Download as pdf or txt
You might also like
- The Real Science Behind Why The COVID Vaccines Are Destroying Organ Function - Dangers of The Spike ProteinDocument40 pagesThe Real Science Behind Why The COVID Vaccines Are Destroying Organ Function - Dangers of The Spike ProteinMara Rebeka Herzog100% (7)
- RedmanDocument8 pagesRedmanJaqueline AguilarNo ratings yet
- Paper Importante MartinDocument8 pagesPaper Importante MartinJony CostaNo ratings yet
- Treatment of Electrolyte Disorders in Adult Patients in The Intensive Care UnitDocument21 pagesTreatment of Electrolyte Disorders in Adult Patients in The Intensive Care UnitBuat TugasNo ratings yet
- Indirect Calorimetry - An Indispensable Tool To Understand and Predict ObesityDocument5 pagesIndirect Calorimetry - An Indispensable Tool To Understand and Predict ObesityRodrigo CastilloNo ratings yet
- How Strongly Does Appetite Counter Weight Loss. Quantification of The Feedback Control of Human Energy IntakeDocument18 pagesHow Strongly Does Appetite Counter Weight Loss. Quantification of The Feedback Control of Human Energy IntakeClaudia GuimarãesNo ratings yet
- KTV Kidney in PressDocument6 pagesKTV Kidney in PressVanessaNo ratings yet
- Long-Term Changes in Energy Expenditure and Body Composition After Massive Weight Loss Induced by Gastric Bypass SurgeryDocument9 pagesLong-Term Changes in Energy Expenditure and Body Composition After Massive Weight Loss Induced by Gastric Bypass SurgeryJavier VegaNo ratings yet
- Nejm199503093321001 PDFDocument8 pagesNejm199503093321001 PDFAle TabaskoNo ratings yet
- Evidence For The Existence of Adaptive Thermogenesis During Weight Loss PDFDocument9 pagesEvidence For The Existence of Adaptive Thermogenesis During Weight Loss PDFAle TabaskoNo ratings yet
- Evidence For The Existence of Adaptive Thermogenesis During Weight LossDocument9 pagesEvidence For The Existence of Adaptive Thermogenesis During Weight LossJaime GonzálezNo ratings yet
- Cachexia in Cancer PatientDocument6 pagesCachexia in Cancer PatientLeni LukmanNo ratings yet
- Jurnal FisikaDocument7 pagesJurnal FisikaKezia HanaraNo ratings yet
- Dennis 2009Document8 pagesDennis 2009Retta CatherinaNo ratings yet
- Armstrong - Hydration Biomarkers and Dietary FluidDocument6 pagesArmstrong - Hydration Biomarkers and Dietary FluidAngieda SoepartoNo ratings yet
- Camps Et Al., 2015 - AT and Metabolic AdaptationDocument8 pagesCamps Et Al., 2015 - AT and Metabolic AdaptationJulia SCNo ratings yet
- Jcinvest00131 0160Document10 pagesJcinvest00131 0160Sarah OctaviaNo ratings yet
- PIIS240545772100245XDocument5 pagesPIIS240545772100245Xsulemi castañonNo ratings yet
- Hypocaloric, High-Protein Nutrition Therapy For Critically Ill Patients With ObesityDocument7 pagesHypocaloric, High-Protein Nutrition Therapy For Critically Ill Patients With ObesityStacey WoodsNo ratings yet
- Ajcn122044 PDFDocument10 pagesAjcn122044 PDFRizky LumalessilNo ratings yet
- Alternate-Day Fasting in Nonobese Subjects: Effects On Body Weight, Body Composition, and Energy MetabolismDocument5 pagesAlternate-Day Fasting in Nonobese Subjects: Effects On Body Weight, Body Composition, and Energy MetabolismCem Tunaboylu (Student)No ratings yet
- 10 1109@icecct 2015 7226135Document7 pages10 1109@icecct 2015 7226135ishupaNo ratings yet
- Weight-Loss Diets For The Prevention and Treatment of ObesityDocument3 pagesWeight-Loss Diets For The Prevention and Treatment of ObesityRupita SitanggangNo ratings yet
- Colloid Normalizes Resuscitation Ratio in Pediatric BurnsDocument7 pagesColloid Normalizes Resuscitation Ratio in Pediatric BurnsLaura Valentina Lopez HerreraNo ratings yet
- Artigo Women at Altitude Carbohydrate Utilization Vduring Exercise at 4,300 MDocument11 pagesArtigo Women at Altitude Carbohydrate Utilization Vduring Exercise at 4,300 MCíntia AnibalNo ratings yet
- The Effects of Intermittent Energy - Antoni 2014Document24 pagesThe Effects of Intermittent Energy - Antoni 2014Fer GominaNo ratings yet
- Aumento Plasmático Dos Poluentes Advém Da Lipólise Subcutânea - IJO - 01Document7 pagesAumento Plasmático Dos Poluentes Advém Da Lipólise Subcutânea - IJO - 01Elenice Peltz NutricionistaNo ratings yet
- 1 s2.0 S0271531720305467 MainDocument9 pages1 s2.0 S0271531720305467 MainNurullita AishaNo ratings yet
- Jci37385 PDFDocument13 pagesJci37385 PDFNur Ahmad HabibiNo ratings yet
- Effects of Intermittent and Continuous Calorie Restriction On Body Weight and Metabolism Over 50 WK: A Randomized Controlled TrialDocument13 pagesEffects of Intermittent and Continuous Calorie Restriction On Body Weight and Metabolism Over 50 WK: A Randomized Controlled TrialSarah OctaviaNo ratings yet
- Effects of A Low Carbohydrate Diet On Energy Expenditure During Weight Loss Maintenance: Randomized TrialDocument14 pagesEffects of A Low Carbohydrate Diet On Energy Expenditure During Weight Loss Maintenance: Randomized TrialNenden ApriliyantiNo ratings yet
- Can Additional Water A Day Keep The Cysts Away, in Patients With Polycystic Kidney DiseaseDocument3 pagesCan Additional Water A Day Keep The Cysts Away, in Patients With Polycystic Kidney DiseaseEmmanuel HernandezNo ratings yet
- 2020 Han. The Benefits of Combining Water and Land-Based TherapyDocument8 pages2020 Han. The Benefits of Combining Water and Land-Based TherapyNathalia Bakes TeodoroNo ratings yet
- Human Colonic Microbiota Associated With Diet ObesDocument6 pagesHuman Colonic Microbiota Associated With Diet ObesHéctor GalvánNo ratings yet
- Negative Impact of Hypocaloric Feeding and Energy Balance On Clinical Outcome in ICU PatientsDocument8 pagesNegative Impact of Hypocaloric Feeding and Energy Balance On Clinical Outcome in ICU PatientsDaniela HernandezNo ratings yet
- Obesity - 2016 - Fothergill - Persistent Metabolic Adaptation 6 Years After The Biggest Loser CompetitionDocument8 pagesObesity - 2016 - Fothergill - Persistent Metabolic Adaptation 6 Years After The Biggest Loser Competitionpablo.s4672No ratings yet
- Nutrition & Metabolism: Energy Expenditure in Chow-Fed Female Non-Human Primates of Various WeightsDocument11 pagesNutrition & Metabolism: Energy Expenditure in Chow-Fed Female Non-Human Primates of Various WeightsAnindira RustandiNo ratings yet
- The Use of Bioimpedance Spectroscopy To Guide Fluid Management in Patients Receiving DialysisDocument7 pagesThe Use of Bioimpedance Spectroscopy To Guide Fluid Management in Patients Receiving Dialysisnelbut2No ratings yet
- Gut Environ GenomicsDocument6 pagesGut Environ GenomicsDra Tábitha Menezes de LimaNo ratings yet
- Basal Energy Expenditure, Resting Energy Expenditure and One Metabolic Equivalent (1 MET) Values For Young Chinese Adults With Different Body WeightsDocument7 pagesBasal Energy Expenditure, Resting Energy Expenditure and One Metabolic Equivalent (1 MET) Values For Young Chinese Adults With Different Body WeightsIrhamna FauziahNo ratings yet
- Exercise For Weight LossDocument2 pagesExercise For Weight LosssimachewNo ratings yet
- !!! Oxidative Priority Meal Frequency and The Energy EDocument12 pages!!! Oxidative Priority Meal Frequency and The Energy EJohnny RockermeierNo ratings yet
- Basal Metabolic Rate Studies in Humans MeasurementDocument21 pagesBasal Metabolic Rate Studies in Humans MeasurementAdrizal RamadhanNo ratings yet
- Basal Metabolic Rate Studies in Humans: Measurement and Development of New EquationsDocument21 pagesBasal Metabolic Rate Studies in Humans: Measurement and Development of New EquationsGinNo ratings yet
- Nutrition - Parenteral 2Document16 pagesNutrition - Parenteral 2Guillaume michiganNo ratings yet
- What Is ObesityDocument2 pagesWhat Is ObesityhandikaNo ratings yet
- NeatDocument3 pagesNeatapi-302659596No ratings yet
- Energy Expenditure and Nutritional Status of Coal Miners: A Cross-Sectional StudyDocument9 pagesEnergy Expenditure and Nutritional Status of Coal Miners: A Cross-Sectional StudyTâm LươngNo ratings yet
- Dietary Assessment in Whitehall II: Comparison of 7 D Diet Diary and Food-Frequency Questionnaire and Validity Against BiomarkersDocument10 pagesDietary Assessment in Whitehall II: Comparison of 7 D Diet Diary and Food-Frequency Questionnaire and Validity Against BiomarkersGiuseppe Peppuz VersariNo ratings yet
- Relationship Between Fructose Content of A NormalDocument1 pageRelationship Between Fructose Content of A NormalZebraNo ratings yet
- 10 1210@clinem@dgaa336 PDFDocument37 pages10 1210@clinem@dgaa336 PDFAuliya BintanNo ratings yet
- Spectroscopic Analysis of Water Treated by and in Proximity To Energy - 10.1016@j.explore.2020.10.005Document12 pagesSpectroscopic Analysis of Water Treated by and in Proximity To Energy - 10.1016@j.explore.2020.10.005koffeekommandoNo ratings yet
- The Cafeteria Diet - As A Tool For Studies of ThermogenesisDocument4 pagesThe Cafeteria Diet - As A Tool For Studies of ThermogenesisRodrigoNo ratings yet
- Lesson 1 Back To Basics Estimating Energy Requirements Foradult Hospital PatientsDocument8 pagesLesson 1 Back To Basics Estimating Energy Requirements Foradult Hospital PatientsBalireddy NeeharikaNo ratings yet
- Bouchard (1983) A Method To Asses Energy Expenditure in Children and AdultsDocument8 pagesBouchard (1983) A Method To Asses Energy Expenditure in Children and AdultsGrigorina MitrofanNo ratings yet
- Gasto Energético e Alteração Na Composição Corporal Após A Dieta Cetogênica IsocalóricaDocument10 pagesGasto Energético e Alteração Na Composição Corporal Após A Dieta Cetogênica Isocalóricaqmatheusq wsantoswNo ratings yet
- Calorie For Calorie, Dietary Fat Restriction Results in More Body Fat Loss Than Carbohydrate Restriction in People With ObesityDocument11 pagesCalorie For Calorie, Dietary Fat Restriction Results in More Body Fat Loss Than Carbohydrate Restriction in People With Obesityines.queiros.nutricionistaNo ratings yet
- 2004 - KYLE Et Al - Bioelectrical Impedance Analysis - Review of Principles and Methods (Parte II)Document24 pages2004 - KYLE Et Al - Bioelectrical Impedance Analysis - Review of Principles and Methods (Parte II)Daniel Tavares de AndradeNo ratings yet
- Bridging The Worlds of Research and Policy MakingDocument2 pagesBridging The Worlds of Research and Policy Makingsazzad suvroNo ratings yet
- Fluid and Electrolytes in Pediatrics: A Comprehensive HandbookFrom EverandFluid and Electrolytes in Pediatrics: A Comprehensive HandbookNo ratings yet
- Gastroparesis: A Comprehensive Approach to Evaluation and ManagementFrom EverandGastroparesis: A Comprehensive Approach to Evaluation and ManagementAnna IbeleNo ratings yet
- Snach+e+Clean+Weightlifting Movements From Full Extension The.2015 SCJDocument4 pagesSnach+e+Clean+Weightlifting Movements From Full Extension The.2015 SCJSheilani MartinsNo ratings yet
- Starting at The Ground Up Range of Motion.9Document12 pagesStarting at The Ground Up Range of Motion.9Sheilani MartinsNo ratings yet
- Infographic Progressing Rehabilitation After InjurDocument2 pagesInfographic Progressing Rehabilitation After InjurSheilani MartinsNo ratings yet
- Intervalo Combinado de Sprint, Pliométrico e Treinamento de Força em Jogadores de Futebol Adolescentes Efeitos Nas Medidas de Velocidade, Força, Potência, Mudança de Direção e Capacidade AnaeróbiaDocument12 pagesIntervalo Combinado de Sprint, Pliométrico e Treinamento de Força em Jogadores de Futebol Adolescentes Efeitos Nas Medidas de Velocidade, Força, Potência, Mudança de Direção e Capacidade AnaeróbiaSheilani MartinsNo ratings yet
- The Assisted Nordic Hamstring Curl: Exercise TechniqueDocument4 pagesThe Assisted Nordic Hamstring Curl: Exercise TechniqueSheilani MartinsNo ratings yet
- Síndrome de Compressão TorácicaDocument4 pagesSíndrome de Compressão TorácicaSheilani MartinsNo ratings yet
- Síndrome de Compressão Torácica 2Document8 pagesSíndrome de Compressão Torácica 2Sheilani MartinsNo ratings yet
- Flexibility Training ConceptsDocument20 pagesFlexibility Training ConceptsSheilani MartinsNo ratings yet
- Studyprotocol Open Access: Alexandra Hott, Sigurd Liavaag, Niels Gunnar Juel and Jens Ivar BroxDocument8 pagesStudyprotocol Open Access: Alexandra Hott, Sigurd Liavaag, Niels Gunnar Juel and Jens Ivar BroxSheilani MartinsNo ratings yet
- Capacidade de Sprints Repetidos Parte I - Fatores Que Contribuem para A FadigaDocument23 pagesCapacidade de Sprints Repetidos Parte I - Fatores Que Contribuem para A FadigaSheilani MartinsNo ratings yet
- Capacidade de Sprints Repetidos - Onde EstamosDocument5 pagesCapacidade de Sprints Repetidos - Onde EstamosSheilani MartinsNo ratings yet
- 2014 Pasiakosetal - SportsMed CDocument22 pages2014 Pasiakosetal - SportsMed CSheilani MartinsNo ratings yet
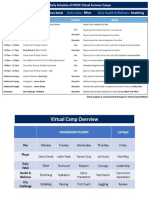
- Sample Daily Schedule Virtual CampDocument2 pagesSample Daily Schedule Virtual CampSheilani MartinsNo ratings yet
- Variation in Barbell Position Relative To Shoulder and Foot Anatomical Landmarks Alters Movement EfficiencyDocument13 pagesVariation in Barbell Position Relative To Shoulder and Foot Anatomical Landmarks Alters Movement EfficiencySheilani MartinsNo ratings yet
- Journal: Periodization: Period or Question Mark?Document4 pagesJournal: Periodization: Period or Question Mark?Sheilani MartinsNo ratings yet
- WHO HSE GCR 2015.13 EngDocument65 pagesWHO HSE GCR 2015.13 EngPuneet MehtaNo ratings yet
- Obstructive Renal Cyst in A Dog - Ultrasonography-GuidedTreatment Using Puncture Aspiration and Injectionwith 95% EthanolDocument3 pagesObstructive Renal Cyst in A Dog - Ultrasonography-GuidedTreatment Using Puncture Aspiration and Injectionwith 95% EthanolIngrid RamisaNo ratings yet
- Wastewater Characteristics: Table 7.1.5 Table 7.1.6Document4 pagesWastewater Characteristics: Table 7.1.5 Table 7.1.6Amin EnviroNo ratings yet
- Section 5 - E&A Drawings PDFDocument1,288 pagesSection 5 - E&A Drawings PDFAndrii PodgornyiNo ratings yet
- WWI 29th Infantry DivisionDocument89 pagesWWI 29th Infantry DivisionCAP History LibraryNo ratings yet
- B20B 6X4 AdtDocument297 pagesB20B 6X4 AdtHANNESNo ratings yet
- Rom, Eprom, & Eeprom Technology: Figure 9-1. Read Only Memory SchematicDocument14 pagesRom, Eprom, & Eeprom Technology: Figure 9-1. Read Only Memory SchematicVu LeNo ratings yet
- 1T 19-20 LBYKM31 Experiment Manual As of Sept 15 2019Document33 pages1T 19-20 LBYKM31 Experiment Manual As of Sept 15 2019Ammi PinedaNo ratings yet
- Veeam Top 10 Reasons Choose Veeam 9 5Document2 pagesVeeam Top 10 Reasons Choose Veeam 9 5Anonymous xKgV3e6XLNo ratings yet
- Chap 002Document50 pagesChap 002Eduardo AndradersNo ratings yet
- Alternating Current and VoltageDocument5 pagesAlternating Current and VoltageRohit SahuNo ratings yet
- TPC-1071H - 1271H - 1571H - 1771H - User Manual - Ed3Document88 pagesTPC-1071H - 1271H - 1571H - 1771H - User Manual - Ed3DeniMestiWidiantoNo ratings yet
- Candle Making: Grace P. TeaňoDocument19 pagesCandle Making: Grace P. TeaňoNoeson TecsonNo ratings yet
- First Long Test in SPS 7Document3 pagesFirst Long Test in SPS 7Dennmark IgutNo ratings yet
- DILO SF6 Catalogue 2021 ENDocument214 pagesDILO SF6 Catalogue 2021 ENBadraa BatorgilNo ratings yet
- Ratio Detector: SNSCT 16Ec304-Communication Theory Unit-3 K.Sumathi, Ap/EceDocument2 pagesRatio Detector: SNSCT 16Ec304-Communication Theory Unit-3 K.Sumathi, Ap/EceChandu NanduNo ratings yet
- Janma Vighatika GrahaDocument5 pagesJanma Vighatika Grahatimsmith1081574No ratings yet
- Ultrasound Beamforming and Image Formation: Mark L. Palmeri, M.D., Ph.D. Biomedical Engineering Duke UniversityDocument50 pagesUltrasound Beamforming and Image Formation: Mark L. Palmeri, M.D., Ph.D. Biomedical Engineering Duke UniversitydeepberaNo ratings yet
- The Learners Demonstrate An Understanding of Some Important Properties of SolutionsDocument4 pagesThe Learners Demonstrate An Understanding of Some Important Properties of Solutionsjennelyn malaynoNo ratings yet
- PVZ - Aradiya Toys - CattailDocument18 pagesPVZ - Aradiya Toys - CattailTallita Alves OliveiraNo ratings yet
- Ice Cream Frozen Dessrt PDFDocument145 pagesIce Cream Frozen Dessrt PDFSreelekshmi LechuNo ratings yet
- Cross FluteDocument6 pagesCross FluteAvicena AlbiruniNo ratings yet
- Fracture CrurisDocument44 pagesFracture CrurisAnonymous turPUJtErNo ratings yet
- Brosur 3M Web ProsesDocument34 pagesBrosur 3M Web ProsesRoni YunusNo ratings yet
- Tábua de Maré - Dezembro 2023Document1 pageTábua de Maré - Dezembro 2023gustavo alvesNo ratings yet
- Ajay Kumar Shukla - CVDocument6 pagesAjay Kumar Shukla - CVdkannanapkNo ratings yet
- Blouse Body Measurement ChartDocument2 pagesBlouse Body Measurement ChartScarletBeauty Enriquez-DiagbelNo ratings yet
- Indian Railways Carbon EmissionsDocument9 pagesIndian Railways Carbon EmissionsTechTrip IndiaNo ratings yet
- Operating Instructions Mechanical Temperature Switches ML1H, MT1H, L2H, T2H, L1X/L1X-EX, T1X/T1X-EX, T2X/T2X-EXDocument8 pagesOperating Instructions Mechanical Temperature Switches ML1H, MT1H, L2H, T2H, L1X/L1X-EX, T1X/T1X-EX, T2X/T2X-EXمحمد فرحاتNo ratings yet