Download as pdf or txt
You might also like
- Pterygoid Implant DR Pallavi D YawaleDocument216 pagesPterygoid Implant DR Pallavi D Yawalerajsuresh85100% (4)
- Alveolar BoneDocument59 pagesAlveolar BoneMohammed hisham khan100% (7)
- PDF Textbook of Prosthodontics PDFDocument2 pagesPDF Textbook of Prosthodontics PDFaakriti mahajanNo ratings yet
- 2019 COWELL® Implant Solution v.26 (LR) PDFDocument113 pages2019 COWELL® Implant Solution v.26 (LR) PDFBernythefly axcNo ratings yet
- Dr. Ishita Singhal Mds First YearDocument189 pagesDr. Ishita Singhal Mds First YearDR. ISHITA SINGHALNo ratings yet
- Alveolar BoneDocument25 pagesAlveolar Bonesamar yousif mohamedNo ratings yet
- Musculoskeletal Anatomy and Physiology 4Document67 pagesMusculoskeletal Anatomy and Physiology 4Dennis Nabor Muñoz, RN,RM100% (1)
- Human Anatomy: The Skeletal System: Osseous Tissue and Skeletal StructureDocument71 pagesHuman Anatomy: The Skeletal System: Osseous Tissue and Skeletal StructureLeilaNo ratings yet
- Teaching Series BoneDocument26 pagesTeaching Series BoneNAND KUMARNo ratings yet
- Bone Physiology DR NzauDocument84 pagesBone Physiology DR NzauNzau MuangeNo ratings yet
- Skeletal - System AnatomyDocument130 pagesSkeletal - System Anatomyhamnafaisall8No ratings yet
- MODULE 4 Skeletal SystemDocument16 pagesMODULE 4 Skeletal SystemKate Andrea PanizalesNo ratings yet
- 2020-2021 AP 1 Lecture 6b Skeletal System 1Document16 pages2020-2021 AP 1 Lecture 6b Skeletal System 1OscarJaiNo ratings yet
- General Anatomy: 1. SupportDocument4 pagesGeneral Anatomy: 1. SupportNu Ri LeeNo ratings yet
- Skeletal SystemDocument70 pagesSkeletal SystemHannah Bless SalvadorNo ratings yet
- Oral. H Lec.12Document4 pagesOral. H Lec.12Abdulrahman UdayNo ratings yet
- Skeletal 6Document28 pagesSkeletal 6BSN-2F Neutral Axis SiazonNo ratings yet
- Presentation 3Document15 pagesPresentation 3Anchal RainaNo ratings yet
- Skeletal SystemDocument80 pagesSkeletal SystemElaine Victoria ElizanNo ratings yet
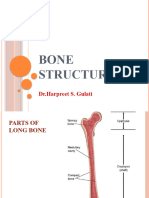
- Bone StructureDocument21 pagesBone Structuresapnakumarigurjar108No ratings yet
- ORTHO-Bone Physiology and Repair (Dr. Gerochi)Document4 pagesORTHO-Bone Physiology and Repair (Dr. Gerochi)Monique BorresNo ratings yet
- Bones: Defination: Bone Is Highly Vascular, Living, Constantly ChangingDocument21 pagesBones: Defination: Bone Is Highly Vascular, Living, Constantly ChangingMd Ahsanuzzaman PinkuNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyDocument3 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyMavic VillanuevaNo ratings yet
- Bone Basic NDocument98 pagesBone Basic NSuraj kumar GuptaNo ratings yet
- Table of ContentDocument52 pagesTable of ContentJasvir SinghNo ratings yet
- CHAPTER 6 ANAPHY TransesDocument13 pagesCHAPTER 6 ANAPHY TransesHoly HaeinNo ratings yet
- Bone TissueDocument46 pagesBone TissueFiraol DiribaNo ratings yet
- ANAPHY Lec Session #5 - SAS (Agdana, Nicole Ken)Document9 pagesANAPHY Lec Session #5 - SAS (Agdana, Nicole Ken)Nicole Ken AgdanaNo ratings yet
- Skeletal SystemDocument14 pagesSkeletal SystemCharlize PalmaNo ratings yet
- (W9) The Skeletal SystemDocument9 pages(W9) The Skeletal SystemReign Heart HayahayNo ratings yet
- Skeletal SystemDocument7 pagesSkeletal Systemopingaangelamae.opingaNo ratings yet
- Module - Skeletal SystemDocument22 pagesModule - Skeletal SystemEller Tacud CollantesNo ratings yet
- Cap 2 Bone As A LivingDocument17 pagesCap 2 Bone As A LivingGaby MayaNo ratings yet
- Dr. Sassia Lecture Bone Histology Part I June 2023Document45 pagesDr. Sassia Lecture Bone Histology Part I June 2023Ali ELKARGHALYNo ratings yet
- Alveolar BoneDocument15 pagesAlveolar Boneamna faridNo ratings yet
- BONE (Histology)Document65 pagesBONE (Histology)fhfebriiNo ratings yet
- Skeletal System: - Composed of The Body's Bones and Associated Ligaments, Tendons, and Cartilages. - FunctionsDocument66 pagesSkeletal System: - Composed of The Body's Bones and Associated Ligaments, Tendons, and Cartilages. - FunctionsDenver TanhuanNo ratings yet
- Lecture Activities No. 6 Skeletal System: Guide Questions AnswersDocument13 pagesLecture Activities No. 6 Skeletal System: Guide Questions AnswersPrancheska Abigayle Peneyra SantiagoNo ratings yet
- 4.2.2. Bone TissueDocument7 pages4.2.2. Bone Tissuealexandra4wineNo ratings yet
- Periodontium NotesDocument12 pagesPeriodontium NotesClarisse Mendoza100% (1)
- CHAPTER 6 ANAPHY TransesDocument13 pagesCHAPTER 6 ANAPHY TransesHoly HaeinNo ratings yet
- W7 - Bone HistologyDocument10 pagesW7 - Bone HistologynhcsmlmolNo ratings yet
- Lecture 22 Bone Physiology IDocument26 pagesLecture 22 Bone Physiology Ijurgen klein-WernerNo ratings yet
- Alveolar BoneDocument23 pagesAlveolar BoneDr Lokesh DaswaniNo ratings yet
- Cartilage and BoneDocument58 pagesCartilage and BoneGer BengNo ratings yet
- BONEDocument36 pagesBONEdrharmainaNo ratings yet
- Alveolar BoneDocument114 pagesAlveolar BoneDent DealsNo ratings yet
- BoneDocument43 pagesBoneKush PathakNo ratings yet
- JointsDocument34 pagesJointsDawood AhmadNo ratings yet
- Alveolar Bone PerioDocument32 pagesAlveolar Bone PerioFourthMolar.com100% (1)
- Bone Is A Mineralized Connective Tissue: Biochemistry DepartmentDocument66 pagesBone Is A Mineralized Connective Tissue: Biochemistry DepartmentYunandhika RizkiNo ratings yet
- Anaphy - Skeletal SystemDocument13 pagesAnaphy - Skeletal SystemYo1No ratings yet
- 7.0 Skeletal SystemDocument45 pages7.0 Skeletal System[R2A] Khadijah Azlan100% (1)
- ALVEOLAR BoneDocument72 pagesALVEOLAR BoneArchana50% (2)
- Skeletal SystemDocument14 pagesSkeletal SystemCharlize PalmaNo ratings yet
- Skeletal System Functions of The Skeletal System: Human Anatomy & Physiology Kylie Jan C. SilvaDocument15 pagesSkeletal System Functions of The Skeletal System: Human Anatomy & Physiology Kylie Jan C. SilvaKert trocioNo ratings yet
- Bone Joints SRA1110Document35 pagesBone Joints SRA1110machonanyasha2005No ratings yet
- The Skeletal SystemDocument7 pagesThe Skeletal SystemKathleenJoyGalAlmasinNo ratings yet
- Bone Tissue & Mascular TissueDocument5 pagesBone Tissue & Mascular TissueJanjan GarcesNo ratings yet
- Bone, Functions, Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandBone, Functions, Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Bone Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandBone Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Advanced farriery knowledge: A study guide and AWCF theory course companionFrom EverandAdvanced farriery knowledge: A study guide and AWCF theory course companionNo ratings yet
- Periodontium NotesDocument12 pagesPeriodontium NotesClarisse Mendoza100% (1)
- Enamel Developmental Stages of A ToothDocument12 pagesEnamel Developmental Stages of A ToothClarisse Mendoza100% (2)
- Development of Palate and Tongue NotesDocument9 pagesDevelopment of Palate and Tongue NotesClarisse MendozaNo ratings yet
- Odontogenesis NotesDocument14 pagesOdontogenesis NotesClarisse Mendoza100% (1)
- 1 11 Dent MatDocument33 pages1 11 Dent MatkrstnkyslNo ratings yet
- AMSTERDAM2022Document9 pagesAMSTERDAM2022Gabriel Filipe Tosin ScivskiNo ratings yet
- SL. NO. Product Packaging GST % New MRP Lowest Retail: Doctor Final PriceDocument5 pagesSL. NO. Product Packaging GST % New MRP Lowest Retail: Doctor Final PriceRohit MuthukumarswamyNo ratings yet
- Root Resorption: DR Brijesh Kumar Singh MDS 2018-21Document37 pagesRoot Resorption: DR Brijesh Kumar Singh MDS 2018-21Brijesh Kumar Singh100% (1)
- A Historical Perspective of Synthetic Ceramic and Traditional Feldspathic PorcelainDocument7 pagesA Historical Perspective of Synthetic Ceramic and Traditional Feldspathic PorcelainCarissaNo ratings yet
- Annexure-I: Revised Rate List Under The West Bengal Health Scheme, 2008 (Notification No. 796-F (MED) Dated 31-01-2011)Document51 pagesAnnexure-I: Revised Rate List Under The West Bengal Health Scheme, 2008 (Notification No. 796-F (MED) Dated 31-01-2011)tanmoyNo ratings yet
- Distraction OsteogenesisDocument141 pagesDistraction OsteogenesisJohan Edward Franklin MarpaungNo ratings yet
- Physical Exam - AppendectomyDocument8 pagesPhysical Exam - Appendectomyirish felixNo ratings yet
- Teeth Development in ChildrenDocument3 pagesTeeth Development in ChildrenCharlie McdonnellNo ratings yet
- UnlEarning Endo 2022 BrouchreDocument17 pagesUnlEarning Endo 2022 Brouchrepawan yadavNo ratings yet
- Effect of Restorative Treatment With Endocrown and Ferrule On TheDocument8 pagesEffect of Restorative Treatment With Endocrown and Ferrule On Theangi trujilloNo ratings yet
- Assessment of Fundamental Knowledge 2011Document10 pagesAssessment of Fundamental Knowledge 2011Neeraj SinghNo ratings yet
- Oral-B Braun 3D Excel Pulsating Toothbrush Manual (Japanese)Document12 pagesOral-B Braun 3D Excel Pulsating Toothbrush Manual (Japanese)mesfaisantNo ratings yet
- Biodata Peneliti 2019Document4 pagesBiodata Peneliti 2019Anyuung SNo ratings yet
- June 1, 2018Document24 pagesJune 1, 2018Strathmore TimesNo ratings yet
- Dental Casting Alloys FinalDocument175 pagesDental Casting Alloys FinalNiaz Ahammed0% (1)
- Variolink Esthetic Brochure 673400Document6 pagesVariolink Esthetic Brochure 673400wuhan lalalaNo ratings yet
- Early Treatment of Class III Malocclusion: Is It Worth The Burden?Document4 pagesEarly Treatment of Class III Malocclusion: Is It Worth The Burden?giselaNo ratings yet
- Daftar Pustaka: Endod 43: 763-8Document6 pagesDaftar Pustaka: Endod 43: 763-8thasyaNo ratings yet
- Hu Friedy Product CatalogDocument548 pagesHu Friedy Product CatalogHayes MaineNo ratings yet
- Gen XT International Catalogue 2014Document44 pagesGen XT International Catalogue 2014haneefmdf0% (1)
- Schallhorn. A Study of The Arbitrary Center and The Kinematic Center of Rotation For Face-Bow Mountings. (1957)Document8 pagesSchallhorn. A Study of The Arbitrary Center and The Kinematic Center of Rotation For Face-Bow Mountings. (1957)Jose Enrique AvilaNo ratings yet
- JGR 4 023Document2 pagesJGR 4 023Kurnia SelaNo ratings yet
- Biodentine Scientific FileDocument32 pagesBiodentine Scientific FileHamdy AlmaghrabyNo ratings yet
- Qdoc - Tips Mcqs in Pediatric Dentistry2pdfDocument359 pagesQdoc - Tips Mcqs in Pediatric Dentistry2pdfFahad SNo ratings yet
- An Historical Overview of Clear Aligner Therapy The Evolution of Clear AlignersDocument8 pagesAn Historical Overview of Clear Aligner Therapy The Evolution of Clear AlignersJean-Philippe MercierNo ratings yet
- Sector Capsule: Oral Care in India: Key Data FindingsDocument3 pagesSector Capsule: Oral Care in India: Key Data FindingsShriniket PatilNo ratings yet