Download as pdf or txt
You might also like
- Search WarrantDocument6 pagesSearch WarrantPat ThomasNo ratings yet
- ASQ Auditing HandbookDocument6 pagesASQ Auditing Handbookpapplion0% (5)
- 2023-12-14 (003) Emergency Motion Prelim InjunctionDocument16 pages2023-12-14 (003) Emergency Motion Prelim InjunctionPat ThomasNo ratings yet
- Benefit Guide Template 3Document18 pagesBenefit Guide Template 3TheChipper1979No ratings yet
- Filarete Treatise On Architecture PDFDocument2 pagesFilarete Treatise On Architecture PDFKelly0% (5)
- Recovery High Schools in Massachusetts: A Promising, Comprehensive Model For Adolescent Substance Abuse and DependenceDocument44 pagesRecovery High Schools in Massachusetts: A Promising, Comprehensive Model For Adolescent Substance Abuse and DependenceThe Stacie Mathewson FoundationNo ratings yet
- IC 13 Guidelines On Standards For High Dependency UnitsDocument4 pagesIC 13 Guidelines On Standards For High Dependency UnitsAnonymous 0WHX7nNo ratings yet
- Unit 10 Safeguarding in Health and Social Care AssignmentDocument16 pagesUnit 10 Safeguarding in Health and Social Care AssignmentAdil Mahmud100% (1)
- Mental Health and COVIDDocument2 pagesMental Health and COVIDRishabh kumarNo ratings yet
- Referral Protocol For Camp ClinicDocument2 pagesReferral Protocol For Camp Clinicmale nurseNo ratings yet
- AP Medical ReportDocument3 pagesAP Medical ReportKatia KatiaNo ratings yet
- Policy Template1Document131 pagesPolicy Template1Jay Raymund Aranas BagasNo ratings yet
- Lassa Fever Final Edited EditedDocument43 pagesLassa Fever Final Edited EditedocmainNo ratings yet
- Periodic Health ExaminationDocument38 pagesPeriodic Health ExaminationHilma NadhifaNo ratings yet
- Nursing in Occupational HealthDocument7 pagesNursing in Occupational HealthjorgeacctNo ratings yet
- Broward County School MemoDocument4 pagesBroward County School MemoChris Vaughn100% (1)
- Occupational Health Hazards and Safety Practices A PDFDocument10 pagesOccupational Health Hazards and Safety Practices A PDFFatima SharminNo ratings yet
- Occupational Health OverviewDocument11 pagesOccupational Health OverviewRidzwan HussainNo ratings yet
- OSHA Workplace Guidance For COVID-19Document35 pagesOSHA Workplace Guidance For COVID-19Todd Prussman100% (2)
- Disability in BangladeshDocument89 pagesDisability in BangladeshArif ShahriarNo ratings yet
- Emotional Impacts of Covid-19 To Medical Practitioners: Unibersidad de ManilaDocument7 pagesEmotional Impacts of Covid-19 To Medical Practitioners: Unibersidad de ManilaJohn Michael Montillano MabiniNo ratings yet
- Drug Awareness and Prevention Program PDFDocument6 pagesDrug Awareness and Prevention Program PDFMarcos Bulay OgNo ratings yet
- Occupational Safety and Health Services: By: Joshua Mar S. MelgarDocument51 pagesOccupational Safety and Health Services: By: Joshua Mar S. MelgarChloe Olazo100% (1)
- Good Shepherd Hospital (Swaziland) TB Infection Control Policy Dec 2014Document30 pagesGood Shepherd Hospital (Swaziland) TB Infection Control Policy Dec 2014COMDIS-HSDNo ratings yet
- Organisational Study Report - Mariyan DivyakarunyalayamDocument5 pagesOrganisational Study Report - Mariyan DivyakarunyalayamBimal AntonyNo ratings yet
- Vanguards of Duty Exploring The Lived Experiences of Healthcare Frontliners During Pandemic SurgeDocument15 pagesVanguards of Duty Exploring The Lived Experiences of Healthcare Frontliners During Pandemic SurgeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Do 208 MH Workplace GuidelinesDocument42 pagesDo 208 MH Workplace GuidelinesxavNo ratings yet
- Executive Summary On Bio-Medical Waste Management: Quantitative Techniques and Research Methods in Management AssignmentDocument5 pagesExecutive Summary On Bio-Medical Waste Management: Quantitative Techniques and Research Methods in Management AssignmentMayuri VarkeyNo ratings yet
- Group ProtocolDocument5 pagesGroup Protocolapi-455072421No ratings yet
- Curriculum MD Forensic MedicineDocument15 pagesCurriculum MD Forensic MedicineAnonymous S0H8cqgnfiNo ratings yet
- Skapinakis Covid 2020Document11 pagesSkapinakis Covid 2020MicMatzNo ratings yet
- Antihypertension Non AdherenceDocument16 pagesAntihypertension Non AdherencebezieNo ratings yet
- VCT ManualDocument70 pagesVCT ManualNay Lin HtikeNo ratings yet
- Public Health Policy - Final Paper Literature Review - Jhorne Bverboncoeur GpantagesDocument12 pagesPublic Health Policy - Final Paper Literature Review - Jhorne Bverboncoeur Gpantagesapi-547155633No ratings yet
- Surgeon General's Workshop On Women's Mental HealthDocument93 pagesSurgeon General's Workshop On Women's Mental HealthHollie1230100% (3)
- Sample-Statement of PurposeDocument5 pagesSample-Statement of PurposeKwame Oppong-PeprahNo ratings yet
- Mental HealthDocument4 pagesMental HealthAhmad Ade aqomuddinNo ratings yet
- Prenatal Health Seeking Behavior of Women in Green Valley Health Center in The Year 2016Document29 pagesPrenatal Health Seeking Behavior of Women in Green Valley Health Center in The Year 2016Grace TayagNo ratings yet
- Sickness ProcedureDocument27 pagesSickness ProcedureRay LeoNo ratings yet
- Importance of Occupational HealthDocument8 pagesImportance of Occupational HealthckopoletoNo ratings yet
- OSH in PhilippinesDocument27 pagesOSH in PhilippinesTOt's VinNo ratings yet
- 12 - Chapter 6 Role of Non-Government Organizations in Disaster ManagementDocument45 pages12 - Chapter 6 Role of Non-Government Organizations in Disaster ManagementMOBLOX100% (1)
- 4140 Philosophy of NursingDocument10 pages4140 Philosophy of Nursingapi-402049640No ratings yet
- Treasury's Covid-19 Economic ScenariosDocument16 pagesTreasury's Covid-19 Economic ScenariosHenry Cooke100% (1)
- 11.initial Assesment & Stabilization of Poly Trauma PatientsDocument7 pages11.initial Assesment & Stabilization of Poly Trauma PatientsmyscribeNo ratings yet
- ICU As High Reliability OrganizationDocument66 pagesICU As High Reliability OrganizationRakhatiar TiarNo ratings yet
- Factors Contributing To Emergence of Hypertension in Diabetic Patients Attending Diabetics Outpatient Clinic in Nyamira CountyDocument27 pagesFactors Contributing To Emergence of Hypertension in Diabetic Patients Attending Diabetics Outpatient Clinic in Nyamira CountyJoshua Mokaya100% (1)
- 42 Global Occupational Health FINALDocument54 pages42 Global Occupational Health FINALIsep Wahyudin100% (2)
- DPCC Mental Health ReportDocument10 pagesDPCC Mental Health ReportWWMTNo ratings yet
- Literature ReviewDocument11 pagesLiterature Reviewapi-437205356No ratings yet
- Bangladesh National Plan For Disaster Management (2016-2020)Document77 pagesBangladesh National Plan For Disaster Management (2016-2020)sh4dow.strid3r9581No ratings yet
- Post Disaster SurveillanceDocument38 pagesPost Disaster SurveillanceAgoez AsiyantoNo ratings yet
- Infection Prevention and Control Manual For Schools and Childcare FacilitiesDocument105 pagesInfection Prevention and Control Manual For Schools and Childcare FacilitiesRose AzuikeNo ratings yet
- 11.2 Baseline Medical Surveillance ProcedureDocument18 pages11.2 Baseline Medical Surveillance ProcedureaceNo ratings yet
- MR-SIA 2023 Rapid-Convenience-Monitoring-RCM-FormDocument2 pagesMR-SIA 2023 Rapid-Convenience-Monitoring-RCM-FormDatu Hoffer RhuNo ratings yet
- Health and Safety ScopeDocument12 pagesHealth and Safety ScopeMuhammad Shahood JamalNo ratings yet
- Planned Teaching On Occupational Health HazardsDocument8 pagesPlanned Teaching On Occupational Health HazardsgandhialpitNo ratings yet
- What Is The Impact of Covid-19 On Safety of Health Care WorkerDocument8 pagesWhat Is The Impact of Covid-19 On Safety of Health Care WorkerChasz Blessing KyaloNo ratings yet
- Therapeutic Relationship: Rubilyn A. Bulquerin-Sumaylo, RN, MSN, LPTDocument24 pagesTherapeutic Relationship: Rubilyn A. Bulquerin-Sumaylo, RN, MSN, LPTRubz BulquerinNo ratings yet
- Clinical Draft PDFDocument62 pagesClinical Draft PDFTapaswini MohantyNo ratings yet
- Occupational Diseases and Health Awareness Through Multimedia: A Case Study Among Women at Risk Employed in Coir Retting in Kerala, IndiaFrom EverandOccupational Diseases and Health Awareness Through Multimedia: A Case Study Among Women at Risk Employed in Coir Retting in Kerala, IndiaNo ratings yet
- House Call: Understanding How Telemedicine is Poised to Transform Healthcare in Rural America and BeyondFrom EverandHouse Call: Understanding How Telemedicine is Poised to Transform Healthcare in Rural America and BeyondNo ratings yet
- Excerpt From Special Message To The Congress On Mental Illness and Mental RetardationDocument3 pagesExcerpt From Special Message To The Congress On Mental Illness and Mental Retardationapi-292360588No ratings yet
- Tim Hugo: Commonwealth of Virginia Ouse of Elegates RichmondDocument3 pagesTim Hugo: Commonwealth of Virginia Ouse of Elegates RichmondPat ThomasNo ratings yet
- Biol Notice AdvisoryDocument1 pageBiol Notice AdvisoryPat ThomasNo ratings yet
- Megan Duffy Contract SummaryDocument1 pageMegan Duffy Contract SummaryPat ThomasNo ratings yet
- Bedford County Use of Force March 2024Document3 pagesBedford County Use of Force March 2024Pat ThomasNo ratings yet
- Report Use of Tony Brown Nov 10 2023Document3 pagesReport Use of Tony Brown Nov 10 2023Pat ThomasNo ratings yet
- Douthat Court OrderDocument3 pagesDouthat Court OrderPat ThomasNo ratings yet
- City of Roanoke Virginia Et Al V Eli Lilly and Company Et Al Vawdce-23-00816 0001.0Document201 pagesCity of Roanoke Virginia Et Al V Eli Lilly and Company Et Al Vawdce-23-00816 0001.0Sam OrlandoNo ratings yet
- Officer Involved Shooting (June 30, 2023) Press ReleaseDocument8 pagesOfficer Involved Shooting (June 30, 2023) Press ReleasePat ThomasNo ratings yet
- 2023-12-14 (003-004) Ex 003 Action Plans P-I Emergency Motion ReducedDocument116 pages2023-12-14 (003-004) Ex 003 Action Plans P-I Emergency Motion ReducedPat ThomasNo ratings yet
- 2023-12-14 (003-003) Ex 002 Notice 95 Ainmals Taken P-I Emergency MotionDocument5 pages2023-12-14 (003-003) Ex 002 Notice 95 Ainmals Taken P-I Emergency MotionPat ThomasNo ratings yet
- Media BurnBan EndedDocument1 pageMedia BurnBan EndedPat ThomasNo ratings yet
- Emergency Declaration-Extension Burn Ban 2023.12 8Document2 pagesEmergency Declaration-Extension Burn Ban 2023.12 8Pat ThomasNo ratings yet
- 2023-12-12 (001-002) Ex 2 Notice of Seizure HearingDocument4 pages2023-12-12 (001-002) Ex 2 Notice of Seizure HearingPat ThomasNo ratings yet
- 95 Animals SeizedDocument5 pages95 Animals SeizedWSLSNo ratings yet
- SCC-ApCo ApprovalDocument8 pagesSCC-ApCo ApprovalPat ThomasNo ratings yet
- FF24 InitialLineupPosterDocument1 pageFF24 InitialLineupPosterPat ThomasNo ratings yet
- Pulaski County Burn BanDocument1 pagePulaski County Burn BanJustin Daniel GearyNo ratings yet
- Notice-Burn Ban LiftedDocument1 pageNotice-Burn Ban LiftedPat ThomasNo ratings yet
- Gun Violence Community AssessmentDocument1 pageGun Violence Community AssessmentPat ThomasNo ratings yet
- Discontinuance of Drought Declaration of Local Emergency.11!22!23Document1 pageDiscontinuance of Drought Declaration of Local Emergency.11!22!23Pat ThomasNo ratings yet
- Franklin County Burn BanDocument1 pageFranklin County Burn BanJustin Daniel GearyNo ratings yet
- Report Use of Force Ashley Biggs Neeley Officer M Donellan Sept 27 2023Document3 pagesReport Use of Force Ashley Biggs Neeley Officer M Donellan Sept 27 2023Pat ThomasNo ratings yet
- Holiday Inn Express Martinsville Presentation - UpdatedDocument24 pagesHoliday Inn Express Martinsville Presentation - UpdatedPat ThomasNo ratings yet
- FERC Pipeline ApprovalDocument5 pagesFERC Pipeline ApprovalPat ThomasNo ratings yet
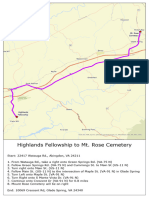
- Highlands To MT Rose 11x17Document1 pageHighlands To MT Rose 11x17Pat ThomasNo ratings yet
- NTSB Plane Crash ReportDocument4 pagesNTSB Plane Crash ReportPat ThomasNo ratings yet
- NTSB - Final Pitt. Co 2022 Plane Crash ReportDocument13 pagesNTSB - Final Pitt. Co 2022 Plane Crash ReportWSLSNo ratings yet
- Garbage Disposal BombsDocument1 pageGarbage Disposal BombsPat ThomasNo ratings yet
- Basic Characteristics of The Organic Agriculture MarketDocument11 pagesBasic Characteristics of The Organic Agriculture MarketshibaaniNo ratings yet
- Lecture Notes On Software Configuration Management: Zia Syed Carnegie Mellon UniversityDocument58 pagesLecture Notes On Software Configuration Management: Zia Syed Carnegie Mellon Universityvarsha reddyNo ratings yet
- Sustainable DevelopmentDocument5 pagesSustainable DevelopmentMeera NairNo ratings yet
- Senior High School Students' Academic Stress, Academic Motivation, and Its Relationship With Their Academic PerformanceDocument45 pagesSenior High School Students' Academic Stress, Academic Motivation, and Its Relationship With Their Academic PerformanceInternational Publication100% (1)
- Dac 100 Cat 2Document2 pagesDac 100 Cat 2Alistahr AmoloNo ratings yet
- Cost Analysis On Cadbury India LTDDocument21 pagesCost Analysis On Cadbury India LTDSurya Deepak Goud80% (20)
- IFT FDA TO6 (Product Tracing Pilots) FinalDocument334 pagesIFT FDA TO6 (Product Tracing Pilots) FinalAngela PatriciaNo ratings yet
- Air Plant Care Sheet: LightDocument3 pagesAir Plant Care Sheet: LightM Mohsin ChowdhuryNo ratings yet
- Emerging Trends in HRMDocument7 pagesEmerging Trends in HRMBarsha ChatterjeeNo ratings yet
- 1 PBDocument9 pages1 PBTariku KolchaNo ratings yet
- English: Quarter 2 - Module 6: You Spell!Document27 pagesEnglish: Quarter 2 - Module 6: You Spell!Warlyn Joy AmorNo ratings yet
- May 25, 2021 Revised Chapter 1-4Document70 pagesMay 25, 2021 Revised Chapter 1-4angelo felizardoNo ratings yet
- Lesson Plan in Technology For Teaching and LearningDocument6 pagesLesson Plan in Technology For Teaching and LearningNiña Mae CabsagNo ratings yet
- English q1 - Week6 Day1Document3 pagesEnglish q1 - Week6 Day1LADY ALTHEA TAHADNo ratings yet
- Accounting For Government and Not-For-Profit OrganizationsDocument29 pagesAccounting For Government and Not-For-Profit OrganizationsPatricia ReyesNo ratings yet
- (PDF) Johnson VictorDocument6 pages(PDF) Johnson Victorchinmay vijay100% (1)
- IB DP English A Literature Paper 1 SLDocument5 pagesIB DP English A Literature Paper 1 SLMenon HariNo ratings yet
- Buckling ChirajaraDocument50 pagesBuckling ChirajaraAlket DhamiNo ratings yet
- Nidhi TripathiDocument3 pagesNidhi TripathiAjay GuptaNo ratings yet
- The Legal Position of The Presumption ofDocument20 pagesThe Legal Position of The Presumption ofRANDAN SADIQNo ratings yet
- 2020 q3 Sportback ManualDocument38 pages2020 q3 Sportback Manualjose luis RamirezNo ratings yet
- Book SG L1 Answers PDFDocument18 pagesBook SG L1 Answers PDFKadir ErgenNo ratings yet
- Managing and Maintaining The Haccp SystemDocument16 pagesManaging and Maintaining The Haccp SystemANKUSHNo ratings yet
- KURVADocument7 pagesKURVAMuhammad Aris MunandarNo ratings yet
- Parts FaDocument14 pagesParts Faadiladilzade98No ratings yet
- Title ProposalDocument6 pagesTitle ProposalChanNo ratings yet
- (MY) Malaysia Shopee International PlatformDocument29 pages(MY) Malaysia Shopee International PlatformalexanderNo ratings yet