256–260 (1998).
to these is an explicit acknowledgement of Statistical Manual of Mental Disorders 4th edn 38. Jonsson, E. G. et al. Polymorphisms in the dopamine
(American Psychiatric Association, Washington, DC, D2 receptor gene and their relationships to striatal
the enormous heterogeneity of the condi- 2000). dopamine receptor density of healthy volunteers.
tion, which requires further exploration 13. Gearhardt, A. N., Corbin, W. R. & Brownell, K. D. Mol. Psychiatry 4, 290–296 (1999).
Preliminary validation of the Yale Food Addiction 39. Davis, C. et al. Opiates, overeating and obesity: a
and characterization. This characterization Scale. Appetite 52, 430–436 (2009). psychogenetic analysis. Int. J. Obes. 35, 1347–1354
will, we anticipate, entail the use of cogni- 14. Gearhardt, A. N., Corbin, W. R. & Brownell, K. D. (2011).
Food addiction: an examination of the diagnostic 40. Miranda, R. et al. Initial evidence of an association
tive neuroscience to provide useful pheno- criteria for dependence. J. Addict. Med. 3, 1–7 between OPRM1 and adolescent alcohol misuse.
typic markers of the numerous pathways (2009). Alcohol. Clin. Exp. Res. 34, 112–122 (2010).
15. Davis, C. & Carter, J. C. Compulsive overeating as an 41. Ramchandani, V. A. et al. A genetic determinant of
to obesity. addiction disorder. A review of theory and evidence. the striatal dopamine response to alcohol in men.
Our intention in this Perspective has Appetite 53, 1–8 (2009). Mol. Psychiatry 16, 809–817 (2011).
16. Striegel-Moore, R. H. & Franko, D. L. Epidemiology 42. Comings, D. E. & Blum, K. Reward deficiency
been to urge caution against the hasty adop- of binge eating disorder. Int. J. Eat. Disord. 34, syndrome: genetic aspects of behavioral disorders.
tion of a model with limited applicability and S19–S29 (2003). Prog. Brain Res. 126, 325–341 (2000).
17. O’Rahilly, S. Human genetics illuminates the paths to 43. Davis, C. & Fox, J. Sensitivity to reward and body
supporting evidence. We do not deny that metabolic disease. Nature 462, 307–314 (2009). mass index (BMI): evidence for a non-linear
there may well be a place for an addiction 18. Drewnowski, A. Obesity, diets, and social inequalities. relationship. Appetite 50, 43–49 (2008).
Nutr. Rev. 67, S36–S39 (2009). 44. Verdejo-Garcia, A., Lawrence, A. J. & Clark, L.
model in the understanding of overeating 19. Davis, C. et al. Evidence that ‘food addiction’ is a valid Impulsivity as a vulnerability marker for
and the spectrum of the obesity syndrome phenotype of obesity. Appetite 57, 711–717 (2011). substance-use disorders: review of findings from
20. Wang, G. J. et al. Enhanced striatal dopamine release high-risk research, problem gamblers and genetic
(FIG 1). However, successful development during food stimulation in binge eating disorder. association studies. Neurosci. Biobehav. Rev. 32,
of such a model will demand a progres- Obesity 19, 1601–1608 (2011). 777–810 (2008).
21. Avena, N. M., Rada, P. & Hoebel, B. G. Evidence for 45. Limosin, F. et al. Impulsiveness as the intermediate
sion beyond existing clinical definitions of sugar addiction: behavioral and neurochemical link between the dopamine receptor D2 gene and
addiction to ideas that are guided by the effects of intermittent, excessive sugar intake. alcohol dependence. Psychiatr. Genet. 13, 127–129
Neurosci. Biobehav. Rev. 32, 20–39 (2008). (2003).
developing neuroscientific literature (BOX 2). 22. Wang, G. J. et al. Brain dopamine and obesity. 46. Eisenberg, D. T. et al. Examining impulsivity as an
It will also demand sophisticated and precise Lancet 357, 354–357 (2001). endophenotype using a behavioral approach: a DRD2
23. Cassin, S. E. & von Ranson, K. M. Is binge eating TaqI A and DRD4 48‑bp VNTR association study.
delineations of altered eating behaviour in experienced as an addiction? Appetite 49, 687–690 Behav. Brain Funct. 3, 2 (2007).
humans, and phenotypic markers that go (2007). 47. Guerrieri, R. et al. The influence of trait and
24. Grucza, R. A. et al. The emerging link between induced state impulsivity on food intake in
well beyond simple cross-sectional measures alcoholism risk and obesity in the United States. normal‑weight healthy women. Appetite 49, 66–73
such as BMI. Arch. Gen. Psychiatry 67, 1301–1308 (2010). (2007).
NATURE REVIEWS | NEUROSCIENCE VOLUME 13 | APRIL 2012 | 285
© 2012 Macmillan Publishers Limited. All rights reserved
PERSPECTIVES
48. Galanti, K., Gluck, M. E. & Geliebter, A. Test meal 68. Volkow, N. D. et al. “Nonhedonic” food motivation in 90. Yokum, S., Ng, J. & Stice, E. Attentional bias to food
intake in obese binge eaters in relation to impulsivity humans involves dopamine in the dorsal striatum and images associated with elevated weight and future
and compulsivity. Int. J. Eat. Disord. 40, 727–732 methylphenidate amplifies this effect. Synapse 44, weight gain: an FMRI study. Obesity 19, 1775–1783
(2007). 175–180 (2002). (2011).
49. Davis, C. et al. Personality and eating behaviors: 69. Haltia, L. T. et al. Effects of intravenous glucose on 91. Killgore, W. D. S. & Yurgelun-Todd, D. A. Body mass
a case–control study of binge eating disorder. dopaminergic function in the human brain in vivo. predicts orbitofrontal activity during visual
Int. J. Eat. Disord. 41, 243–250 (2008). Synapse 61, 748–756 (2007). presentations of high-calorie foods. Neuroreport 16,
50. Kenny, P. J. Common cellular and molecular 70. Steele, K. E. et al. Alterations of central dopamine 859–863 (2005).
mechanisms in obesity and drug addiction. receptors before and after gastric bypass surgery. 92. Batterink, L., Yokum, S. & Stice, E. Body mass
Nature Rev. Neurosci. 12, 638–651 (2011). Obes. Surg. 20, 369–374 (2010). correlates inversely with inhibitory control in response
51. Bocarsly, M. E., Berner, L. A., Hoebel, B. G. & 71. Dunn, J. P. et al. Decreased dopamine type 2 receptor to food among adolescent girls: an fMRI study.
Avena, N. M. Rats that binge eat fat-rich food do not availability after bariatric surgery: preliminary Neuroimage 52, 1696–1703 (2010).
show somatic signs or anxiety associated with opiate- findings. Brain Res. 1350, 123–130 (2010). 93. Ng, J., Stice, E., Yokum, S. & Bohon, C. An fMRI study
like withdrawal: implications for nutrient-specific food 72. Volkow, N. D., Wang, G. J., Fowler, J. S. & Tomasi, D. of obesity, food reward, and perceived caloric density.
addiction behaviors. Physiol. Behav. 104, 865–872 Addiction circuitry in the human brain. Annu. Rev. Does a low-fat label make food less appealing?
(2011). Pharmacol. Toxicol. 52, 321–336 (2012). Appetite 57, 65–72 (2011).
52. Avena, N. M., Rada, P., Moise, N. & Hoebel, B. G. 73. Passamonti, L. et al. Personality predicts the brain’s 94. Stice, E., Spoor, S., Bohon, C., Veldhuizen, M. G. &
Sucrose sham feeding on a binge schedule releases response to viewing appetizing foods: the neural basis Small, D. M. Relation of reward from food intake and
accumbens dopamine repeatedly and eliminates the of a risk factor for overeating. J. Neurosci. 29, 43–51 anticipated food intake to obesity: a functional
acetylcholine satiety response. Neuroscience 139, (2009). magnetic resonance imaging study. J. Abnorm.
813–820 (2006). 74. Kullmann, S. et al. The obese brain: association of Psychol. 117, 924–935 (2008).
53. Avena, N. M., Rada, P. & Hoebel, B. G. Sugar and fat body mass index and insulin sensitivity with resting 95. Gearhardt, A. N. et al. Neural correlates of food
bingeing have notable differences in addictive-like state network functional connectivity. Hum. Brain addiction. Arch. Gen. Psychiatry 68, 808–816 (2011).
behavior. J. Nutr. 139, 623–628 (2009). Mapp. 21 Apr 2011 (doi:10.1002/hbm.21268). 96. DelParigi, A., Chen, K., Salbe, A. D., Reiman, E. M. &
54. Johnson, P. M. & Kenny, P. J. Dopamine D2 receptors 75. Everitt, B. J. et al. Review. Neural mechanisms Tataranni, P. A. Sensory experience of food and
in addiction-like reward dysfunction and compulsive underlying the vulnerability to develop compulsive obesity: a positron emission tomography study of the
eating in obese rats. Nature Neurosci. 13, 635–641 drug-seeking habits and addiction. Phil. Trans. R. Soc. B brain regions affected by tasting a liquid meal after a
(2010). 363, 3125–3135 (2008). prolonged fast. Neuroimage 24, 436–443 (2005).
55. Avena, N. M., Long, K. A. & Hoebel, B. G. 76. Dalley, J. W. et al. Nucleus accumbens D2/3 receptors 97. Le, D. S. et al. Less activation of the left dorsolateral
Sugar-dependent rats show enhanced responding predict trait impulsivity and cocaine reinforcement. prefrontal cortex in response to a meal: a feature of
for sugar after abstinence: evidence of a sugar Science 315, 1267–1270 (2007). obesity. Am. J. Clin. Nutr. 84, 725–731 (2006).
deprivation effect. Physiol. Behav. 84, 359–362 77. Koob, G. F. & Le Moal, M. Review. Neurobiological 98. Le, D. S. et al. Less activation in the left dorsolateral
(2005). mechanisms for opponent motivational processes in prefrontal cortex in the reanalysis of the response to a
56. Colantuoni, C. et al. Evidence that intermittent, addiction. Phil. Trans. R. Soc. B 363, 3113–3123 meal in obese than in lean women and its association
excessive sugar intake causes endogenous opioid (2008). with successful weight loss. Am. J. Clin. Nutr. 86,
dependence. Obes Res. 10, 478–488 (2002). 78. Robinson, T. E. & Berridge, K. C. The neural basis of 573–579 (2007).
57. Rada, P., Avena, N. M. & Hoebel, B. G. Daily bingeing drug craving: an incentive-sensitization theory of 99. Frank, G. K. W., Reynolds, J. R., Shott, M. E. &
on sugar repeatedly releases dopamine in the addiction. Brain Res. Brain Res. Rev. 18, 247–291 O’Reilly, R. C. Altered temporal difference learning in
accumbens shell. Neuroscience 134, 737–744 (1993). bulimia nervosa. Biol. Psychiatry 70, 728–735
(2005). 79. Volkow, N. D. et al. Low level of brain dopamine D2 (2011).
58. Colantuoni, C. et al. Excessive sugar intake alters receptors in methamphetamine abusers: association 100. Bohon, C. & Stice, E. Reward abnormalities among
binding to dopamine and mu-opioid receptors in the with metabolism in the orbitofrontal cortex. women with full and subthreshold bulimia nervosa:
brain. Neuroreport 12, 3549–3552 (2001). Am. J. Psychiatry 158, 2015–2021 (2001). a functional magnetic resonance imaging study.
59. Ahmed, S. H., Kenny, P. J., Koob, G. F. & Markou, A. 80. Deroche-Gamonet, V., Belin, D. & Piazza, P. V. Int. J. Eat. Disord. 44, 585–595 (2010).
Neurobiological evidence for hedonic allostasis Evidence for addiction-like behavior in the rat. 101. Karhunen, L. J. et al. Regional cerebral blood flow
associated with escalating cocaine use. Nature Science 305, 1014–1017 (2004). during exposure to food in obese binge eating women.
Neurosci. 5, 625–626 (2002). 81. Robbins, T. W., Gillan, C. M., Smith, D. G., de Wit, S. & Psychiatry Res. 99, 29–42 (2000).
60. Kenny, P. J., Chen, S. A., Kitamura, O., Markou, A. & Ersche, K. D. Neurocognitive endophenotypes of
Koob, G. F. Conditioned withdrawal drives heroin impulsivity and compulsivity: towards dimensional Acknowledgements
consumption and decreases reward sensitivity. psychiatry. Trends Cogn. Sci. 16, 81–91 (2012). We would like to thank B. Everitt for his comments, particu‑
J. Neurosci. 26, 5894–5900 (2006). 82. Vandenbroeck, P., Goossens, J. & Clemens, M. larly on Box 2. H.Z. is jointly funded by the Wellcome Trust
61. Geiger, B. M. et al. Deficits of mesolimbic dopamine Tackling Obesities: Future Choices — Obesity System and GlaxoSmithKline. I.S.F. and P.C.F. are supported by the
neurotransmission in rat dietary obesity. Neuroscience Atlas (Government Office for Science, UK, 2007). Bernard Wolfe Health Neuroscience Fund. H.Z., I.S.F. and
159, 1193–1199 (2009). 83. Rothemund, Y. et al. Differential activation of the P.C.F. are also supported by the Wellcome Trust, MRC
62. Geiger, B. M. et al. Evidence for defective mesolimbic dorsal striatum by high-calorie visual food stimuli in (Medical Research Council) Centre for Obesity and Related
dopamine exocytosis in obesity-prone rats. FASEB J. obese individuals. Neuroimage 37, 410–421 (2007). Diseases, and the UK National Institute for Health Research
22, 2740–2746 (2008). 84. Martin, L. E. et al. Neural mechanisms associated with (NIHR) Cambridge Biomedical Research Centre. This work
63. Rada, P., Bocarsly, M. E., Barson, J. R., Hoebel, B. G. food motivation in obese and healthy weight adults. was carried out at the Institute of Metabolic Science and the
& Leibowitz, S. F. Reduced accumbens dopamine in Obesity 18, 254–260 (2010). We l l c o m e – M R C - f u n d e d B e h av i o u ra l a n d C l i n i c a l
Sprague-Dawley rats prone to overeating a fat-rich 85. Davids, S. et al. Increased dorsolateral prefrontal Neuroscience Institute. It was inspired by discussions with
diet. Physiol. Behav. 101, 394–400 (2010). cortex activation in obese children during observation fellow members of the Behaviour and Health Research Unit.
64. Corwin, R. L. & Grigson, P. S. Symposium overview- of food stimuli. Int. J. Obes. 34, 94–104 (2010).
food addiction: fact or fiction? J. Nutr. 139, 617–619 86. Bruce, A. S. et al. Obese children show hyperactivation Competing interests statement
(2009). to food pictures in brain networks linked to motivation, The authors declare competing financial interests; see Web
65. Volkow, N. D. et al. Low dopamine striatal D2 reward and cognitive control. Int. J. Obes 34, version for details.
receptors are associated with prefrontal metabolism 1494–1500 (2010).
in obese subjects: possible contributing factors. 87. Schienle, A., Schäfer, A., Hermann, A. & Vaitl, D. DATABASES
Neuroimage 42, 1537–1543 (2008). Binge-eating disorder: reward sensitivity and brain Pathway Interaction Database: http://pid.nci.nih.gov
66. Small, D. M., Jones-Gotman, M. & Dagher, A. activation to images of food. Biol. Psychiatry 65,
Feeding-induced dopamine release in dorsal striatum 654–661 (2009). FURTHER INFORMATION
correlates with meal pleasantness ratings in healthy 88. Brooks, S. J. et al. Differential neural responses to Behaviour and Health Research Unit:
human volunteers. Neuroimage 19, 1709–1715 food images in women with bulimia versus anorexia http://www.bhru.iph.cam.ac.uk
(2003). nervosa. PLoS ONE 6, e22259 (2011). Metabolic Research Laboratories:
67. Volkow, N. D. et al. Brain dopamine is associated with 89. Stice, E., Yokum, S., Blum, K. & Bohon, C. Weight gain http://www.mrl.ims.cam.ac.uk
eating behaviors in humans. Int. J. Eat. Disord. 33, is associated with reduced striatal response to ALL LINKS ARE ACTIVE IN THE ONLINE PDF
136–142 (2003). palatable food. J. Neurosci. 30, 13105–13109 (2010).
286 | APRIL 2012 | VOLUME 13 www.nature.com/reviews/neuro
View publication stats
© 2012 Macmillan Publishers Limited. All rights reserved
You might also like
- Language, Literacy and Early Childhood Education 3... - (4 Oral Language Perspectives and Phases) Chapter 2Document21 pagesLanguage, Literacy and Early Childhood Education 3... - (4 Oral Language Perspectives and Phases) Chapter 2Cecilia ElliottNo ratings yet
- Food AdictionDocument10 pagesFood AdictionVictoria ZorzopulosNo ratings yet
- ADICCIÓN Comida, ConceptoDocument8 pagesADICCIÓN Comida, Conceptoadriannn017No ratings yet
- Neurologic Craving of Carbohydrates PDFDocument5 pagesNeurologic Craving of Carbohydrates PDFirfan fandiNo ratings yet
- Food Addiction Eating Addiction and Eating DisordersDocument10 pagesFood Addiction Eating Addiction and Eating DisordersWilmer PeñaNo ratings yet
- The Plausibility of Sugar Addiction and Its Role in Obesity and Eating Disorders - Benton PDFDocument16 pagesThe Plausibility of Sugar Addiction and Its Role in Obesity and Eating Disorders - Benton PDFBetinna BoladoNo ratings yet
- A Critical Examination of The Practical Implications Derived From The Food Addiction ConceptDocument7 pagesA Critical Examination of The Practical Implications Derived From The Food Addiction Conceptadriannn017No ratings yet
- Nu 12113564Document24 pagesNu 12113564Laura CanoNo ratings yet
- Vella-Pai2017 Article ANarrativeReviewOfPotentialTreDocument7 pagesVella-Pai2017 Article ANarrativeReviewOfPotentialTreAisah indrawatiNo ratings yet
- Addiction and The Brain Development Not DiseaseDocument13 pagesAddiction and The Brain Development Not DiseaseGayneOrtegaNo ratings yet
- Ijerph 18 09791Document10 pagesIjerph 18 09791Elisa RodríguezNo ratings yet
- Lewis, 2017Document12 pagesLewis, 2017Angela JimenezNo ratings yet
- Implications of Ultra-Processed Food AddictionDocument6 pagesImplications of Ultra-Processed Food Addiction6cmrd8488pNo ratings yet
- Nutrition Knowledge Assessment Studies in Adults: A Systematic ReviewDocument14 pagesNutrition Knowledge Assessment Studies in Adults: A Systematic ReviewPablo CamposNo ratings yet
- 10 1056@NEJMra1602872 PDFDocument10 pages10 1056@NEJMra1602872 PDFBeny RiliantoNo ratings yet
- Neuroethical Issues in Pharmacological Cognitive EnhancementDocument17 pagesNeuroethical Issues in Pharmacological Cognitive EnhancementManuela Flores InostrozaNo ratings yet
- Adhrnc FinalDocument22 pagesAdhrnc FinalMary Ann OquendoNo ratings yet
- Jurnal Pendukung 2Document13 pagesJurnal Pendukung 2Eko PrasNo ratings yet
- Food Addiction. Food On The Brain: November 2012Document5 pagesFood Addiction. Food On The Brain: November 2012Eddy JayNo ratings yet
- Theoretical, Practical, and Social Issues in Behavioral Treatments of ObesityDocument23 pagesTheoretical, Practical, and Social Issues in Behavioral Treatments of ObesityJoão P. RibeiroNo ratings yet
- Probiotic Food Consumption Is Associated With Lower Severity and P - 2019 - NutrDocument6 pagesProbiotic Food Consumption Is Associated With Lower Severity and P - 2019 - NutrRinaNo ratings yet
- Leitura Extensão 10-09-19 PDFDocument16 pagesLeitura Extensão 10-09-19 PDFJuliete TavaresNo ratings yet
- Eating Reg SDT ArticleDocument16 pagesEating Reg SDT ArticleDidar YANASNo ratings yet
- Am J Psychiatry 2013 May 170-5 - 6 EnigmaticDocument8 pagesAm J Psychiatry 2013 May 170-5 - 6 EnigmaticKarla MenaresNo ratings yet
- Seminar: Jonathan Posner, Guilherme V Polanczyk, Edmund Sonuga-BarkeDocument13 pagesSeminar: Jonathan Posner, Guilherme V Polanczyk, Edmund Sonuga-BarkeCristinaNo ratings yet
- Effective Strategies in Ending Weight Stigma in HealthcareDocument16 pagesEffective Strategies in Ending Weight Stigma in HealthcareClaudia Capelli AspillagaNo ratings yet
- Alimentos Hormonales, Experienciales y NeuronalesDocument7 pagesAlimentos Hormonales, Experienciales y NeuronalesJuanNo ratings yet
- Sugar Addiction The State of The ScienceDocument16 pagesSugar Addiction The State of The Sciencepsic.tatianebezerraNo ratings yet
- Cambios Neurobiologicos y Consumo. NjemDocument10 pagesCambios Neurobiologicos y Consumo. NjemLala FolmerNo ratings yet
- Food Reward SystemDocument12 pagesFood Reward SystemCamilla MendesNo ratings yet
- Review Article Relationships Between Intuitive Eating and Health Indicators Literature ReviewDocument10 pagesReview Article Relationships Between Intuitive Eating and Health Indicators Literature ReviewYasmim CronembergerNo ratings yet
- Towards An Animal Model of Food Addiction: Obesity Facts April 2012Document17 pagesTowards An Animal Model of Food Addiction: Obesity Facts April 2012Eddy JayNo ratings yet
- The Role of Diet and Nutrition On Mental Health and WellbeingDocument3 pagesThe Role of Diet and Nutrition On Mental Health and WellbeingMeha RajNo ratings yet
- Obesity and Responsibility: Is It Time To Rethink Agency?Document8 pagesObesity and Responsibility: Is It Time To Rethink Agency?Ibrahima Séga Jr SangaréNo ratings yet
- Michalak-Vegetarian 2012Document11 pagesMichalak-Vegetarian 2012Ira GladchukNo ratings yet
- EDIFY Eating Disorders Delineating Illness and RecDocument9 pagesEDIFY Eating Disorders Delineating Illness and RecNealNo ratings yet
- Obesogens: A Unifying Theory For The Global Rise in Obesity: International Journal of ObesityDocument12 pagesObesogens: A Unifying Theory For The Global Rise in Obesity: International Journal of Obesityprajjalita borahNo ratings yet
- Affect, Object Relation and Eating DisordersDocument10 pagesAffect, Object Relation and Eating DisordersGloria KentNo ratings yet
- CONFERENCIA..motivación en ObesidadDocument6 pagesCONFERENCIA..motivación en ObesidadJavier AlvarezNo ratings yet
- Brain Change in Addiction As LDocument11 pagesBrain Change in Addiction As Lanthea.scerri-richard.02No ratings yet
- Ijerph 18 11269Document9 pagesIjerph 18 11269driveamadeaNo ratings yet
- Neuropharmacology of Compulsive Eating: ReviewDocument9 pagesNeuropharmacology of Compulsive Eating: ReviewIusti MariNo ratings yet
- Euro Eating Disorders Rev - 2022 - Nimbley - Sensory Processing and Eating Behaviours in Autism A Systematic ReviewDocument22 pagesEuro Eating Disorders Rev - 2022 - Nimbley - Sensory Processing and Eating Behaviours in Autism A Systematic Reviewars_80No ratings yet
- Hoebel e Avena - Açúcar e VícioDocument18 pagesHoebel e Avena - Açúcar e VícioGracielaRecheNo ratings yet
- T2D Patient Impowerment PDFDocument11 pagesT2D Patient Impowerment PDFRafikNo ratings yet
- Texto para TrabajarDocument2 pagesTexto para TrabajarAnnaNo ratings yet
- Dietary Interventions in Mild Cognitive Impairment and DementiaDocument14 pagesDietary Interventions in Mild Cognitive Impairment and Dementialina ningdyarNo ratings yet
- ORG7510 Monday 91145pm WK6 The Addiction Methodology of Bio Psychology CHRISTIEGYdocxDocument11 pagesORG7510 Monday 91145pm WK6 The Addiction Methodology of Bio Psychology CHRISTIEGYdocxYvonne ChristieNo ratings yet
- Example Paper - Health Psychol - 2021 - Foley - Just Keep Taking Them Keep Hoping They LL Work A Qualitative Study of AdheringDocument25 pagesExample Paper - Health Psychol - 2021 - Foley - Just Keep Taking Them Keep Hoping They LL Work A Qualitative Study of Adheringdr.serpilcakirNo ratings yet
- British J Pharmacology - 2022 - Laque - Linking Drug and Food Addiction Via Compulsive AppetiteDocument21 pagesBritish J Pharmacology - 2022 - Laque - Linking Drug and Food Addiction Via Compulsive AppetiteElisa RodríguezNo ratings yet
- Author's Accepted Manuscript: Journal of Affective DisordersDocument47 pagesAuthor's Accepted Manuscript: Journal of Affective DisordersTito AlhoNo ratings yet
- 0-Addicto Craving Hone-Blanchet (2014)Document15 pages0-Addicto Craving Hone-Blanchet (2014)gildas5d5almeidaNo ratings yet
- Article 1 Anorexia NervosaDocument7 pagesArticle 1 Anorexia Nervosayeremia imanuelNo ratings yet
- Nres1dm-Chapter I and IIDocument35 pagesNres1dm-Chapter I and IImlmmandapNo ratings yet
- Processes and Pathways To Binge Eating DevelopmentDocument10 pagesProcesses and Pathways To Binge Eating Developmentsuporteflnc02No ratings yet
- Mindfulness-Based Interventions For Obesity-Related Eating Behaviors: A Literature ReviewDocument20 pagesMindfulness-Based Interventions For Obesity-Related Eating Behaviors: A Literature ReviewEliseia CarvalhoNo ratings yet
- Literature Review Eating DisordersDocument12 pagesLiterature Review Eating Disordersafmzaoahmicfxg100% (1)
- Yau, Stress Eating Behaviors, 2013Document17 pagesYau, Stress Eating Behaviors, 2013Maribel Ruiz BurgaNo ratings yet
- A Systematic Review On The Kap-O Framework For Diabetes Education and ResearchDocument21 pagesA Systematic Review On The Kap-O Framework For Diabetes Education and ResearchToyour EternityNo ratings yet
- Food Addiction Denial: False Information and Irrational ThinkingFrom EverandFood Addiction Denial: False Information and Irrational ThinkingNo ratings yet
- Holzel Et Al 2Document20 pagesHolzel Et Al 2jlawrenceNo ratings yet
- PsychoanalysisDocument30 pagesPsychoanalysisjaydokNo ratings yet
- REVIEW QUIZ - Schemas - Modified Jan 24 2014Document2 pagesREVIEW QUIZ - Schemas - Modified Jan 24 2014Srnt YyoNo ratings yet
- Chapter Two-Foundation of Individual Behavior and Learning in An OrganizationDocument14 pagesChapter Two-Foundation of Individual Behavior and Learning in An OrganizationMikias DegwaleNo ratings yet
- TCMP Implementation PolicyDocument8 pagesTCMP Implementation PolicyBeulah Aurora GonzagaNo ratings yet
- When Clients Can't Connect With or Name Their Emotions - Russ Harris - EbookDocument27 pagesWhen Clients Can't Connect With or Name Their Emotions - Russ Harris - Ebook2qf4ffhsh2No ratings yet
- Noun & Preposition Collocations With OF. Noun & Preposition Collocations With FORDocument3 pagesNoun & Preposition Collocations With OF. Noun & Preposition Collocations With FORLavinia GherasimNo ratings yet
- Nancy Roper's Contribution To Nursing Theory: Roper-Logan-Tierney Model of NursingDocument9 pagesNancy Roper's Contribution To Nursing Theory: Roper-Logan-Tierney Model of NursingBeatrice ChenNo ratings yet
- The Effects of E-Cigarette Smoking To The Academic Performance of StudentsDocument4 pagesThe Effects of E-Cigarette Smoking To The Academic Performance of StudentsAngelie Rañera ValenzuelaNo ratings yet
- Snow White's Short AnalysisDocument3 pagesSnow White's Short AnalysisDavid GomezNo ratings yet
- Introduction To Human Resource Development: Werner & Desimone (2006) 1Document28 pagesIntroduction To Human Resource Development: Werner & Desimone (2006) 1michaelbensonbabuNo ratings yet
- Unit 1Document42 pagesUnit 1Anushka MishraNo ratings yet
- 2p-Review of DapDocument10 pages2p-Review of DapDess DotimasNo ratings yet
- PersonalDevelopment - Q1 - Mod 3 - DevelopmentalTasksAccordingToDevelopmentalStages - v5Document31 pagesPersonalDevelopment - Q1 - Mod 3 - DevelopmentalTasksAccordingToDevelopmentalStages - v5KryssssNo ratings yet
- Transactional AnalysisDocument9 pagesTransactional Analysisarush9211No ratings yet
- William Glasser: Choice Theory: By: Jessica Young Allison Arriaga Nicole Schreiber Michael LamorgeseDocument25 pagesWilliam Glasser: Choice Theory: By: Jessica Young Allison Arriaga Nicole Schreiber Michael Lamorgesesekiz888No ratings yet
- Josue Jimenez EDSP 525 Case Study: Dr. RamirezDocument12 pagesJosue Jimenez EDSP 525 Case Study: Dr. Ramirezapi-481591637No ratings yet
- Chapter 2Document4 pagesChapter 2Bayu Christiana AdiNo ratings yet
- Principle of Management (Organizational Culture)Document11 pagesPrinciple of Management (Organizational Culture)Samy. E.N.DNo ratings yet
- Technical Communication NotesDocument3 pagesTechnical Communication NotesManak JainNo ratings yet
- K02873 - 20180529171509 - Chapter 12 Hergenhahn 7e FinalDocument33 pagesK02873 - 20180529171509 - Chapter 12 Hergenhahn 7e Finalzuh blackNo ratings yet
- HR For Non HR ManagersDocument58 pagesHR For Non HR ManagersStephen OliekaNo ratings yet
- FBI The School Shooter A Quick Reference GuideDocument1 pageFBI The School Shooter A Quick Reference GuidePaul FarrellNo ratings yet
- FunctinalismDocument13 pagesFunctinalismGerson GeingobNo ratings yet
- Topic01 Intro HistoryDocument46 pagesTopic01 Intro HistoryFareeha KhanNo ratings yet
- Group DynamicsDocument15 pagesGroup DynamicsAmarri ColeNo ratings yet
- Detecting Crucial StrategiesDocument11 pagesDetecting Crucial StrategieserickimanziNo ratings yet
- Wier, Kelly, 11-12-14, Formal Observation, FiDocument4 pagesWier, Kelly, 11-12-14, Formal Observation, Fiapi-242012292No ratings yet
- Esai Bahasa InggrisDocument10 pagesEsai Bahasa InggrisWahyu KurniawanNo ratings yet