Download as pdf or txt
You might also like
- Soap Note 5.0Document4 pagesSoap Note 5.0Paulus IskandarNo ratings yet
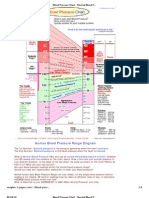
- Blood Pressure ChartDocument4 pagesBlood Pressure ChartPixelateNo ratings yet
- AnginaDocument8 pagesAnginabagusindra1111No ratings yet
- The Association Between Nonalcoholic Fatty Liver Disease and Stroke: Results From The Korean Genome and Epidemiology Study (Koges)Document11 pagesThe Association Between Nonalcoholic Fatty Liver Disease and Stroke: Results From The Korean Genome and Epidemiology Study (Koges)winnerfromparisNo ratings yet
- DEVOTEDocument9 pagesDEVOTEDZGR NNNo ratings yet
- Serum Concentrations of Adiponectin and Risk of Type 2 Diabetes Mellitus and Coronary Heart Disease in Apparently Healthy Middle-Aged MenDocument15 pagesSerum Concentrations of Adiponectin and Risk of Type 2 Diabetes Mellitus and Coronary Heart Disease in Apparently Healthy Middle-Aged MenEcha MagungNo ratings yet
- Thiazolidinediones and Cardiovascular Outcomes in Older Patients With DiabetesDocument10 pagesThiazolidinediones and Cardiovascular Outcomes in Older Patients With Diabetesivel1506No ratings yet
- Effects of Candesartan and Amlodipine On Cardiovascular Events in Hypertensive Patients With Chronic Kidney DiseaseDocument8 pagesEffects of Candesartan and Amlodipine On Cardiovascular Events in Hypertensive Patients With Chronic Kidney Diseasenova sorayaNo ratings yet
- Nida - Lipid Profiles and Postprandial GlucoseDocument7 pagesNida - Lipid Profiles and Postprandial GlucoseSepty KawaiNo ratings yet
- Postgradmedj 96 525Document5 pagesPostgradmedj 96 525Huda TrisenaNo ratings yet
- Human C-Reactive Protein and The Metabolic SyndromeDocument13 pagesHuman C-Reactive Protein and The Metabolic SyndromeEmir SaricNo ratings yet
- (03241750 - Acta Medica Bulgarica) Cardiovascular Risk in Type 2 Diabetic Patients With Asymptomatic Hyperuricemia and GoutDocument8 pages(03241750 - Acta Medica Bulgarica) Cardiovascular Risk in Type 2 Diabetic Patients With Asymptomatic Hyperuricemia and GoutTeodorNo ratings yet
- CKD HT 3Document8 pagesCKD HT 3Peer TutorNo ratings yet
- Diabetes, Glycemic Control, and New-Onset Heart Failure in Patients With Stable Coronary Artery DiseaseDocument6 pagesDiabetes, Glycemic Control, and New-Onset Heart Failure in Patients With Stable Coronary Artery DiseaseAMADA122No ratings yet
- Einarson 2018Document19 pagesEinarson 2018Nikola Dragicka DragicevicNo ratings yet
- 2019 Article 612Document17 pages2019 Article 612Asad NawazNo ratings yet
- TMP 37 D9Document8 pagesTMP 37 D9FrontiersNo ratings yet
- Journal of Diabetes and Its ComplicationsDocument7 pagesJournal of Diabetes and Its ComplicationsOanna ChippNo ratings yet
- Dci 210017Document3 pagesDci 210017Gloria WuNo ratings yet
- Prevalence of Cardiovascular Disease in Type 2 DiaDocument20 pagesPrevalence of Cardiovascular Disease in Type 2 Diasaifadin khalilNo ratings yet
- Determinants of Coronary Heart Disease Among Adults: A Case-Control StudyDocument12 pagesDeterminants of Coronary Heart Disease Among Adults: A Case-Control StudyDewa KrisdiantoNo ratings yet
- Role of Hypertension and Obesity As Risk Factors For IhdDocument5 pagesRole of Hypertension and Obesity As Risk Factors For IhdMohammad Mujtaba GhaffariNo ratings yet
- DIAB41598 - 2021 - Article - 88593 9Document12 pagesDIAB41598 - 2021 - Article - 88593 9marsim92No ratings yet
- HipertensionDocument21 pagesHipertensionGrupo 3737No ratings yet
- Total Lipid Profile Levels As BdjasDocument12 pagesTotal Lipid Profile Levels As BdjasAnonymous tG35SYROzENo ratings yet
- JurdingDocument7 pagesJurdingsiti hazard aldinaNo ratings yet
- Content ServerDocument11 pagesContent Server沈尚諭No ratings yet
- Jcem 3448Document9 pagesJcem 3448Keenan JaquesNo ratings yet
- 1 s2.0 S000291491730807X MainDocument11 pages1 s2.0 S000291491730807X MainEndru AngelNo ratings yet
- Effect of Age On Mortality, Hospitalizations and Response To Digoxin in Patients With Heart Failure: The DIG StudyDocument8 pagesEffect of Age On Mortality, Hospitalizations and Response To Digoxin in Patients With Heart Failure: The DIG StudyHadi KuriryNo ratings yet
- Ijms-22-00287Document10 pagesIjms-22-00287vidhi parekhNo ratings yet
- Framingham Risk Score SaDocument8 pagesFramingham Risk Score Saapi-301624030No ratings yet
- Cardiovascular Safety Profile of Currently Available Diabetic DrugsDocument17 pagesCardiovascular Safety Profile of Currently Available Diabetic Drugsvina_nursyaidahNo ratings yet
- The Year in Cardiology 2013: Cardiovascular Disease PreventionDocument6 pagesThe Year in Cardiology 2013: Cardiovascular Disease PreventionVincent LivandyNo ratings yet
- Association of Proteinuria and Incident Atrial Fibrillation in Patients With Diabetes Mellitus: A Population Based Senior Cohort StudyDocument10 pagesAssociation of Proteinuria and Incident Atrial Fibrillation in Patients With Diabetes Mellitus: A Population Based Senior Cohort StudydrkhengkiNo ratings yet
- 2359 4802 Ijcs 34 05 s01 0012.x98175Document10 pages2359 4802 Ijcs 34 05 s01 0012.x98175Suryati HusinNo ratings yet
- Prospective Study of Fasting Blood Glucose and Intracerebral Hemorrhagic RiskDocument7 pagesProspective Study of Fasting Blood Glucose and Intracerebral Hemorrhagic Riskhidayatul rahmoNo ratings yet
- Nam 2011Document6 pagesNam 2011Ahmed AnwarNo ratings yet
- Low-Density Lipoprotein Cholesterol and Risk of Intracerebral HemorrhageDocument14 pagesLow-Density Lipoprotein Cholesterol and Risk of Intracerebral HemorrhageaghniajolandaNo ratings yet
- Cardiovascular Risk Factors in Patients With Chronic Kidney Disease Under Conservative TreatmentDocument9 pagesCardiovascular Risk Factors in Patients With Chronic Kidney Disease Under Conservative TreatmentTai rascunhos TaiNo ratings yet
- 2017-Taravatmanesh, Et Al-2017 - Determining The Factors Associated With Cardiovascular Disease Recurrence Tehran Lipid and Glucose StudyDocument7 pages2017-Taravatmanesh, Et Al-2017 - Determining The Factors Associated With Cardiovascular Disease Recurrence Tehran Lipid and Glucose Studycipto susiloNo ratings yet
- NephrologyDocument9 pagesNephrologyAGATA M.H KINANTINo ratings yet
- Association Between Metabolic Syndrome and Risk of Cardiovascular Disease, Using Different Criteria and Stratified by SexDocument5 pagesAssociation Between Metabolic Syndrome and Risk of Cardiovascular Disease, Using Different Criteria and Stratified by SexAlfredoNo ratings yet
- Abstracts: Nephrology Dialysis TransplantationDocument1 pageAbstracts: Nephrology Dialysis TransplantationrezkyfikriNo ratings yet
- Pa Nag Iot Akos 2008Document10 pagesPa Nag Iot Akos 2008Chris ChrisNo ratings yet
- 302 Cardiovascular Risk: AssessmentDocument1 page302 Cardiovascular Risk: AssessmentLêHữuHoàiNo ratings yet
- Diastolic Function Is A Strong Predictor of Mortality in Patients With Chronic Kidney DiseaseDocument6 pagesDiastolic Function Is A Strong Predictor of Mortality in Patients With Chronic Kidney DiseasehanifahrafaNo ratings yet
- ImplicationsDocument6 pagesImplicationschandra9000No ratings yet
- Effect of BmiDocument5 pagesEffect of BmiSyaiful Putra RanaNo ratings yet
- Keywords:-Acute Coronary Syndrome, Triglycerides, HighDocument6 pagesKeywords:-Acute Coronary Syndrome, Triglycerides, HighInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Original Article: Study of Myocardial Perfusion in Obese Individuals Without Known Ischemic Heart DiseaseDocument9 pagesOriginal Article: Study of Myocardial Perfusion in Obese Individuals Without Known Ischemic Heart DiseaseCONSTANZA FIGUEROA LOPEZNo ratings yet
- Jurnal 1Document10 pagesJurnal 1fitri juliantiNo ratings yet
- Kanegae 2017Document9 pagesKanegae 2017Kennard Aristo ArifinNo ratings yet
- Diabetes, Glucose Level, and Risk of Sudden Cardiac DeathDocument6 pagesDiabetes, Glucose Level, and Risk of Sudden Cardiac DeathDino DanielNo ratings yet
- CCR 17 E051121189015Document15 pagesCCR 17 E051121189015Paramitha HarmanNo ratings yet
- J of Clinical Hypertension - 2019 - Turana - High Blood Pressure in Dementia How Low Can We GoDocument8 pagesJ of Clinical Hypertension - 2019 - Turana - High Blood Pressure in Dementia How Low Can We GoyudaNo ratings yet
- Adua Et Al-2017-Clinical and Translational MedicineDocument11 pagesAdua Et Al-2017-Clinical and Translational MedicineSam Asamoah SakyiNo ratings yet
- 2001 Relationship of Blood Pressure To 25-Year Mortality Due To Coronary Heart Disease, Cardiovascular Diseases, and All Causes in Young Adult MenDocument8 pages2001 Relationship of Blood Pressure To 25-Year Mortality Due To Coronary Heart Disease, Cardiovascular Diseases, and All Causes in Young Adult MencarlosNo ratings yet
- Hubungan Rasio Trigliserida/High Density Lipoprotein-Cholesterol (TG/HDL-C) Dengan Kejadian Infark Miokard Akut Di RSUP Prof. Dr. R. D. Kandou ManadoDocument5 pagesHubungan Rasio Trigliserida/High Density Lipoprotein-Cholesterol (TG/HDL-C) Dengan Kejadian Infark Miokard Akut Di RSUP Prof. Dr. R. D. Kandou ManadoIvanna NdoenNo ratings yet
- Shinchiro Oshima 2018Document6 pagesShinchiro Oshima 2018Bogdan NeamtuNo ratings yet
- Type 2 Diabetes: Assessing The Relative Risks and Benefits of Glucose-Lowering MedicationsDocument10 pagesType 2 Diabetes: Assessing The Relative Risks and Benefits of Glucose-Lowering MedicationsmosabNo ratings yet
- Plasma Lipids: Optimal Levels for HealthFrom EverandPlasma Lipids: Optimal Levels for HealthAmerican Health FoundationNo ratings yet
- Articulo 6Document6 pagesArticulo 6Gina GuisamanoNo ratings yet
- Platform Abstracts / Journal of Adolescent Health 68 (2021) S20 Es59 S23Document2 pagesPlatform Abstracts / Journal of Adolescent Health 68 (2021) S20 Es59 S23Gina GuisamanoNo ratings yet
- The Journal For Nurse Practitioners: Jacqueline O'Toole, MSC, NP, Irene Gibson, Ma, RGN, Gerard T. Flaherty, MDDocument4 pagesThe Journal For Nurse Practitioners: Jacqueline O'Toole, MSC, NP, Irene Gibson, Ma, RGN, Gerard T. Flaherty, MDGina GuisamanoNo ratings yet
- Public Health: Original ResearchDocument7 pagesPublic Health: Original ResearchGina GuisamanoNo ratings yet
- Hemodynamic Assessment in The Contemporary ICUDocument33 pagesHemodynamic Assessment in The Contemporary ICUnacxit6No ratings yet
- Outcomes - Associated - With - Multiple - Organ - Dysfunctio PDFDocument12 pagesOutcomes - Associated - With - Multiple - Organ - Dysfunctio PDFSultan Rahmat SeptianNo ratings yet
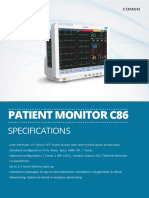
- Patient Monitor C86: SpecificationsDocument4 pagesPatient Monitor C86: SpecificationsBmet ConnectNo ratings yet
- Bio Lab 11Document5 pagesBio Lab 11Sarah JaglalNo ratings yet
- Seminar Hipertensi Dan Komplikasi Kardiovaskular FinalDocument45 pagesSeminar Hipertensi Dan Komplikasi Kardiovaskular FinalbrianNo ratings yet
- JuRnal 6 PDFDocument8 pagesJuRnal 6 PDFNurhajar AzzahraNo ratings yet
- Cardiovascular System SheetDocument11 pagesCardiovascular System SheetBetsy Brown ByersmithNo ratings yet
- Anesthesia MCQDocument13 pagesAnesthesia MCQbouchikhi100% (1)
- 05 N293 35232Document21 pages05 N293 35232Agung RezpectorNo ratings yet
- Prevalence of Hypertension and Associated Risk Factors Among University Students: Comparative StudyDocument9 pagesPrevalence of Hypertension and Associated Risk Factors Among University Students: Comparative StudyChristabella Natalia WijayaNo ratings yet
- SEX DifferencesDocument12 pagesSEX DifferencesSubhashini KNo ratings yet
- USMLE Step 1 in Final YearDocument33 pagesUSMLE Step 1 in Final YearsehrishNo ratings yet
- Imews v2 0 Chart A GenericDocument2 pagesImews v2 0 Chart A GenericdoodrillNo ratings yet
- Cathlab ManualDocument81 pagesCathlab ManualvikrameyeNo ratings yet
- Noor Endocrinologybase. FINALDocument62 pagesNoor Endocrinologybase. FINALschool adressNo ratings yet
- Mindray PM7000 Monitor Service ManualDocument109 pagesMindray PM7000 Monitor Service Manualeduardoquijada100% (1)
- Penatalaksanaan Hipertensi EmergensiDocument10 pagesPenatalaksanaan Hipertensi Emergensimk lawfirmNo ratings yet
- Treatment of Hypertension: JNC 8 and More: Pharmacist'S Letter / Prescriber'S LetterDocument6 pagesTreatment of Hypertension: JNC 8 and More: Pharmacist'S Letter / Prescriber'S LetterJen CanlasNo ratings yet
- 03 Pharmacotherapy Vol 2 Cardiology IIDocument68 pages03 Pharmacotherapy Vol 2 Cardiology IIعلى الجارحىNo ratings yet
- Clinical Notes On The Illness and Death of President Franklin D 1970Document13 pagesClinical Notes On The Illness and Death of President Franklin D 1970Đang Kết NốiNo ratings yet
- Fluid Therapy in Dogs and CatsDocument273 pagesFluid Therapy in Dogs and CatsAgrovet Don BoscoNo ratings yet
- Roe Glucose Conc in Different Blood Compartments 2005Document18 pagesRoe Glucose Conc in Different Blood Compartments 2005jeffnroe1No ratings yet
- Anaesthesia in The Prone PositionDocument19 pagesAnaesthesia in The Prone PositionzaftotNo ratings yet
- Physical Fitness PPT 2023Document124 pagesPhysical Fitness PPT 2023Nati MsbNo ratings yet
- Impact of High Altitude On Cardiovascular Health: Current PerspectivesDocument19 pagesImpact of High Altitude On Cardiovascular Health: Current PerspectivesveronicaNo ratings yet
- HEALTH TEACHING PLAN - HypertensionDocument1 pageHEALTH TEACHING PLAN - HypertensionJasimah GutocNo ratings yet
- Health 2NDDocument21 pagesHealth 2NDJulie AlayonNo ratings yet
- Answer - Fundamentals of Nursing IV: Nursing Process, Physical and Health Assessment and Routine ProceduresDocument15 pagesAnswer - Fundamentals of Nursing IV: Nursing Process, Physical and Health Assessment and Routine ProceduresMae UsquisaNo ratings yet