Download as pdf or txt
You might also like
- MoH Adverse Events Policy PDFDocument33 pagesMoH Adverse Events Policy PDFnayan4uNo ratings yet
- JC Frailty As A Risk Predictor in Cardiac SurgeryDocument30 pagesJC Frailty As A Risk Predictor in Cardiac SurgeryFaizan Ahmad AliNo ratings yet
- Catheter Cardiovasc Interv 2021 May 27 Romeo FJDocument8 pagesCatheter Cardiovasc Interv 2021 May 27 Romeo FJFernando SousaNo ratings yet
- Acute Renal Failure in Critically Ill Surgical Patients PDFDocument7 pagesAcute Renal Failure in Critically Ill Surgical Patients PDFRomán Jiménez LópezNo ratings yet
- Fried Frailty Pred Surg Outcomes AmCSurg 10Document8 pagesFried Frailty Pred Surg Outcomes AmCSurg 10edos838No ratings yet
- El Kersh2015Document8 pagesEl Kersh2015Sathoodeh BanuNo ratings yet
- Pengertian Status Fisik ASADocument8 pagesPengertian Status Fisik ASARiki HidayatullahNo ratings yet
- Santos 2018Document7 pagesSantos 2018Bertha FransiscaNo ratings yet
- PIIS1078588419310755Document7 pagesPIIS1078588419310755zeeshan qurbanNo ratings yet
- Tabata 2014Document6 pagesTabata 2014Kings AndrewNo ratings yet
- Serum Biomarkers Related To Frailty Predict Negative Outcomes in Older Adults With Hip FractureDocument10 pagesSerum Biomarkers Related To Frailty Predict Negative Outcomes in Older Adults With Hip FractureBernardo Abel Cedeño VelozNo ratings yet
- Repair of Rotator Cuff Tears in The Elderly: Does It Make Sense?Document10 pagesRepair of Rotator Cuff Tears in The Elderly: Does It Make Sense?Gustavo BECERRA PERDOMONo ratings yet
- Frailty and AnesthesiaDocument33 pagesFrailty and AnesthesiaRadmila KaranNo ratings yet
- Gait Speed, Grip Strength, and Clinical Outcomes in Older Patients With Hematologic MalignanciesDocument9 pagesGait Speed, Grip Strength, and Clinical Outcomes in Older Patients With Hematologic MalignanciesTícia RanessaNo ratings yet
- Increased Heart Rate During Walk Test Predicts Chronic-Phase Worsening of Renal Function in Patients With Acute Myocardial Infarction and Normal Kidney FunctionDocument10 pagesIncreased Heart Rate During Walk Test Predicts Chronic-Phase Worsening of Renal Function in Patients With Acute Myocardial Infarction and Normal Kidney Functionvn0328897777No ratings yet
- Giglio 2018Document11 pagesGiglio 2018yafanitaizzatiNo ratings yet
- Cardiac ValveDocument9 pagesCardiac Valveikbal rambalinoNo ratings yet
- Addendum of Newer Anticoagulants To The SIR Consensus GuidelineDocument5 pagesAddendum of Newer Anticoagulants To The SIR Consensus GuidelineCenith De Los ReyesNo ratings yet
- 2021 Special Care in Dentistry Detection of Calcified AtheromasDocument6 pages2021 Special Care in Dentistry Detection of Calcified AtheromasNATALIA SILVA ANDRADENo ratings yet
- 10 1016@j Eurger 2016 01 005 PDFDocument4 pages10 1016@j Eurger 2016 01 005 PDFBasilio Papuico RomeroNo ratings yet
- Reliability of Gait Performance Tests in Men and Women With Hemiparesis After StrokeDocument8 pagesReliability of Gait Performance Tests in Men and Women With Hemiparesis After StrokeKaniNo ratings yet
- Analysis of Post Operative Systemic To Pulmonary Artery Shunt FailureDocument5 pagesAnalysis of Post Operative Systemic To Pulmonary Artery Shunt FailurePaul HartingNo ratings yet
- The Shortfall in Long-Term Survival of Patients With Repaired Thoracic Orabdominal Aortic Aneurysms Retrospective CaseeControl Analysis Ofhospital Episode StatisticsDocument9 pagesThe Shortfall in Long-Term Survival of Patients With Repaired Thoracic Orabdominal Aortic Aneurysms Retrospective CaseeControl Analysis Ofhospital Episode StatisticsJeffery TaylorNo ratings yet
- Accuracy of Achalasia Quality of Life and Eckardt Scores For Assessment of Clinical Improvement Post Treatment For AchalasiaDocument9 pagesAccuracy of Achalasia Quality of Life and Eckardt Scores For Assessment of Clinical Improvement Post Treatment For AchalasiaykommNo ratings yet
- Calder 2016 - Meta Analysis and Suggested Guidelines For Prevention of Venous Thromboembolism (VTE) in Foot and Ankle SurgeryDocument12 pagesCalder 2016 - Meta Analysis and Suggested Guidelines For Prevention of Venous Thromboembolism (VTE) in Foot and Ankle SurgeryNoel Yongshen LeeNo ratings yet
- Journal of Clinical & Translational EndocrinologyDocument5 pagesJournal of Clinical & Translational EndocrinologyRicky BooyNo ratings yet
- Hs 15069Document4 pagesHs 15069Deepak RanaNo ratings yet
- A Randomized Controlled Trial of Endovascular Aneurysm Repair Versus Open Surgery For Abdominal Aortic Aneurysms in Low - To Moderate-Risk PatientsDocument8 pagesA Randomized Controlled Trial of Endovascular Aneurysm Repair Versus Open Surgery For Abdominal Aortic Aneurysms in Low - To Moderate-Risk Patientsvfd08051996No ratings yet
- Atm 09 02 118Document10 pagesAtm 09 02 118idham shadiqNo ratings yet
- International Journal of Cardiology: Contents Lists Available atDocument8 pagesInternational Journal of Cardiology: Contents Lists Available atWesleyMesquitaNo ratings yet
- Yejvs - 7376Document14 pagesYejvs - 7376Francisco Álvarez MarcosNo ratings yet
- 24 Rudrajit EtalDocument6 pages24 Rudrajit EtaleditorijmrhsNo ratings yet
- The Model For End-Stage Liver DiseaseDocument9 pagesThe Model For End-Stage Liver Diseasegwyneth.green.512No ratings yet
- CC 4915Document10 pagesCC 4915Livia Meidy UbayidNo ratings yet
- 3 Ijmpsoct20173Document6 pages3 Ijmpsoct20173TJPRC PublicationsNo ratings yet
- Wang Et Al - Older Age and Outcome AfterDocument9 pagesWang Et Al - Older Age and Outcome AfterMurat MukharyamovNo ratings yet
- 11 134 v12n4 2013 PredictingPortalDocument11 pages11 134 v12n4 2013 PredictingPortalDevy Widiya GrafitasariNo ratings yet
- Alvarado Scoring in Acute Appendicitis-A Clinicopathological CorrelationDocument5 pagesAlvarado Scoring in Acute Appendicitis-A Clinicopathological CorrelationMahlina Nur LailiNo ratings yet
- A New Operational Definition of Frailty The Frailty Trait Scale - Garcia - Garcia2014Document7 pagesA New Operational Definition of Frailty The Frailty Trait Scale - Garcia - Garcia2014dariorguezNo ratings yet
- 2021 Article 10158Document10 pages2021 Article 10158juajimenez55No ratings yet
- Displasia de CaderaDocument10 pagesDisplasia de CaderaPAOLA ESTEFANIA ESPINOZA CASTRONo ratings yet
- Bessire 2014Document7 pagesBessire 2014andrei3cucuNo ratings yet
- Radiol 2019190734Document10 pagesRadiol 2019190734Dimas agung okoputraNo ratings yet
- F QRSDocument9 pagesF QRSaisyah hamzakirNo ratings yet
- The Alvarado Score For Predicting Acute Appendicitis: A Systematic ReviewDocument13 pagesThe Alvarado Score For Predicting Acute Appendicitis: A Systematic ReviewAndy Zevallos AraujoNo ratings yet
- 2003-Academic Emergency MedicineDocument154 pages2003-Academic Emergency MedicinealiceNo ratings yet
- Annsurg00185 0122Document6 pagesAnnsurg00185 0122Fajr MuzammilNo ratings yet
- SMJ 56 626Document6 pagesSMJ 56 626Andy HongNo ratings yet
- Vesconi 2009Document14 pagesVesconi 2009Nguyễn Đức LongNo ratings yet
- Validity of Grace Risk Score To Predict The Prognosis in Elderly Patients With Acute Coronary SyndromeDocument9 pagesValidity of Grace Risk Score To Predict The Prognosis in Elderly Patients With Acute Coronary SyndromeFachry MuhammadNo ratings yet
- 10.1007@s11739 019 02196 ZDocument10 pages10.1007@s11739 019 02196 ZMaharani Sari NastitiNo ratings yet
- Søvik2019 Article AcuteKidneyInjuryInTraumaPatie PDFDocument13 pagesSøvik2019 Article AcuteKidneyInjuryInTraumaPatie PDFamal.fathullahNo ratings yet
- ScienceDocument6 pagesSciencesddfsfNo ratings yet
- CSM 3 2 46 52Document7 pagesCSM 3 2 46 52Santoso 9JimmyNo ratings yet
- NutritionDocument10 pagesNutritionDani ursNo ratings yet
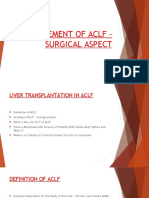
- Management of AclfDocument30 pagesManagement of Aclfsaraswathy sNo ratings yet
- Extracorporeal Life Support in Pediatric Cardiac DysfunctionDocument5 pagesExtracorporeal Life Support in Pediatric Cardiac DysfunctionNoor Aida AriyaniNo ratings yet
- Artigo TX Bia 2011Document5 pagesArtigo TX Bia 2011gutorpNo ratings yet
- Vanreijen 2019Document10 pagesVanreijen 2019Ivor Wiguna Hartanto WilopoNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyFrom EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyRating: 1 out of 5 stars1/5 (1)
- Complementary and Alternative Medical Lab Testing Part 17: OncologyFrom EverandComplementary and Alternative Medical Lab Testing Part 17: OncologyNo ratings yet
- J Clin Rheumatol 2021 Aug 2 Fernandez-Avila DGDocument4 pagesJ Clin Rheumatol 2021 Aug 2 Fernandez-Avila DGFernando SousaNo ratings yet
- J Hepatol 2022 Jan 20 Pape S Mat Compl 1Document17 pagesJ Hepatol 2022 Jan 20 Pape S Mat Compl 1Fernando SousaNo ratings yet
- Disaster Med Public Health Prep 2021 Aug 2 Cereghini JDocument11 pagesDisaster Med Public Health Prep 2021 Aug 2 Cereghini JFernando SousaNo ratings yet
- Pediatr Transplant 2021 E14105Document4 pagesPediatr Transplant 2021 E14105Fernando SousaNo ratings yet
- J Rheumatol 2021 Jun 15 Fernandez-Avila DGDocument7 pagesJ Rheumatol 2021 Jun 15 Fernandez-Avila DGFernando SousaNo ratings yet
- Hypertension 2020 76 2 333-41Document9 pagesHypertension 2020 76 2 333-41Fernando SousaNo ratings yet
- Orthop J Sports Med 2021 9 7 23259671211013394Document6 pagesOrthop J Sports Med 2021 9 7 23259671211013394Fernando SousaNo ratings yet
- Eur Child Adolesc Psychiatry 2020 29 1 71-81Document11 pagesEur Child Adolesc Psychiatry 2020 29 1 71-81Fernando SousaNo ratings yet
- Eur J Ophthalmol 2020 May 13 Diamint DVDocument5 pagesEur J Ophthalmol 2020 May 13 Diamint DVFernando SousaNo ratings yet
- Epilepsy Behav 2020 112 107447Document4 pagesEpilepsy Behav 2020 112 107447Fernando SousaNo ratings yet
- Effect of PEEP On Dead Space in An Experimental Model of ARDSDocument10 pagesEffect of PEEP On Dead Space in An Experimental Model of ARDSFernando SousaNo ratings yet
- J Thromb Thrombolysis 2020 Sep 14 Smith DDocument8 pagesJ Thromb Thrombolysis 2020 Sep 14 Smith DFernando SousaNo ratings yet
- Acr 1st NsedDocument2 pagesAcr 1st NsedRey SilvestreNo ratings yet
- Yseali Younified 2020 A Guide To Planning A Community Service ActivityDocument17 pagesYseali Younified 2020 A Guide To Planning A Community Service ActivityHamidatun NisaNo ratings yet
- Home EconomicsDocument5 pagesHome EconomicsNicole Kathleen Caranto100% (1)
- Anandhu M AVT Academy 1486Document17 pagesAnandhu M AVT Academy 1486anandmg41No ratings yet
- COPD Case Pres2Document29 pagesCOPD Case Pres2Kelly Queenie Andres100% (2)
- 2012 Resistant HypertensionDocument9 pages2012 Resistant HypertensionBarry Tumpal Wouter NapitupuluNo ratings yet
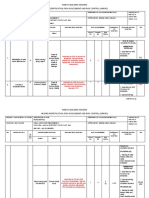
- SPC HIRADC - 022 - Road WorksDocument5 pagesSPC HIRADC - 022 - Road WorksKalai ArasanNo ratings yet
- FORM 4.1 Self Assesment Check ListDocument3 pagesFORM 4.1 Self Assesment Check ListNica ManlugonNo ratings yet
- Medical GasesDocument20 pagesMedical Gasesmagicarray.hrNo ratings yet
- Chronic MeningitisDocument7 pagesChronic Meningitisneurojuancarfab100% (1)
- Janitorial ProductivityDocument7 pagesJanitorial ProductivityThe Cleaning LibraryNo ratings yet
- The Who Five Keys To Safer Food A Tool For Food Safety Health PromotionDocument15 pagesThe Who Five Keys To Safer Food A Tool For Food Safety Health PromotionCarlos RuizNo ratings yet
- KasaiDocument7 pagesKasaishalukiriNo ratings yet
- MSDS AstDocument6 pagesMSDS AstKRRNo ratings yet
- Things We Do For No Reason: Calculating A "Corrected Calcium" LevelDocument3 pagesThings We Do For No Reason: Calculating A "Corrected Calcium" LevelCsr ArsNo ratings yet
- Macro Analysis PhilippinesDocument9 pagesMacro Analysis PhilippinesAnthony AlferesNo ratings yet
- Nursing Care Plan - Fatigue (Antepartum)Document3 pagesNursing Care Plan - Fatigue (Antepartum)kaimimiyaNo ratings yet
- MEDICARDDocument19 pagesMEDICARDSrcdc CooperativeNo ratings yet
- Advance Project Final FeasibilityDocument31 pagesAdvance Project Final FeasibilityMohammad Adil ChoudharyNo ratings yet
- Codependency Treatment Systematic Review 2015Document12 pagesCodependency Treatment Systematic Review 2015Ryan PetersonNo ratings yet
- 37 - Hematuria & RCCDocument53 pages37 - Hematuria & RCCRashed ShatnawiNo ratings yet
- Reviste Medicale Internationale Cotate IsiDocument28 pagesReviste Medicale Internationale Cotate IsidoruNo ratings yet
- Prevalence of Rifampicin Resistance Tuberculosis and Associated Factors Among Presumptive TB or MDRDocument3 pagesPrevalence of Rifampicin Resistance Tuberculosis and Associated Factors Among Presumptive TB or MDRTigray OutlookNo ratings yet
- Research Agenda of The College of Business and Entrepreneurship - DDocument57 pagesResearch Agenda of The College of Business and Entrepreneurship - DSev BlancoNo ratings yet
- Pharm Test BankDocument5 pagesPharm Test BankMorgan SmithNo ratings yet
- Requirements For Vessels Arriving in The Port of SingaporeDocument10 pagesRequirements For Vessels Arriving in The Port of SingaporenarutorazNo ratings yet
- Lesson Plan - Detecting The Mood Disorder FinalDocument2 pagesLesson Plan - Detecting The Mood Disorder FinalTrixie MizonaNo ratings yet
- SCIDDocument10 pagesSCIDIbrahimNo ratings yet
- Checked Testing Effectiveness of Types of ToothpasteDocument9 pagesChecked Testing Effectiveness of Types of ToothpasteMaya AltahaNo ratings yet