
Routes of Drug administration-RuizScioliMontoto
Routes of Drug administration-RuizScioliMontoto
You might also like
- Biopharmaceutics - BrahmankarDocument414 pagesBiopharmaceutics - Brahmankarmatin586% (58)
- Pharmacology For Nurses Lecture Notes: ContentsDocument20 pagesPharmacology For Nurses Lecture Notes: ContentsTuya Rosales100% (1)
- Routes of Drug AdministrationDocument44 pagesRoutes of Drug AdministrationFaith GabrielNo ratings yet
- Routes of Drug Administration: Dosage, Design, and Pharmacotherapy SuccessDocument44 pagesRoutes of Drug Administration: Dosage, Design, and Pharmacotherapy SuccessRahul PatilNo ratings yet
- Routes of Drug Administration Vias AdministracionDocument37 pagesRoutes of Drug Administration Vias AdministracionAMAYRANI CITLALI TORAL OROZCONo ratings yet
- 698 PDF PDFDocument8 pages698 PDF PDFMuh Indra SudirjaNo ratings yet
- Bp704t Ndds IDocument25 pagesBp704t Ndds Iapplied chemistNo ratings yet
- PharmacokintaticDocument38 pagesPharmacokintaticnoor norNo ratings yet
- P Tech Assignment 1Document7 pagesP Tech Assignment 1Rana Aakif SaleemNo ratings yet
- Drug Delivery Technologies. The Way Forward in The New Decade (Review)Document12 pagesDrug Delivery Technologies. The Way Forward in The New Decade (Review)georgiaNo ratings yet
- Introduction To Novel Drug Delivery SystDocument5 pagesIntroduction To Novel Drug Delivery SystshreeharilxrNo ratings yet
- General Pharmacology Nina 2017-2018newDocument33 pagesGeneral Pharmacology Nina 2017-2018newSheba RoymonNo ratings yet
- Pharma 1,2Document10 pagesPharma 1,2Ahmed KafajiNo ratings yet
- Nama Inovator ObatDocument8 pagesNama Inovator ObatAmiro AuliaNo ratings yet
- Implantable Therapeutic Systems: Introduction of ImplantDocument16 pagesImplantable Therapeutic Systems: Introduction of ImplantUma MaheswararaoNo ratings yet
- Controlled Release Drug Formulation in Pharmaceuticals: A Study On Their Application and PropertiesDocument17 pagesControlled Release Drug Formulation in Pharmaceuticals: A Study On Their Application and PropertiesintanNo ratings yet
- YyyyDocument12 pagesYyyyRohan SharmaNo ratings yet
- A Prolonged Release Parenteral Drug Delivery SystemDocument11 pagesA Prolonged Release Parenteral Drug Delivery SystemronnymcmNo ratings yet
- Introduction To PharmacologyDocument50 pagesIntroduction To PharmacologyAbdishakour Hassa.100% (1)
- Assigment Controlled Drug Delivery SystemDocument5 pagesAssigment Controlled Drug Delivery SystemZainab AbdullahiNo ratings yet
- Mechanism of Implantable Drug Delivery SystemsDocument48 pagesMechanism of Implantable Drug Delivery SystemsTanveer AhmedNo ratings yet
- Practical 2Document5 pagesPractical 2Arooj FatimaNo ratings yet
- Historical Perspective of CDDSDocument3 pagesHistorical Perspective of CDDSHemant BhattNo ratings yet
- 4 RJPDFT 10 4 2018Document13 pages4 RJPDFT 10 4 2018Fransisco AlfredoNo ratings yet
- 1 - Pendahuluan - Drug Delivery Systems-09 2016Document26 pages1 - Pendahuluan - Drug Delivery Systems-09 2016Kos KosasihNo ratings yet
- Atrigel A Potential Parenteral Controlled Drug Delivery SystemDocument8 pagesAtrigel A Potential Parenteral Controlled Drug Delivery SystemMaria RoswitaNo ratings yet
- Ijps258 269Document12 pagesIjps258 269Kristine Dwi PuspitasariNo ratings yet
- 4 - Drug Product Design ParametersDocument7 pages4 - Drug Product Design ParametersVinz AlvarezNo ratings yet
- NDDS (BP704) IDocument22 pagesNDDS (BP704) Ihasan.aliNo ratings yet
- NDDS AnswersDocument56 pagesNDDS AnswersPrajwal PatankarNo ratings yet
- Chapter 1Document32 pagesChapter 1Czerwin JualesNo ratings yet
- Unit One of PharmacologyDocument63 pagesUnit One of PharmacologyAbdinaasir MohamedNo ratings yet
- Controlled Drug DeliveryDocument23 pagesControlled Drug DeliveryAnburaj JamesNo ratings yet
- Biopharm 2Document3 pagesBiopharm 2muzzamiluswaNo ratings yet
- AbsorptionDocument84 pagesAbsorptionDr. Bharat JainNo ratings yet
- Diploma EEE DocumentDocument72 pagesDiploma EEE DocumentJaganMohanGuduruNo ratings yet
- تصميم كويزDocument73 pagesتصميم كويزHemo HindiNo ratings yet
- Brahmakar - Biopharmaceutics & PharmacokineticsDocument374 pagesBrahmakar - Biopharmaceutics & PharmacokineticsSamritiNo ratings yet
- PumpsOsmotic-Duros Osmotic Implant For HumansDocument15 pagesPumpsOsmotic-Duros Osmotic Implant For Humansomar100% (1)
- Biopharmaceutics - 1 2022Document24 pagesBiopharmaceutics - 1 2022Varshini VarshaNo ratings yet
- Gupta Kumar - Nano Meningkatkan BA DLLDocument40 pagesGupta Kumar - Nano Meningkatkan BA DLLHesti HariantiNo ratings yet
- What Is PharmacologyDocument5 pagesWhat Is PharmacologyShardendu MishraNo ratings yet
- Review On Immediate Drug Released Dosage FormDocument8 pagesReview On Immediate Drug Released Dosage FormEditor IJTSRDNo ratings yet
- New Era University: Pharmacology For MidwiferyDocument11 pagesNew Era University: Pharmacology For MidwiferyHarriegail O. LontocNo ratings yet
- Topical Drug DeliveryDocument21 pagesTopical Drug DeliveryhappyNo ratings yet
- Document 2Document9 pagesDocument 2zoha fatimaNo ratings yet
- Article Wjpps 14988056511Document12 pagesArticle Wjpps 14988056511Its MENo ratings yet
- Pharmacokinetics and PharmacodynamicsDocument113 pagesPharmacokinetics and PharmacodynamicsEvelyn MedinaNo ratings yet
- Introduction To Pharmacology: Katzung, Bertram G, Susan B. Masters, and Anthony J. Trevor. Basic & ClinicalDocument40 pagesIntroduction To Pharmacology: Katzung, Bertram G, Susan B. Masters, and Anthony J. Trevor. Basic & Clinicaljamila ilNo ratings yet
- ParenteralDocument4 pagesParenteralreymar.martinez88No ratings yet
- A Prolonged Release Parenteral Drug Delivery System - An OverviewDocument11 pagesA Prolonged Release Parenteral Drug Delivery System - An Overviewcristian135No ratings yet
- SRDDS Matrix TabletDocument17 pagesSRDDS Matrix TabletMISBAH KAUSARNo ratings yet
- 6Document11 pages6UgaugaaNo ratings yet
- Review Article VikashdashDocument4 pagesReview Article VikashdashamjohnnyNo ratings yet
- Parenteral Drug AbsorptionDocument24 pagesParenteral Drug AbsorptionAsnakeNo ratings yet
- 17.alekhya Research ArticleDocument8 pages17.alekhya Research ArticleBaru Chandrasekhar RaoNo ratings yet
- Microneedle-mediated Transdermal and Intradermal Drug DeliveryFrom EverandMicroneedle-mediated Transdermal and Intradermal Drug DeliveryNo ratings yet
- Pharmacology- The Molecular Dance: Understanding Drug Interactions: Harmony and Chaos: The Symphony of Drug InteractionsFrom EverandPharmacology- The Molecular Dance: Understanding Drug Interactions: Harmony and Chaos: The Symphony of Drug InteractionsNo ratings yet
- EthoxDocument24 pagesEthoxAlfredo MéndezNo ratings yet
- H2so4 20% - MSDSDocument6 pagesH2so4 20% - MSDSPhạm Văn HiếuNo ratings yet
- Fluid Flow Assurance Issues Literature ReviewDocument12 pagesFluid Flow Assurance Issues Literature ReviewMatahari SenjaNo ratings yet
- MSDS Calsium OxideDocument6 pagesMSDS Calsium OxidePipit RatnasariNo ratings yet
- Microbiological Beneficiation of Low Grade Manganese Ores: A ReviewDocument21 pagesMicrobiological Beneficiation of Low Grade Manganese Ores: A ReviewSEP-PublisherNo ratings yet
- CREII-Module-4 - Lecture 18 & 19 PDFDocument21 pagesCREII-Module-4 - Lecture 18 & 19 PDFshubhamNo ratings yet
- Earthscience, PPTDocument12 pagesEarthscience, PPTAlaisa Claire Dela TorreNo ratings yet
- Qualitative Analysis NotesDocument1 pageQualitative Analysis NotesNaseema MalikNo ratings yet
- Final Report of The Amended Safety Assessment of Glyceryl LaurateDocument40 pagesFinal Report of The Amended Safety Assessment of Glyceryl LaurateSam SonNo ratings yet
- Slide 1Document68 pagesSlide 1KASPER كاسبرNo ratings yet
- Kemp P H 1969Document278 pagesKemp P H 1969RICARDO DE FREITAS FERNANDES PONTESNo ratings yet
- MIST 2019-2020 QuestionDocument4 pagesMIST 2019-2020 QuestionmackenzieoleoNo ratings yet
- MSDS DIaliser ElisioDocument6 pagesMSDS DIaliser Elisioika setiawatiNo ratings yet
- Separation and Purification of Organic CompoundsDocument8 pagesSeparation and Purification of Organic CompoundsRachel Jean OlarteNo ratings yet
- PiroxicamDocument4 pagesPiroxicamSahil AliNo ratings yet
- ODI-TOX SILVER (Toxin Binder) MSDSDocument4 pagesODI-TOX SILVER (Toxin Binder) MSDSTazia DuldulNo ratings yet
- PT Final Exam Level-II (Specific)Document5 pagesPT Final Exam Level-II (Specific)RohitNo ratings yet
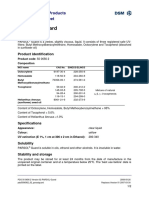
- Parsol Guard-Hoja de Datos (DSM)Document2 pagesParsol Guard-Hoja de Datos (DSM)LuisCastilloCastroNo ratings yet
- Chem LabDocument44 pagesChem LabalbertoNo ratings yet
- Propilparabeno HandbookDocument3 pagesPropilparabeno HandbookCarlos Fernando Jacobo PérezNo ratings yet
- Acrylic Modified Water Soluble Oil Based CoatingsDocument4 pagesAcrylic Modified Water Soluble Oil Based Coatingsichsan hakimNo ratings yet
- Liquid Liquid ExtractionDocument34 pagesLiquid Liquid ExtractionTubagusNo ratings yet
- Gr. 7 Science TG (Q1 To 4)Document224 pagesGr. 7 Science TG (Q1 To 4)Qwyn Vylette Sanson67% (9)
- PRE4122 Exercise No. 4 Imperfections in SolidsDocument9 pagesPRE4122 Exercise No. 4 Imperfections in SolidsعبداللهأحمدNo ratings yet
- SolutionsDocument11 pagesSolutionsBeatriz G. AblayNo ratings yet
- FL SopDocument45 pagesFL SopSara JohnsonNo ratings yet
- Seminar Report On "Water Breakthrough" Submitted To Savitribai Phule Pune UniversityDocument34 pagesSeminar Report On "Water Breakthrough" Submitted To Savitribai Phule Pune UniversityFINAL YEAR PETROLEUM 2020 BATCHNo ratings yet
- CH 1 - Introduction To ChemistryDocument30 pagesCH 1 - Introduction To ChemistryvncntmarlesNo ratings yet
- Biochem Lab ReportDocument4 pagesBiochem Lab ReportChryza Faith QuicoyNo ratings yet
- Industrial Production of L-GlutamineDocument4 pagesIndustrial Production of L-Glutamineedal_108No ratings yet























































































Download as pdf or txt
You might also like
- Biopharmaceutics - BrahmankarDocument414 pagesBiopharmaceutics - Brahmankarmatin586% (58)
- Pharmacology For Nurses Lecture Notes: ContentsDocument20 pagesPharmacology For Nurses Lecture Notes: ContentsTuya Rosales100% (1)
- Routes of Drug AdministrationDocument44 pagesRoutes of Drug AdministrationFaith GabrielNo ratings yet
- Routes of Drug Administration: Dosage, Design, and Pharmacotherapy SuccessDocument44 pagesRoutes of Drug Administration: Dosage, Design, and Pharmacotherapy SuccessRahul PatilNo ratings yet
- Routes of Drug Administration Vias AdministracionDocument37 pagesRoutes of Drug Administration Vias AdministracionAMAYRANI CITLALI TORAL OROZCONo ratings yet
- 698 PDF PDFDocument8 pages698 PDF PDFMuh Indra SudirjaNo ratings yet
- Bp704t Ndds IDocument25 pagesBp704t Ndds Iapplied chemistNo ratings yet
- PharmacokintaticDocument38 pagesPharmacokintaticnoor norNo ratings yet
- P Tech Assignment 1Document7 pagesP Tech Assignment 1Rana Aakif SaleemNo ratings yet
- Drug Delivery Technologies. The Way Forward in The New Decade (Review)Document12 pagesDrug Delivery Technologies. The Way Forward in The New Decade (Review)georgiaNo ratings yet
- Introduction To Novel Drug Delivery SystDocument5 pagesIntroduction To Novel Drug Delivery SystshreeharilxrNo ratings yet
- General Pharmacology Nina 2017-2018newDocument33 pagesGeneral Pharmacology Nina 2017-2018newSheba RoymonNo ratings yet
- Pharma 1,2Document10 pagesPharma 1,2Ahmed KafajiNo ratings yet
- Nama Inovator ObatDocument8 pagesNama Inovator ObatAmiro AuliaNo ratings yet
- Implantable Therapeutic Systems: Introduction of ImplantDocument16 pagesImplantable Therapeutic Systems: Introduction of ImplantUma MaheswararaoNo ratings yet
- Controlled Release Drug Formulation in Pharmaceuticals: A Study On Their Application and PropertiesDocument17 pagesControlled Release Drug Formulation in Pharmaceuticals: A Study On Their Application and PropertiesintanNo ratings yet
- YyyyDocument12 pagesYyyyRohan SharmaNo ratings yet
- A Prolonged Release Parenteral Drug Delivery SystemDocument11 pagesA Prolonged Release Parenteral Drug Delivery SystemronnymcmNo ratings yet
- Introduction To PharmacologyDocument50 pagesIntroduction To PharmacologyAbdishakour Hassa.100% (1)
- Assigment Controlled Drug Delivery SystemDocument5 pagesAssigment Controlled Drug Delivery SystemZainab AbdullahiNo ratings yet
- Mechanism of Implantable Drug Delivery SystemsDocument48 pagesMechanism of Implantable Drug Delivery SystemsTanveer AhmedNo ratings yet
- Practical 2Document5 pagesPractical 2Arooj FatimaNo ratings yet
- Historical Perspective of CDDSDocument3 pagesHistorical Perspective of CDDSHemant BhattNo ratings yet
- 4 RJPDFT 10 4 2018Document13 pages4 RJPDFT 10 4 2018Fransisco AlfredoNo ratings yet
- 1 - Pendahuluan - Drug Delivery Systems-09 2016Document26 pages1 - Pendahuluan - Drug Delivery Systems-09 2016Kos KosasihNo ratings yet
- Atrigel A Potential Parenteral Controlled Drug Delivery SystemDocument8 pagesAtrigel A Potential Parenteral Controlled Drug Delivery SystemMaria RoswitaNo ratings yet
- Ijps258 269Document12 pagesIjps258 269Kristine Dwi PuspitasariNo ratings yet
- 4 - Drug Product Design ParametersDocument7 pages4 - Drug Product Design ParametersVinz AlvarezNo ratings yet
- NDDS (BP704) IDocument22 pagesNDDS (BP704) Ihasan.aliNo ratings yet
- NDDS AnswersDocument56 pagesNDDS AnswersPrajwal PatankarNo ratings yet
- Chapter 1Document32 pagesChapter 1Czerwin JualesNo ratings yet
- Unit One of PharmacologyDocument63 pagesUnit One of PharmacologyAbdinaasir MohamedNo ratings yet
- Controlled Drug DeliveryDocument23 pagesControlled Drug DeliveryAnburaj JamesNo ratings yet
- Biopharm 2Document3 pagesBiopharm 2muzzamiluswaNo ratings yet
- AbsorptionDocument84 pagesAbsorptionDr. Bharat JainNo ratings yet
- Diploma EEE DocumentDocument72 pagesDiploma EEE DocumentJaganMohanGuduruNo ratings yet
- تصميم كويزDocument73 pagesتصميم كويزHemo HindiNo ratings yet
- Brahmakar - Biopharmaceutics & PharmacokineticsDocument374 pagesBrahmakar - Biopharmaceutics & PharmacokineticsSamritiNo ratings yet
- PumpsOsmotic-Duros Osmotic Implant For HumansDocument15 pagesPumpsOsmotic-Duros Osmotic Implant For Humansomar100% (1)
- Biopharmaceutics - 1 2022Document24 pagesBiopharmaceutics - 1 2022Varshini VarshaNo ratings yet
- Gupta Kumar - Nano Meningkatkan BA DLLDocument40 pagesGupta Kumar - Nano Meningkatkan BA DLLHesti HariantiNo ratings yet
- What Is PharmacologyDocument5 pagesWhat Is PharmacologyShardendu MishraNo ratings yet
- Review On Immediate Drug Released Dosage FormDocument8 pagesReview On Immediate Drug Released Dosage FormEditor IJTSRDNo ratings yet
- New Era University: Pharmacology For MidwiferyDocument11 pagesNew Era University: Pharmacology For MidwiferyHarriegail O. LontocNo ratings yet
- Topical Drug DeliveryDocument21 pagesTopical Drug DeliveryhappyNo ratings yet
- Document 2Document9 pagesDocument 2zoha fatimaNo ratings yet
- Article Wjpps 14988056511Document12 pagesArticle Wjpps 14988056511Its MENo ratings yet
- Pharmacokinetics and PharmacodynamicsDocument113 pagesPharmacokinetics and PharmacodynamicsEvelyn MedinaNo ratings yet
- Introduction To Pharmacology: Katzung, Bertram G, Susan B. Masters, and Anthony J. Trevor. Basic & ClinicalDocument40 pagesIntroduction To Pharmacology: Katzung, Bertram G, Susan B. Masters, and Anthony J. Trevor. Basic & Clinicaljamila ilNo ratings yet
- ParenteralDocument4 pagesParenteralreymar.martinez88No ratings yet
- A Prolonged Release Parenteral Drug Delivery System - An OverviewDocument11 pagesA Prolonged Release Parenteral Drug Delivery System - An Overviewcristian135No ratings yet
- SRDDS Matrix TabletDocument17 pagesSRDDS Matrix TabletMISBAH KAUSARNo ratings yet
- 6Document11 pages6UgaugaaNo ratings yet
- Review Article VikashdashDocument4 pagesReview Article VikashdashamjohnnyNo ratings yet
- Parenteral Drug AbsorptionDocument24 pagesParenteral Drug AbsorptionAsnakeNo ratings yet
- 17.alekhya Research ArticleDocument8 pages17.alekhya Research ArticleBaru Chandrasekhar RaoNo ratings yet
- Microneedle-mediated Transdermal and Intradermal Drug DeliveryFrom EverandMicroneedle-mediated Transdermal and Intradermal Drug DeliveryNo ratings yet
- Pharmacology- The Molecular Dance: Understanding Drug Interactions: Harmony and Chaos: The Symphony of Drug InteractionsFrom EverandPharmacology- The Molecular Dance: Understanding Drug Interactions: Harmony and Chaos: The Symphony of Drug InteractionsNo ratings yet
- EthoxDocument24 pagesEthoxAlfredo MéndezNo ratings yet
- H2so4 20% - MSDSDocument6 pagesH2so4 20% - MSDSPhạm Văn HiếuNo ratings yet
- Fluid Flow Assurance Issues Literature ReviewDocument12 pagesFluid Flow Assurance Issues Literature ReviewMatahari SenjaNo ratings yet
- MSDS Calsium OxideDocument6 pagesMSDS Calsium OxidePipit RatnasariNo ratings yet
- Microbiological Beneficiation of Low Grade Manganese Ores: A ReviewDocument21 pagesMicrobiological Beneficiation of Low Grade Manganese Ores: A ReviewSEP-PublisherNo ratings yet
- CREII-Module-4 - Lecture 18 & 19 PDFDocument21 pagesCREII-Module-4 - Lecture 18 & 19 PDFshubhamNo ratings yet
- Earthscience, PPTDocument12 pagesEarthscience, PPTAlaisa Claire Dela TorreNo ratings yet
- Qualitative Analysis NotesDocument1 pageQualitative Analysis NotesNaseema MalikNo ratings yet
- Final Report of The Amended Safety Assessment of Glyceryl LaurateDocument40 pagesFinal Report of The Amended Safety Assessment of Glyceryl LaurateSam SonNo ratings yet
- Slide 1Document68 pagesSlide 1KASPER كاسبرNo ratings yet
- Kemp P H 1969Document278 pagesKemp P H 1969RICARDO DE FREITAS FERNANDES PONTESNo ratings yet
- MIST 2019-2020 QuestionDocument4 pagesMIST 2019-2020 QuestionmackenzieoleoNo ratings yet
- MSDS DIaliser ElisioDocument6 pagesMSDS DIaliser Elisioika setiawatiNo ratings yet
- Separation and Purification of Organic CompoundsDocument8 pagesSeparation and Purification of Organic CompoundsRachel Jean OlarteNo ratings yet
- PiroxicamDocument4 pagesPiroxicamSahil AliNo ratings yet
- ODI-TOX SILVER (Toxin Binder) MSDSDocument4 pagesODI-TOX SILVER (Toxin Binder) MSDSTazia DuldulNo ratings yet
- PT Final Exam Level-II (Specific)Document5 pagesPT Final Exam Level-II (Specific)RohitNo ratings yet
- Parsol Guard-Hoja de Datos (DSM)Document2 pagesParsol Guard-Hoja de Datos (DSM)LuisCastilloCastroNo ratings yet
- Chem LabDocument44 pagesChem LabalbertoNo ratings yet
- Propilparabeno HandbookDocument3 pagesPropilparabeno HandbookCarlos Fernando Jacobo PérezNo ratings yet
- Acrylic Modified Water Soluble Oil Based CoatingsDocument4 pagesAcrylic Modified Water Soluble Oil Based Coatingsichsan hakimNo ratings yet
- Liquid Liquid ExtractionDocument34 pagesLiquid Liquid ExtractionTubagusNo ratings yet
- Gr. 7 Science TG (Q1 To 4)Document224 pagesGr. 7 Science TG (Q1 To 4)Qwyn Vylette Sanson67% (9)
- PRE4122 Exercise No. 4 Imperfections in SolidsDocument9 pagesPRE4122 Exercise No. 4 Imperfections in SolidsعبداللهأحمدNo ratings yet
- SolutionsDocument11 pagesSolutionsBeatriz G. AblayNo ratings yet
- FL SopDocument45 pagesFL SopSara JohnsonNo ratings yet
- Seminar Report On "Water Breakthrough" Submitted To Savitribai Phule Pune UniversityDocument34 pagesSeminar Report On "Water Breakthrough" Submitted To Savitribai Phule Pune UniversityFINAL YEAR PETROLEUM 2020 BATCHNo ratings yet
- CH 1 - Introduction To ChemistryDocument30 pagesCH 1 - Introduction To ChemistryvncntmarlesNo ratings yet
- Biochem Lab ReportDocument4 pagesBiochem Lab ReportChryza Faith QuicoyNo ratings yet
- Industrial Production of L-GlutamineDocument4 pagesIndustrial Production of L-Glutamineedal_108No ratings yet