Download as pdf or txt
You might also like
- Jason Cafer MD - Julianna Link PA-C - Cafer's Psychopharmacology - Visualize To Memorize 270 Medication Mascots - Libgen - LiDocument304 pagesJason Cafer MD - Julianna Link PA-C - Cafer's Psychopharmacology - Visualize To Memorize 270 Medication Mascots - Libgen - LiElectric Amoeba100% (7)
- Clinical Manual of Child and Adolescent PsychopharmacologyDocument194 pagesClinical Manual of Child and Adolescent PsychopharmacologyDanielFernandoJaramilloNo ratings yet
- Substance Use Disorders - OpioidsDocument41 pagesSubstance Use Disorders - Opioidsmaggykariuki002No ratings yet
- Opioids: Addiction and TreatmentsDocument20 pagesOpioids: Addiction and TreatmentsrinaviadrinririnNo ratings yet
- Vivitrol TreatmentDocument8 pagesVivitrol TreatmentHarish RathodNo ratings yet
- Opioid Withdrawal in The Emergency Setting - UpToDateDocument15 pagesOpioid Withdrawal in The Emergency Setting - UpToDateSanti HerreraNo ratings yet
- Opioid Withdrawal in AdolescentsDocument21 pagesOpioid Withdrawal in Adolescentsmayteveronica1000No ratings yet
- Drug of AbuseDocument20 pagesDrug of AbuseMaysoun AtoumNo ratings yet
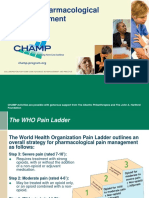
- Review WHOPainLadder OpioidsandNonOpioidsDocument13 pagesReview WHOPainLadder OpioidsandNonOpioidsamajida fadia rNo ratings yet
- Substance Related DisorderDocument35 pagesSubstance Related Disorderزينب عيسىNo ratings yet
- Pi Is 0001209211012464Document11 pagesPi Is 0001209211012464Micca MikNo ratings yet
- Medication Assisted Treatment 9-21-20121Document6 pagesMedication Assisted Treatment 9-21-20121GodstruthNo ratings yet
- TPPM 2019 7 104Document9 pagesTPPM 2019 7 104Wiwit AsariNo ratings yet
- Ans 8 Analgesic DrugsDocument32 pagesAns 8 Analgesic Drugsyounas63No ratings yet
- The Key To Freeing Your Life From AddictionDocument22 pagesThe Key To Freeing Your Life From AddictionBrainyBlondieNo ratings yet
- Drug Used in Geriatrics: Vrushali Neve Asst. Professor Pharmacology Dept. KGRDCP & RI, KarjatDocument18 pagesDrug Used in Geriatrics: Vrushali Neve Asst. Professor Pharmacology Dept. KGRDCP & RI, KarjatVaibhav ThoratNo ratings yet
- Managing Opioid Withdrawal With BuprenorphineDocument7 pagesManaging Opioid Withdrawal With BuprenorphineAgata KurniawatyNo ratings yet
- Guía de OpioidesDocument13 pagesGuía de OpioidesJAIME MUÑOZNo ratings yet
- Opioid Dependence: Joseph J. Benich IIIDocument12 pagesOpioid Dependence: Joseph J. Benich IIIValentina Londoño CadavidNo ratings yet
- New Zealand Data Sheet: OXYNORM® Capsules OXYNORM® Oral SolutionDocument14 pagesNew Zealand Data Sheet: OXYNORM® Capsules OXYNORM® Oral SolutionFranz Josef TariganNo ratings yet
- Hospital Formulary: Astralis Medical GroupDocument36 pagesHospital Formulary: Astralis Medical GroupJade MBNo ratings yet
- Chapter 1: IntroductionDocument27 pagesChapter 1: IntroductionkevinNo ratings yet
- Rokacet Rokacet PlusDocument11 pagesRokacet Rokacet PlusNaomie bocobzaNo ratings yet
- Drug Interaction of Dental DrugsDocument14 pagesDrug Interaction of Dental DrugsAnubhuti SabhlokNo ratings yet
- Opioid WithdrawalDocument6 pagesOpioid Withdrawalhasan jamiNo ratings yet
- Opioid Potentiators MemoDocument5 pagesOpioid Potentiators MemomattiaNo ratings yet
- ZOMORPH Capsules 10mgDocument6 pagesZOMORPH Capsules 10mgFlorexan Malanday PasonNo ratings yet
- Principles of Opioid Management: Symptom GuidelinesDocument45 pagesPrinciples of Opioid Management: Symptom GuidelinesTheresia Avila KurniaNo ratings yet
- Clinical AssignmentDocument22 pagesClinical AssignmentKeziah GillNo ratings yet
- Ondasentron TraducirDocument3 pagesOndasentron Traducirdayanita1221No ratings yet
- Ondasentron TraducirDocument3 pagesOndasentron Traducirdayanita1221No ratings yet
- Pharma 2014Document34 pagesPharma 2014backupuoload85No ratings yet
- Clinical Pocket Guide Tapering-ADocument4 pagesClinical Pocket Guide Tapering-Alarst06No ratings yet
- Opioid Analgesic S: Click To Edit Master Subtitle StyleDocument59 pagesOpioid Analgesic S: Click To Edit Master Subtitle StyleFatma Felix MayugiNo ratings yet
- OpioidsDocument4 pagesOpioidsdr.anuthomas14No ratings yet
- Opiod AnalgesicsDocument13 pagesOpiod Analgesicschebetnaomi945No ratings yet
- Geriatrics Department BookDocument69 pagesGeriatrics Department BookHazemAbu-BakrNo ratings yet
- Pharmacology - Opioids - The Lecturio Online Medical LibraryDocument10 pagesPharmacology - Opioids - The Lecturio Online Medical Libraryjean PiedraNo ratings yet
- Pedo Seminar - Analgesics and Antibiotics Used in ChildrenDocument44 pagesPedo Seminar - Analgesics and Antibiotics Used in ChildrenPuneet ChoudharyNo ratings yet
- 23 - Pharma. - د. شامل 7Document10 pages23 - Pharma. - د. شامل 7Hassan AdnanNo ratings yet
- Articaine (Septocaine) : Mu-Opioid Receptors Are in A Family of G-Protein Coupled ReceptorsDocument30 pagesArticaine (Septocaine) : Mu-Opioid Receptors Are in A Family of G-Protein Coupled ReceptorsphamnhuchauphuongNo ratings yet
- Opiod Analgesics &antagonistsDocument58 pagesOpiod Analgesics &antagonistsVictoria ChepkorirNo ratings yet
- Practice Standard: Safe Prescribing of Opioids and SedativesDocument4 pagesPractice Standard: Safe Prescribing of Opioids and SedativesSteve GreenNo ratings yet
- 10 TH Conf Poly PharmacyDocument5 pages10 TH Conf Poly Pharmacytr14niNo ratings yet
- Opioid Analgesics & Antagonists: Dr. Hayder B Sahib Ph.D. PharmacologyDocument47 pagesOpioid Analgesics & Antagonists: Dr. Hayder B Sahib Ph.D. Pharmacologyarham pirachaNo ratings yet
- Prescribing Guidelines For Geriatric PatientsDocument17 pagesPrescribing Guidelines For Geriatric PatientsDrVinod Kumar Goud Vemula100% (1)
- Research Paper On CodeineDocument6 pagesResearch Paper On Codeineefkm3yz9100% (1)
- Factors Modifying Drug EffectDocument43 pagesFactors Modifying Drug EffectSunil100% (4)
- Pharmacological Treatment of Respiratory DisordersDocument8 pagesPharmacological Treatment of Respiratory DisorderssaraiNo ratings yet
- Opioids AnalgesicDocument1 pageOpioids AnalgesicAbhay SagarNo ratings yet
- Otc Template Pi CodeineDocument4 pagesOtc Template Pi Codeinegopi nathNo ratings yet
- Drug Ons: AdverseDocument5 pagesDrug Ons: AdverseMisty CheifNo ratings yet
- Pharma Gujjjju IndiaDocument241 pagesPharma Gujjjju IndiaHarsh NimavatNo ratings yet
- Pharma Unit 3 2022 MidtermDocument57 pagesPharma Unit 3 2022 MidtermJohn Dave V. VillarmenteNo ratings yet
- NICEDocument5 pagesNICEJuliaNo ratings yet
- AntiepilepticsDocument13 pagesAntiepilepticstbuyinza21apNo ratings yet
- PharmacologyDocument156 pagesPharmacologyElvis MasigaNo ratings yet
- Opioid Analgesics: Dosage Instructions, Side-Effects, Contra-Indications and WarningsDocument6 pagesOpioid Analgesics: Dosage Instructions, Side-Effects, Contra-Indications and WarningsteddypolNo ratings yet
- AN ALTERNATIVE TO CODEINE AND HYDROCODONE - Management of Persistent CoughDocument2 pagesAN ALTERNATIVE TO CODEINE AND HYDROCODONE - Management of Persistent CoughAnna LiachenkoNo ratings yet
- Chronic Obstructive Pulmonary Disease Case Study: QuestionsDocument7 pagesChronic Obstructive Pulmonary Disease Case Study: QuestionsMohammad KhalaylahNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Opioid Use Disorders:: Therapeutic Manuals for Healing and RecuperationFrom EverandOpioid Use Disorders:: Therapeutic Manuals for Healing and RecuperationNo ratings yet
- SMCLK SJMC 09 2020 PDFDocument102 pagesSMCLK SJMC 09 2020 PDFMarina JankovicNo ratings yet
- Jurnal Farmakogenomik 1Document19 pagesJurnal Farmakogenomik 1WikaNo ratings yet
- 8 Principles of Drug Metabolism, With An Emphasis On Psychiatric DrugsDocument32 pages8 Principles of Drug Metabolism, With An Emphasis On Psychiatric Drugstaro0% (1)
- Clinical Pharmacokinetics of FluoxetineDocument14 pagesClinical Pharmacokinetics of FluoxetinePalwasha MalikNo ratings yet
- Cytochrome P450 PharmacogeneticsDocument3 pagesCytochrome P450 PharmacogeneticsSiegfriedCristoforNo ratings yet
- Classics in Chemical Neuroscience: ChlorpromazineDocument10 pagesClassics in Chemical Neuroscience: ChlorpromazineLisa MariaNo ratings yet
- AmphetaminesDocument39 pagesAmphetaminesRonie Alvarez MaldonadoNo ratings yet
- FDA DDI Guidance 2012Document79 pagesFDA DDI Guidance 2012gshgssgNo ratings yet
- 7-Pediatric - Drug TherapyDocument42 pages7-Pediatric - Drug TherapyDyn Adriani100% (1)
- ACD/Percepta: Overview of The ModulesDocument91 pagesACD/Percepta: Overview of The ModulesTinto J AlencherryNo ratings yet
- Forensic Science International: Frank Musshoff, Ulrike M. Stamer, Burkhard MadeaDocument10 pagesForensic Science International: Frank Musshoff, Ulrike M. Stamer, Burkhard MadeaFakhry FathaniyNo ratings yet
- Invega SustennaDocument33 pagesInvega SustennammoslemNo ratings yet
- Dosage Form For Personalized Medicine: HistoryDocument11 pagesDosage Form For Personalized Medicine: HistoryNayeema KhowserNo ratings yet
- Antifungal ClassDocument25 pagesAntifungal ClassRifa AudinaNo ratings yet
- Chirality in Clinical PracticeDocument7 pagesChirality in Clinical Practicepb_ncNo ratings yet
- Farmacologia Del TramalDocument45 pagesFarmacologia Del TramalJenni Paola CarvajalinoNo ratings yet
- April RN 2021Document35 pagesApril RN 2021Irshad AhamadNo ratings yet
- 3 Biomedicine The Profession DMPK Lena Gustavsson 2015 FinalDocument50 pages3 Biomedicine The Profession DMPK Lena Gustavsson 2015 FinalJayrine MonteroNo ratings yet
- AmitriptylineDocument9 pagesAmitriptylinetrimi68No ratings yet
- TrisDocument48 pagesTrisisgaydioNo ratings yet
- Mario A. Dicato, Eric Van Cutsem - Side Effects of Medical Cancer Therapy (2018, Springer International Publishing) PDFDocument512 pagesMario A. Dicato, Eric Van Cutsem - Side Effects of Medical Cancer Therapy (2018, Springer International Publishing) PDFTatiana100% (1)
- Chemo in ChildrenDocument24 pagesChemo in ChildrenMuhammadFaisalNo ratings yet
- TDM Clinic Guide PDFDocument5 pagesTDM Clinic Guide PDFamalNo ratings yet
- Drug InteractionsDocument11 pagesDrug InteractionssamNo ratings yet
- Pharmacogenomics: Current Status and Future PerspectivesDocument13 pagesPharmacogenomics: Current Status and Future PerspectivesSergio VillicañaNo ratings yet
- Pharmacogenetics Drug Drug Interactions1Document16 pagesPharmacogenetics Drug Drug Interactions1Marfu'ah Mar'ahNo ratings yet
- Factors Affecting Inter Individual Variations in Drug ResponseDocument10 pagesFactors Affecting Inter Individual Variations in Drug Responsehumera50% (4)
- Abstracts Pharmacology 2010Document234 pagesAbstracts Pharmacology 2010Escoazul EscozulNo ratings yet