Download as docx, pdf, or txt
You might also like
- Motivation Letter - AMANDA PDFDocument1 pageMotivation Letter - AMANDA PDFamanda100% (1)
- Cancer. Quratulain TariqDocument18 pagesCancer. Quratulain TariqHafiz Shahid1No ratings yet
- Screening and Early Detection: Issues For Older AdultsDocument9 pagesScreening and Early Detection: Issues For Older AdultsinelNo ratings yet
- Jurnal ColostomyDocument8 pagesJurnal ColostomyVerticha IndahmutNo ratings yet
- Cancer Screening: Dr. Waqar MunirDocument26 pagesCancer Screening: Dr. Waqar MunirWaqar MunirNo ratings yet
- Module 1 Epidemiology Anatomy and Physiology of The Cell CarcinogenesisDocument38 pagesModule 1 Epidemiology Anatomy and Physiology of The Cell CarcinogenesisAlessandra MercadoNo ratings yet
- Koko's Project 2 Submitted WorkDocument50 pagesKoko's Project 2 Submitted WorkNlemorusa PaschalineNo ratings yet
- Cancer Screening - Health Impact, Prevalence, Correlates and InterventionsDocument38 pagesCancer Screening - Health Impact, Prevalence, Correlates and InterventionsMary OvbieboNo ratings yet
- 2011 Article 342Document4 pages2011 Article 342Gilang IrwansyahNo ratings yet
- National Cancer Institute Tumor Markers Fact SheetDocument4 pagesNational Cancer Institute Tumor Markers Fact SheetJit KarjeeNo ratings yet
- Growing Burden of Cancer Cases in India - Overview On Causes and Types of CancerDocument7 pagesGrowing Burden of Cancer Cases in India - Overview On Causes and Types of CancerBISHAL KUMAR PATRONo ratings yet
- NURS 530 Prostate CancerDocument7 pagesNURS 530 Prostate CancerVivian OcampoNo ratings yet
- How to Prevent Prostate Problems: A Complete Guide to the Essentials of Prostate HealthFrom EverandHow to Prevent Prostate Problems: A Complete Guide to the Essentials of Prostate HealthNo ratings yet
- Prostate Cancer Early Detection, Diagnosis, and StagingDocument39 pagesProstate Cancer Early Detection, Diagnosis, and StagingLuis AcevedoNo ratings yet
- Colorectal Cancer Screening in An Equal Access Healthcare SystemDocument11 pagesColorectal Cancer Screening in An Equal Access Healthcare SystemTri Rahma Yani YawatiNo ratings yet
- Cancer Volume 77 Issue 2 1996Document7 pagesCancer Volume 77 Issue 2 1996BiancaTCNo ratings yet
- PROSTATE CANCER (Class 12th Project)Document26 pagesPROSTATE CANCER (Class 12th Project)RahulNo ratings yet
- Analytic Hierarchy Process in An Online QuestionnaireDocument84 pagesAnalytic Hierarchy Process in An Online QuestionnaireUlianti UmurahNo ratings yet
- Effective Cancer Detection Using Soft Computing TechniqueDocument5 pagesEffective Cancer Detection Using Soft Computing TechniqueInternational Organization of Scientific Research (IOSR)No ratings yet
- Prostate Cancer Screening: Are We There Yet?: March 2010 Andrew M.D. Wolf, MD University of Virginia School of MedicineDocument48 pagesProstate Cancer Screening: Are We There Yet?: March 2010 Andrew M.D. Wolf, MD University of Virginia School of Medicineibrunom3No ratings yet
- Effect of Cancer On Prostates All Over The WorldDocument42 pagesEffect of Cancer On Prostates All Over The WorldRahulNo ratings yet
- Ovarian Cancer ThesisDocument8 pagesOvarian Cancer ThesisDon Dooley100% (1)
- Active Surveillance For Prostate Cancer AUA Update 33 2008Document8 pagesActive Surveillance For Prostate Cancer AUA Update 33 2008moetazNo ratings yet
- Incidence Mortality Survival and Prognostic AnalysDocument15 pagesIncidence Mortality Survival and Prognostic AnalyslhykaNo ratings yet
- CA Prostate by Dr. Musaib MushtaqDocument71 pagesCA Prostate by Dr. Musaib MushtaqDr. Musaib MushtaqNo ratings yet
- Assignment of Prostate Cancer by Adel Khalil PDFDocument18 pagesAssignment of Prostate Cancer by Adel Khalil PDFعادل خليلNo ratings yet
- Thyroid Cancer Early Detection, Diagnosis, and StagingDocument24 pagesThyroid Cancer Early Detection, Diagnosis, and StagingDao Trung HaiNo ratings yet
- Article Review: Disease and Economic Burden of Prostate Cancer in Malaysia: A ReviewDocument8 pagesArticle Review: Disease and Economic Burden of Prostate Cancer in Malaysia: A ReviewMeiselAdeliaNo ratings yet
- Example of Research Paper About CancerDocument8 pagesExample of Research Paper About Cancerjuzel0zupis3100% (1)
- 1785-Article Text-3218-1-10-20210529Document11 pages1785-Article Text-3218-1-10-20210529Megersa RaseNo ratings yet
- Noncommunicable Diseases: What Is The Burden of Non Communicable Disease?Document9 pagesNoncommunicable Diseases: What Is The Burden of Non Communicable Disease?Nanda MaulaniNo ratings yet
- Research Paper Colorectal CancerDocument4 pagesResearch Paper Colorectal Cancerxactrjwgf100% (1)
- Common Cancer Types Among Men: Published: Wednesday, August 17, 2011 00:00 Written By: People's JournalDocument5 pagesCommon Cancer Types Among Men: Published: Wednesday, August 17, 2011 00:00 Written By: People's JournalIbrahim RegachoNo ratings yet
- Cancer UnderstandingsDocument2 pagesCancer UnderstandingsSteicy MorgadoNo ratings yet
- Cummings Et Al-2014-The Journal of PathologyDocument9 pagesCummings Et Al-2014-The Journal of Pathologyalicia1990No ratings yet
- Gut 2011 Morris 806 13Document9 pagesGut 2011 Morris 806 13568563No ratings yet
- Nurses As Cancer InsurgentsDocument7 pagesNurses As Cancer InsurgentsNick RealinoNo ratings yet
- Philippine Cancer Control Program - Llamas, Lomod, ParajesDocument39 pagesPhilippine Cancer Control Program - Llamas, Lomod, ParajesSHIELOU LOMODNo ratings yet
- DaskivichAnnalsManuscript 1Document27 pagesDaskivichAnnalsManuscript 1Southern California Public RadioNo ratings yet
- Current Cancer Screening IssuesDocument44 pagesCurrent Cancer Screening IssuesNational Press FoundationNo ratings yet
- CANCER UPDATE Clinical Stem Cell Document - Alex Mou & Ryan TangDocument7 pagesCANCER UPDATE Clinical Stem Cell Document - Alex Mou & Ryan Tangalexmou2008No ratings yet
- Impact of Comorbidities and Age On Cause-Speci Fic Mortality in Postmenopausal Patients With Breast CancerDocument8 pagesImpact of Comorbidities and Age On Cause-Speci Fic Mortality in Postmenopausal Patients With Breast Cancersmithkelsey244No ratings yet
- Nej Mo A 1201637Document11 pagesNej Mo A 1201637GianNo ratings yet
- Prostate Cancer, 2nd Ed. by Anne KatzDocument317 pagesProstate Cancer, 2nd Ed. by Anne Katzkrisz.vorosNo ratings yet
- Name of Student Name of Instructor Course ID DateDocument18 pagesName of Student Name of Instructor Course ID DateNeelam shahzadiNo ratings yet
- CHE 101 Term PaperDocument16 pagesCHE 101 Term PaperFuzail KhanNo ratings yet
- Analisis Kanser Prostat MalaysiaDocument13 pagesAnalisis Kanser Prostat MalaysiaMuhammad AimanNo ratings yet
- Jus 160003Document12 pagesJus 160003Jose NestaresNo ratings yet
- Cancer .Document11 pagesCancer .Bushra ZafarNo ratings yet
- What To Know About CancerDocument17 pagesWhat To Know About CancerKARL PASCUANo ratings yet
- A Foe With Many FacesDocument2 pagesA Foe With Many FacesJuan TamaniNo ratings yet
- Brief: Ovarian Cancers: Evolving Paradigms in Research and CareDocument4 pagesBrief: Ovarian Cancers: Evolving Paradigms in Research and CareFrancesco MultinuNo ratings yet
- Lifestyle and Dietary Factors in The Prevention of Lethal Prostate CancerDocument10 pagesLifestyle and Dietary Factors in The Prevention of Lethal Prostate CancerDale MckinneyNo ratings yet
- Bowel Cancer: Cancer Because It Is A Cancer of Either Rectum or Colon or Sometimes ItDocument8 pagesBowel Cancer: Cancer Because It Is A Cancer of Either Rectum or Colon or Sometimes Itnoor fatimaNo ratings yet
- Screeningforcancer: Whentostop?: A Practical Guide and Review of The EvidenceDocument14 pagesScreeningforcancer: Whentostop?: A Practical Guide and Review of The EvidenceMohamedRashadNo ratings yet
- Filipou - 2016Document4 pagesFilipou - 2016TurboNo ratings yet
- 1-Tumor Markers - National Cancer InstituteDocument5 pages1-Tumor Markers - National Cancer InstituteAhmed Abd El AzizNo ratings yet
- Prostate Cancer Between Prognosis and Adequate/proper TherapyDocument8 pagesProstate Cancer Between Prognosis and Adequate/proper TherapyGabriel NguyenNo ratings yet
- ESC Focused Guidelines Acute and Chronic Heart FailureDocument13 pagesESC Focused Guidelines Acute and Chronic Heart FailureSergio Mora CanelaNo ratings yet
- Nursing Care Plan: Subjective Data " GoalDocument2 pagesNursing Care Plan: Subjective Data " GoalJay VillasotoNo ratings yet
- Experience On Nutrient Focus Approach in EthiopiaDocument12 pagesExperience On Nutrient Focus Approach in EthiopiaRado RamaholimihajaNo ratings yet
- Kidus FinalDocument51 pagesKidus Finalselam zewdu assefaNo ratings yet
- I. Topic: Pertussis II. ObjectivesDocument7 pagesI. Topic: Pertussis II. ObjectivesKaren PanganibanNo ratings yet
- Report of Examination of A Female Victim of Sexual Assault: History Related To The Incident (As Stated by SubjectDocument3 pagesReport of Examination of A Female Victim of Sexual Assault: History Related To The Incident (As Stated by SubjectKashishNo ratings yet
- Goboy - Risk For Infection NCPDocument3 pagesGoboy - Risk For Infection NCPLouise GermaineNo ratings yet
- MGR University Nursing Dissertation TopicsDocument8 pagesMGR University Nursing Dissertation TopicsHowToWriteMyPaperOmaha100% (1)
- IMS World ReviewDocument15 pagesIMS World ReviewRakesh ShivranNo ratings yet
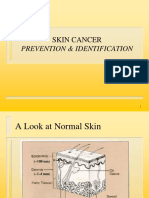
- Prevention & Identification: Skin CancerDocument25 pagesPrevention & Identification: Skin Cancermkman100% (1)
- Risk Register Peralatan Medik 2022Document8 pagesRisk Register Peralatan Medik 2022maintenance anmedNo ratings yet
- Job Hazard Analysis RiskassessmentDocument4 pagesJob Hazard Analysis RiskassessmentJunard M. Lu HapNo ratings yet
- Universiti Teknologi Mara: Confidential 1 LG/FEB 2017/ELC231/ELC230Document9 pagesUniversiti Teknologi Mara: Confidential 1 LG/FEB 2017/ELC231/ELC230YASMINNo ratings yet
- University of Liverpool India Fellowships ProgrammeDocument6 pagesUniversity of Liverpool India Fellowships ProgrammeShashank BansalNo ratings yet
- Pain Management Clinical Guidelinesv2 PDFDocument15 pagesPain Management Clinical Guidelinesv2 PDFErwin Novia Rachmawati100% (1)
- Pharmacy Management SystemDocument4 pagesPharmacy Management SystemTaniya FernandoNo ratings yet
- Diabetes Melittus 12Document19 pagesDiabetes Melittus 12mnmrznNo ratings yet
- Contoh Soal UkomDocument13 pagesContoh Soal Ukomtotok0% (1)
- Schedule of Duty Form: Baguio General Hospital and Medical CenterDocument3 pagesSchedule of Duty Form: Baguio General Hospital and Medical CenterVALERIANO MACARIONo ratings yet
- Certifacte For Solo ParentDocument1 pageCertifacte For Solo Parentsan nicolas 2nd betis guagua pampangaNo ratings yet
- BAS 213 Food ChemistryDocument1 pageBAS 213 Food ChemistrySamiksha SinghNo ratings yet
- Clinical Teaching: On A Modern ApproachDocument11 pagesClinical Teaching: On A Modern ApproachMay JuneNo ratings yet
- Preventing Stunting in ChildrenDocument4 pagesPreventing Stunting in Childrenadkhiatul muslihatinNo ratings yet
- Case Study: Rocio'S HospitalDocument7 pagesCase Study: Rocio'S HospitalMubasher ZardadNo ratings yet
- Surgical Antibiotic Prophylaxis Duration Position Statement October 2021 v1Document3 pagesSurgical Antibiotic Prophylaxis Duration Position Statement October 2021 v1debby twonabilaNo ratings yet
- Mindfulness and PsychotherapyDocument6 pagesMindfulness and Psychotherapyameera kNo ratings yet
- P1 Facts About AnencephalyDocument8 pagesP1 Facts About AnencephalyAde Cahyo IslamiNo ratings yet
- 213 PDFDocument5 pages213 PDFYanine Borda MuñozNo ratings yet
- Fs 2 Chapter 7 Silorioruel.dDocument22 pagesFs 2 Chapter 7 Silorioruel.dNeliza SalcedoNo ratings yet