Download as pdf or txt
You might also like
- IAPD20 Virtual Abstract Book CompressedDocument991 pagesIAPD20 Virtual Abstract Book CompressedAnonymous NqTjEcNo ratings yet
- 101 Black Seed Oil Benefits, Uses & CuresDocument15 pages101 Black Seed Oil Benefits, Uses & CuresAli100% (3)
- AdenomyosisDocument16 pagesAdenomyosisWiwik'RatnaSariPratiwi'100% (2)
- Ajrcccm 2004Document9 pagesAjrcccm 2004kichilla1No ratings yet
- Impact of Prophylactic Continuous Positive Airway Pressure On Transient Tachypnea of The Newborn and Neonatal Intensive Care Admission in Newborns Delivered by Elective Cesarean SectionDocument8 pagesImpact of Prophylactic Continuous Positive Airway Pressure On Transient Tachypnea of The Newborn and Neonatal Intensive Care Admission in Newborns Delivered by Elective Cesarean SectionFabiano SilvaNo ratings yet
- TTNpublicationDocument5 pagesTTNpublicationVerushka CrespoNo ratings yet
- Jurnal Pubme 1 RdsDocument13 pagesJurnal Pubme 1 Rdsriri risna aNo ratings yet
- Australian Critical CareDocument9 pagesAustralian Critical CareLisa MaghfirahNo ratings yet
- 2019 A Phase II Randomized Controlled Trial For Lung and Diaphragm Protective VentilationDocument7 pages2019 A Phase II Randomized Controlled Trial For Lung and Diaphragm Protective VentilationwilsonmauriciolozanoNo ratings yet
- Klebsiella PDFDocument4 pagesKlebsiella PDFOscarEduardoNo ratings yet
- Lung Ultrasound Score As A Predictor of Ventilator Use in Preterm Infants With Dyspnea Within 24 H After Dhospitalization PDFDocument8 pagesLung Ultrasound Score As A Predictor of Ventilator Use in Preterm Infants With Dyspnea Within 24 H After Dhospitalization PDFcesar juarezNo ratings yet
- 1 ChestDocument5 pages1 ChestZakiyah Nur HaqqiNo ratings yet
- Journal NicuDocument4 pagesJournal NicuMargaret LlavorNo ratings yet
- Viral Respiratory Infections in Preterm Infants During andDocument9 pagesViral Respiratory Infections in Preterm Infants During andMariusNo ratings yet
- Risk Factors For Pediatric Extubation FailureDocument17 pagesRisk Factors For Pediatric Extubation FailureFabiola VaniaNo ratings yet
- Background: Corresponding AuthorDocument8 pagesBackground: Corresponding AuthorPratiwi UmbohNo ratings yet
- Clinical Predictors of Radiographic Abnormalities Among Infants With Bronchiolitis in A Paediatric Emergency DepartmentDocument5 pagesClinical Predictors of Radiographic Abnormalities Among Infants With Bronchiolitis in A Paediatric Emergency Departmentnavali rahmaNo ratings yet
- International Consensus On Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations (Costr)Document71 pagesInternational Consensus On Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations (Costr)Dr.Sushree Smita Behura100% (1)
- Buonsenso Et Al-2018-Pediatric PulmonologyDocument9 pagesBuonsenso Et Al-2018-Pediatric Pulmonologywawa chenNo ratings yet
- MD 0000000000012257Document5 pagesMD 0000000000012257Sykat ZamanNo ratings yet
- Journal ReadingDocument5 pagesJournal ReadingRoma WestNo ratings yet
- Articulo ViernesDocument6 pagesArticulo Viernesvelf5No ratings yet
- Umbilical Cord ClampingDocument10 pagesUmbilical Cord ClampingTika WulandariNo ratings yet
- E PDFDocument5 pagesE PDFKarolinaNo ratings yet
- Neonatal PneumoniaDocument8 pagesNeonatal PneumoniaAde Gustina SiahaanNo ratings yet
- Grafica 2 BiennDocument16 pagesGrafica 2 Biennwincu roNo ratings yet
- Dyke 2023 Ped Radiol PREFUL Lung MRI Ventilation NICUDocument9 pagesDyke 2023 Ped Radiol PREFUL Lung MRI Ventilation NICUJonathan DykeNo ratings yet
- Articulo Tesis 9Document8 pagesArticulo Tesis 9Lourdes MarcosNo ratings yet
- Neonatal Lung Ultrasonography To Evaluate Need For Surfactant and Mechanical VentilationDocument8 pagesNeonatal Lung Ultrasonography To Evaluate Need For Surfactant and Mechanical VentilationAlexandra NemesNo ratings yet
- Zgddekzz 23 11 1097Document6 pagesZgddekzz 23 11 1097arieza nur pratamaNo ratings yet
- CJRT 2019 011Document8 pagesCJRT 2019 011Siti HumairahNo ratings yet
- Does Antenatal Corticosteroid Therapy Improve Neonatal Outcomes in Late Preterm Birth?Document8 pagesDoes Antenatal Corticosteroid Therapy Improve Neonatal Outcomes in Late Preterm Birth?faikaoesmaniaNo ratings yet
- Pediatrics 1001 (Final)Document5 pagesPediatrics 1001 (Final)Paul HartingNo ratings yet
- Pi Is 0022347611006548Document7 pagesPi Is 0022347611006548Yudo PrabowoNo ratings yet
- Comparison of Saans Neonatal Continuous Positive Airway PressureDocument6 pagesComparison of Saans Neonatal Continuous Positive Airway Pressureemailtrinaya30No ratings yet
- DANI 2012 - Surfactant Replacement in Preterm Infants With RDSDocument4 pagesDANI 2012 - Surfactant Replacement in Preterm Infants With RDSRafael JustinoNo ratings yet
- Etiological Study of Respiratory Distress in Newborn: Original ResearchDocument5 pagesEtiological Study of Respiratory Distress in Newborn: Original ResearchNovia KurniantiNo ratings yet
- Mechanical Ventilation of The Premature NeonateDocument16 pagesMechanical Ventilation of The Premature NeonateHaitham HafezNo ratings yet
- Relationship Between Oxygenation Index and Extubation Outcome in Neonates Using Mechanical VentilatorDocument6 pagesRelationship Between Oxygenation Index and Extubation Outcome in Neonates Using Mechanical VentilatorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Neonatal Tracheostomy - JonathanWalsh 2018Document12 pagesNeonatal Tracheostomy - JonathanWalsh 2018Ismael Erazo AstudilloNo ratings yet
- Journal Pone 0000192Document5 pagesJournal Pone 0000192TriponiaNo ratings yet
- Respiratory Distress in Term Babies, Can We Predict The Outcome?Document5 pagesRespiratory Distress in Term Babies, Can We Predict The Outcome?Dr. Nimesha GamhewageNo ratings yet
- Wright Et Al 2022 PDFDocument9 pagesWright Et Al 2022 PDFRadu CiprianNo ratings yet
- Use of High-Flow Nasal Cannula Oxygen Therapy To Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate HypoxemiaDocument10 pagesUse of High-Flow Nasal Cannula Oxygen Therapy To Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate HypoxemiaLingga AniNo ratings yet
- A Pilot Prospective Study On Closed Loop Controlled Ventilation and Oxygenation in Ventilated Children During The Weaning PhaseDocument9 pagesA Pilot Prospective Study On Closed Loop Controlled Ventilation and Oxygenation in Ventilated Children During The Weaning PhaseSiti HumairahNo ratings yet
- Causes and Outcomes of Respiratory Distress in NeonatesDocument8 pagesCauses and Outcomes of Respiratory Distress in NeonatesMohammad AlmuhaiminNo ratings yet
- NRDS国教班Document39 pagesNRDS国教班raj patelNo ratings yet
- Paediatrica IndonesianaDocument9 pagesPaediatrica IndonesianaAudina PutriNo ratings yet
- Lauder 2019Document12 pagesLauder 2019Julio AltamiranoNo ratings yet
- SDR Segun EdadDocument9 pagesSDR Segun EdadLuzbenia ChaparroNo ratings yet
- The Role of Delayed Cord Clamping in Improving The Outcome in Preterm BabiesDocument5 pagesThe Role of Delayed Cord Clamping in Improving The Outcome in Preterm BabiesJehangir AllamNo ratings yet
- 5882-PDF Galley-38159-1-10-20201216Document5 pages5882-PDF Galley-38159-1-10-20201216MF SNo ratings yet
- Neonatal Mechanical Ventilation Predictors of Mortality and OutcomesDocument8 pagesNeonatal Mechanical Ventilation Predictors of Mortality and OutcomesAthenaeum Scientific PublishersNo ratings yet
- Gruber2016 PDFDocument4 pagesGruber2016 PDFGiovanni HenryNo ratings yet
- Evaluation of Tracheal Intubations in A Paediatric Intensive Care UnitDocument10 pagesEvaluation of Tracheal Intubations in A Paediatric Intensive Care Unitan.mohammed.maisNo ratings yet
- A Framework For The Management of The Pediatric AirwayDocument23 pagesA Framework For The Management of The Pediatric AirwayDaniel GallegoNo ratings yet
- SPIROMETRYDocument9 pagesSPIROMETRYaeyousefNo ratings yet
- Artigo Ana e Frederico 2021Document10 pagesArtigo Ana e Frederico 2021CarolinaNo ratings yet
- DIT SoniyaRDocument4 pagesDIT SoniyaRLaelannie MagpayoNo ratings yet
- Intjprevmed6133-2704195 004504Document6 pagesIntjprevmed6133-2704195 004504Ade HabibieNo ratings yet
- Short-Acting Sedative-Analgesic Drugs Protect Against Development of Ventilator-Associated Events in Children: Secondary Analysis of The EUVAE StudyDocument8 pagesShort-Acting Sedative-Analgesic Drugs Protect Against Development of Ventilator-Associated Events in Children: Secondary Analysis of The EUVAE StudyevyNo ratings yet
- Doyle & Bradshaw - Sixty Golden MinutesDocument6 pagesDoyle & Bradshaw - Sixty Golden MinutesVillia DamayantieNo ratings yet
- MR Muu STHDocument13 pagesMR Muu STHSiti HumairahNo ratings yet
- CJRT 2019 011Document8 pagesCJRT 2019 011Siti HumairahNo ratings yet
- Assessment of Common Criteria For Awake Extubation in Infants and Young ChildrenDocument8 pagesAssessment of Common Criteria For Awake Extubation in Infants and Young ChildrenSiti HumairahNo ratings yet
- CC 3898Document10 pagesCC 3898Siti HumairahNo ratings yet
- A Pilot Prospective Study On Closed Loop Controlled Ventilation and Oxygenation in Ventilated Children During The Weaning PhaseDocument9 pagesA Pilot Prospective Study On Closed Loop Controlled Ventilation and Oxygenation in Ventilated Children During The Weaning PhaseSiti HumairahNo ratings yet
- Variability of Respiratory Parameters and Extubation Readiness in Ventilated NeonatesDocument6 pagesVariability of Respiratory Parameters and Extubation Readiness in Ventilated NeonatesSiti HumairahNo ratings yet
- Jurnal 4 SNDocument11 pagesJurnal 4 SNSiti HumairahNo ratings yet
- JClinNeonatol73158-3845905 104059Document4 pagesJClinNeonatol73158-3845905 104059Siti HumairahNo ratings yet
- Ocular Trauma: H. Amiruddin, DR., Spm. Rsud Arifin Achmad PekanbaruDocument22 pagesOcular Trauma: H. Amiruddin, DR., Spm. Rsud Arifin Achmad PekanbaruNovasiska Indriyani HutajuluNo ratings yet
- CBSE NCERT Solutions For Class 12 Science Chapter 4: Back of Chapter QuestionsDocument5 pagesCBSE NCERT Solutions For Class 12 Science Chapter 4: Back of Chapter QuestionsSatvik MishraNo ratings yet
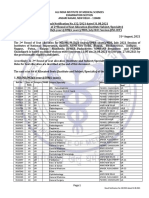
- 2nd Round Seat Allotment Result MDMS MDS Final NET2Document52 pages2nd Round Seat Allotment Result MDMS MDS Final NET2SARKAR JAVED AKHTARNo ratings yet
- TamifluDocument20 pagesTamiflukiwikid718635No ratings yet
- DC Healthy People ReportDocument108 pagesDC Healthy People ReportChristina SturdivantNo ratings yet
- WorldAlzheimerReport2016 PDFDocument140 pagesWorldAlzheimerReport2016 PDFBinod मगरNo ratings yet
- 9 Essential CBT Techniques and Tools PsychotherapyDocument4 pages9 Essential CBT Techniques and Tools Psychotherapyآئمہ توصيف100% (1)
- Sodium Hyaluronate (Hyaluronic Acid) Promotes Migration of Human Corneal Epithelial Cells in VitroDocument2 pagesSodium Hyaluronate (Hyaluronic Acid) Promotes Migration of Human Corneal Epithelial Cells in VitroanamaghfirohNo ratings yet
- Clayton & Willihnganz: Basic Pharmacology For Nurses, 17th EditionDocument4 pagesClayton & Willihnganz: Basic Pharmacology For Nurses, 17th EditionabsianoNo ratings yet
- Contoh Artikel Buk RenoDocument5 pagesContoh Artikel Buk RenoDewita Wulan PratiwiNo ratings yet
- Narrative Report On Second Sem SyllabusDocument92 pagesNarrative Report On Second Sem SyllabusChristine Joy MolinaNo ratings yet
- 2.4.B DR Denni Clinical Evidence of Ribociclib Into Clinical PracticeDocument40 pages2.4.B DR Denni Clinical Evidence of Ribociclib Into Clinical Practicetepat rshsNo ratings yet
- Spine 2019 BrochureDocument10 pagesSpine 2019 BrochureLuciana AliceNo ratings yet
- Vitamin B12 InfographicDocument2 pagesVitamin B12 InfographicIan WynneNo ratings yet
- Report of Anp Icu PostingDocument5 pagesReport of Anp Icu PostingsimonjosanNo ratings yet
- Agents Used in Anemias 2Document25 pagesAgents Used in Anemias 2Raboha TawilNo ratings yet
- Henoch-Schonlein Purpura: An Update: Nutan Kamath, Suchetha RaoDocument7 pagesHenoch-Schonlein Purpura: An Update: Nutan Kamath, Suchetha RaoManjunath VaddambalNo ratings yet
- CurosurDocument2 pagesCurosuredNo ratings yet
- SOMATOM Definition AS Open 20 64 RadOncol PDFDocument20 pagesSOMATOM Definition AS Open 20 64 RadOncol PDFJorge LopezNo ratings yet
- CeftriaxoneDocument2 pagesCeftriaxonegaatgaatNo ratings yet
- Rapport Annuel Santé EuropéenDocument248 pagesRapport Annuel Santé EuropéennouvelobsNo ratings yet
- Paralytic Ileus: Prepared By: Laurence A. Adena, ManDocument43 pagesParalytic Ileus: Prepared By: Laurence A. Adena, ManJanah Beado PagayNo ratings yet
- EosinophiliaDocument8 pagesEosinophiliajohnNo ratings yet
- Terpinen 4 OlDocument8 pagesTerpinen 4 OlDouglas RussellNo ratings yet
- HysterectomyDocument24 pagesHysterectomypt.mahmoudNo ratings yet
- Kgmcta Membership List: Sl. No. Mem. No. Name Department CollegeDocument36 pagesKgmcta Membership List: Sl. No. Mem. No. Name Department CollegekgmctaNo ratings yet
- Fetal Hypoxia 2157 7420.1000e121Document1 pageFetal Hypoxia 2157 7420.1000e121Fian ChristoNo ratings yet