Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
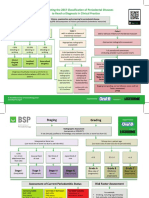
- BSP FlowchartDocument2 pagesBSP FlowchartShahrukh ali khan100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Critical Appraisal Tools and Reporting Guidelines For Evidence-Based PracticeDocument10 pagesCritical Appraisal Tools and Reporting Guidelines For Evidence-Based PracticeSITI KURNIAWATINo ratings yet
- TIDieR Checklist PDFDocument2 pagesTIDieR Checklist PDFTanya TaypeNo ratings yet
- Evaluationand Comparisonofthe Effectof Different Border Molding Materialson 0 AComplete Denture Retention Aniinvivoi StudyDocument7 pagesEvaluationand Comparisonofthe Effectof Different Border Molding Materialson 0 AComplete Denture Retention Aniinvivoi StudyShahrukh ali khanNo ratings yet
- Comparison of Complete Denture Fabricated by Two Different Border Molding Materials, in Terms of Patients' SatisfactionDocument4 pagesComparison of Complete Denture Fabricated by Two Different Border Molding Materials, in Terms of Patients' SatisfactionShahrukh ali khanNo ratings yet
- Complete Denture IntroductionDocument3 pagesComplete Denture IntroductionShahrukh ali khanNo ratings yet
- Staging and GradingDocument4 pagesStaging and GradingShahrukh ali khanNo ratings yet
- Diagnosis and Treatment Planning Part 1Document12 pagesDiagnosis and Treatment Planning Part 1Shahrukh ali khanNo ratings yet
- Effects of Ageing On Edentulous Mouth: BoneDocument6 pagesEffects of Ageing On Edentulous Mouth: BoneShahrukh ali khanNo ratings yet
- Dental Bleaching: Presenter: DR Shahrukh Ali Khan Resident R1 Prosthodontics Aga Khan University, HospitalDocument47 pagesDental Bleaching: Presenter: DR Shahrukh Ali Khan Resident R1 Prosthodontics Aga Khan University, HospitalShahrukh ali khanNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleShahrukh ali khanNo ratings yet
- Clinics in SurgeryDocument5 pagesClinics in SurgeryShahrukh ali khanNo ratings yet
- Common Mistakes in Clinical ResearchDocument6 pagesCommon Mistakes in Clinical ResearchShahrukh ali khanNo ratings yet
- FDS Amp 2020Document140 pagesFDS Amp 2020Shahrukh ali khan100% (1)
- Evaluation of Signs, Symptoms, and Occlusal Factors Among Patients With Temporomandibular Disorders According To Helkimo IndexDocument8 pagesEvaluation of Signs, Symptoms, and Occlusal Factors Among Patients With Temporomandibular Disorders According To Helkimo IndexShahrukh ali khanNo ratings yet
- Bloodborne Pathogens Learner Course Guide: Florida Department of HealthDocument30 pagesBloodborne Pathogens Learner Course Guide: Florida Department of HealthShahrukh ali khanNo ratings yet
- Infection Control in DentistryDocument69 pagesInfection Control in DentistryShahrukh ali khanNo ratings yet
- ارزیابی مقالات کارآزمایی بالینی دارای گروه کنترل تصادفی شده مجله دانشکده دندانپزشکی دانشگاه علوم پزشکی مشهد منتشره از سال 2831 الی2814Document10 pagesارزیابی مقالات کارآزمایی بالینی دارای گروه کنترل تصادفی شده مجله دانشکده دندانپزشکی دانشگاه علوم پزشکی مشهد منتشره از سال 2831 الی2814Majid KarimiNo ratings yet
- Indian Heart JournalDocument18 pagesIndian Heart JournalSanaSofiyahNo ratings yet
- Evidence-Basedprosthodontics: Fundamental Considerations, Limitations, and GuidelinesDocument17 pagesEvidence-Basedprosthodontics: Fundamental Considerations, Limitations, and GuidelinesRohan BhagatNo ratings yet
- CONSORT 2010 Checklist of Information To Include When Reporting A Randomised TrialDocument2 pagesCONSORT 2010 Checklist of Information To Include When Reporting A Randomised TrialAnonymous bbLNsOpAEINo ratings yet
- Journal of Global Antimicrobial ResistanceDocument16 pagesJournal of Global Antimicrobial ResistanceJuan Martín VargasNo ratings yet
- Post Market Clinical Follow Up Studies 1604996252Document17 pagesPost Market Clinical Follow Up Studies 1604996252FVNo ratings yet
- Tullu (2019) - Writing The Title and Abstract For A Research PaperDocument6 pagesTullu (2019) - Writing The Title and Abstract For A Research PaperMaria Inês AzevedoNo ratings yet
- Good Research Practice - 2014-GuidelinesDocument15 pagesGood Research Practice - 2014-GuidelinesGuyver FixNo ratings yet
- A Systematic Review of The Quality of Iv Fluid Therapy in Veterinary MedicineDocument8 pagesA Systematic Review of The Quality of Iv Fluid Therapy in Veterinary MedicineNicol RojasNo ratings yet
- Clinical Effectivieness of Occupational Therapy in Mental Health A Meta-AnalysisDocument9 pagesClinical Effectivieness of Occupational Therapy in Mental Health A Meta-AnalysisGloria Nataly Ramirez Badillo100% (1)
- (JOMI) PFANNANSTIEL 2022 - Reporting Quality of Full Mouth Studies in Implant DentistryDocument35 pages(JOMI) PFANNANSTIEL 2022 - Reporting Quality of Full Mouth Studies in Implant DentistrydrjonduNo ratings yet
- CONSORT Group CONSORT 2010 Statement Updated GuideDocument8 pagesCONSORT Group CONSORT 2010 Statement Updated GuideSmulskii AndriiNo ratings yet
- PLOS ONE Manuscript Guidelines SavedDocument22 pagesPLOS ONE Manuscript Guidelines SavedRicardo GonzalezNo ratings yet
- Materials and Methods in Research PaperDocument6 pagesMaterials and Methods in Research Papergw1m2qtf100% (1)
- How To Write A Scientific Manuscript For PublicatiDocument11 pagesHow To Write A Scientific Manuscript For PublicatiHaile SolomonNo ratings yet
- Computers in Biology and MedicineDocument16 pagesComputers in Biology and MedicineDhanalekshmi YedurkarNo ratings yet
- How To Design and Set Up A Clinical Trial Part 2: Protocols and ApprovalsDocument5 pagesHow To Design and Set Up A Clinical Trial Part 2: Protocols and Approvalsdruzair007No ratings yet
- Introduction To Systematic Review and Meta-Analysis - RN PDFDocument22 pagesIntroduction To Systematic Review and Meta-Analysis - RN PDFAndi sri wahyu putriNo ratings yet
- PDF Ama Manual of Style A Guide For Authors and Editors 11Th Edition Jama Network Editors Ebook Full ChapterDocument53 pagesPDF Ama Manual of Style A Guide For Authors and Editors 11Th Edition Jama Network Editors Ebook Full Chapterjerry.medas487100% (5)
- Econsort GuidelinesDocument5 pagesEconsort GuidelinesHansNo ratings yet
- Penjelasan Consort Utk Artikel KlinisDocument28 pagesPenjelasan Consort Utk Artikel KlinisWitri Septia NingrumNo ratings yet
- Protocol Development and Statistical Analysis PlanDocument40 pagesProtocol Development and Statistical Analysis PlanpalanivelNo ratings yet
- 4 OverviewBrightonMethods Vaccine 2007Document4 pages4 OverviewBrightonMethods Vaccine 2007Simbakutty VenkataramananNo ratings yet
- CASP RCT Checklist Year 2020Document8 pagesCASP RCT Checklist Year 2020Agitha PutriNo ratings yet
- 464 - Surgical Endoscopy - Submission Guidelines 082023Document23 pages464 - Surgical Endoscopy - Submission Guidelines 082023alihumoodhasanNo ratings yet
- APRM ChecklistDocument6 pagesAPRM ChecklistMohd Amiruddin Ag DamitNo ratings yet
- Research On The Use Technology of Nurse EducationDocument16 pagesResearch On The Use Technology of Nurse EducationDina TrisnawatiNo ratings yet
- 15 Portuguese GUIDE FOR SCIENTIFIC WRITING HOW TO AVOID COMMON MISTAKES IN A SCIENTIFIC ARTICLEDocument13 pages15 Portuguese GUIDE FOR SCIENTIFIC WRITING HOW TO AVOID COMMON MISTAKES IN A SCIENTIFIC ARTICLEFernando OrlandoNo ratings yet