
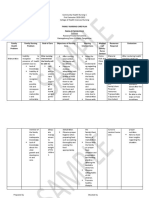
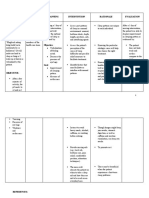
Family Nursing Care Plan: Initial Data Base
Family Nursing Care Plan: Initial Data Base
You might also like
- Public Health Nursing in The Philippines-1 1599890831 PDFDocument400 pagesPublic Health Nursing in The Philippines-1 1599890831 PDFBsusbs89% (18)
- NCP Impaired Verbal CommunicationDocument2 pagesNCP Impaired Verbal CommunicationLovelie Grace GalarpeNo ratings yet
- FNCP Risk For InfectionDocument4 pagesFNCP Risk For InfectionAemz Alacasnap Ainegud0% (1)
- Instrument of NormalDocument17 pagesInstrument of NormalEdraline Lumawig100% (2)
- MCN-OB Questions and RationalesDocument23 pagesMCN-OB Questions and RationalesRI NA100% (3)
- SMC and Tbi Fl11-035Document3 pagesSMC and Tbi Fl11-035Jim100% (1)
- FNCPDocument10 pagesFNCPMark Jaco AngNo ratings yet
- Family Nursing Care Plan: Cadavos, K. Pci Cero, P. Pci Cadavos, S. Pci Gula, M. PciDocument15 pagesFamily Nursing Care Plan: Cadavos, K. Pci Cero, P. Pci Cadavos, S. Pci Gula, M. PciLouis Gabriel AdayaNo ratings yet
- Family Nursing Care PlanDocument4 pagesFamily Nursing Care PlanSyvNo ratings yet
- Inadequate Living Space - NCPDocument2 pagesInadequate Living Space - NCPissaiahnicolleNo ratings yet
- Malnutrition FNCPDocument3 pagesMalnutrition FNCPMaribel ValenzuelaNo ratings yet
- FCP (Gorres)Document3 pagesFCP (Gorres)Kaloy KamaoNo ratings yet
- Family Nursing Care Plan - Inadequate Living SpaceDocument1 pageFamily Nursing Care Plan - Inadequate Living SpaceAngelica Malacay RevilNo ratings yet
- Family Care Plan of ROSARIO: (1 Level Assessment) (2 Level Assessment) (Specific)Document3 pagesFamily Care Plan of ROSARIO: (1 Level Assessment) (2 Level Assessment) (Specific)Eduard Reyjell MontañoNo ratings yet
- FNCP Inadequate Living SpaceDocument2 pagesFNCP Inadequate Living SpaceRouwi Desiatco100% (1)
- FNCP 1Document13 pagesFNCP 1Mikee PeraltaNo ratings yet
- Improper Food HandlingDocument2 pagesImproper Food HandlingampalNo ratings yet
- 2an - Chn-Family Interview Sheet - RamosDocument8 pages2an - Chn-Family Interview Sheet - RamosLouwella RamosNo ratings yet
- Family Nursing Care Plan FinalDocument1 pageFamily Nursing Care Plan FinalKhrisha Anne Davillo100% (1)
- Initial Data Base Fro Ics CHNDocument16 pagesInitial Data Base Fro Ics CHNMay Chelle ErazoNo ratings yet
- vINA Faulty Eating HabitsDocument2 pagesvINA Faulty Eating HabitsMyrshaida IbrahimNo ratings yet
- First Level AssessmentDocument2 pagesFirst Level AssessmentWenalyn Grace Abella LlavanNo ratings yet
- Family Nursing Care Plan Group 5Document2 pagesFamily Nursing Care Plan Group 5Aireen100% (1)
- FNCP Prioritization SheetDocument3 pagesFNCP Prioritization SheetAndrea Franchesca DelaCruz DescalzoNo ratings yet
- Typology of Nursing Care ProblemsDocument2 pagesTypology of Nursing Care ProblemsJohnny Yao JrNo ratings yet
- Typology of Nursing Problems in Family Nursing Practice and Scale Ranking Health Conditions and Problems According To PrioritiesDocument24 pagesTypology of Nursing Problems in Family Nursing Practice and Scale Ranking Health Conditions and Problems According To PrioritiesHannah Ros Quitorio II100% (1)
- Typology of A Problem and Family Nursing Care PlanDocument11 pagesTypology of A Problem and Family Nursing Care PlanAngelica Cassandra Villena100% (1)
- CHN FCPsDocument9 pagesCHN FCPsKZ100% (1)
- Criteria Computation Actual Score Justification 1.nature of The ProblemDocument4 pagesCriteria Computation Actual Score Justification 1.nature of The ProblemBeverly DatuNo ratings yet
- NCPDocument6 pagesNCPHaifa KanapiaNo ratings yet
- FNCPDocument4 pagesFNCPsenyorakathNo ratings yet
- Self/Home Medication As A Health Threat I. Inability ToDocument11 pagesSelf/Home Medication As A Health Threat I. Inability Tolan100% (1)
- Family Health Problems With CuesDocument4 pagesFamily Health Problems With CuesgerimyNo ratings yet
- FNCP Final EditedDocument10 pagesFNCP Final EditedMrLarry DolorNo ratings yet
- Problem: Diabetes Mellitus: Criteria Computation Actual Score Justification I. Nature of The ProblemDocument2 pagesProblem: Diabetes Mellitus: Criteria Computation Actual Score Justification I. Nature of The ProblemYessamin Paith Roderos100% (1)
- FNCPDocument3 pagesFNCPDarcey NicholeNo ratings yet
- Kat PrioDocument2 pagesKat PrioKatyana CesarNo ratings yet
- Family Nursing Care PlanDocument3 pagesFamily Nursing Care PlanJarda DacuagNo ratings yet
- ECOMAP Community Health Nursing CHNDocument1 pageECOMAP Community Health Nursing CHNmNo ratings yet
- Dysfunctional Uterine Bleeding (DUB)Document1 pageDysfunctional Uterine Bleeding (DUB)Bheru LalNo ratings yet
- Family Nursing Care Plan CHNDocument5 pagesFamily Nursing Care Plan CHNmachriza12308023No ratings yet
- FNCP For FAMPLANDocument2 pagesFNCP For FAMPLANJairah CandaoNo ratings yet
- Family Nursing Care Plan SampleDocument2 pagesFamily Nursing Care Plan SampleKhylamarie VillalunaNo ratings yet
- HypertensionDocument3 pagesHypertensionCheryl Lim SorianoNo ratings yet
- Poor Personal Hygiene PriorityDocument4 pagesPoor Personal Hygiene PrioritycamziiiNo ratings yet
- Cues/Data Family Nursing Problems: Unsanitary Food Handling and Preparation IDocument3 pagesCues/Data Family Nursing Problems: Unsanitary Food Handling and Preparation IAlbert GamasNo ratings yet
- FNCP Proper RevisedDocument2 pagesFNCP Proper RevisedKevinNo ratings yet
- Sample FNCP Accident HazardDocument2 pagesSample FNCP Accident HazardMichael PiducaNo ratings yet
- Family Nursing Care PlanDocument2 pagesFamily Nursing Care PlanXerxes DejitoNo ratings yet
- POST NATAL FNCP - DotdotDocument1 pagePOST NATAL FNCP - DotdotGiselle EstoquiaNo ratings yet
- Family Nursing Care Plan-MalnutritionDocument2 pagesFamily Nursing Care Plan-MalnutritionNovelyn PuaNo ratings yet
- Initial Data Base For Family Nursing Practice: A. Family Structure Characteristics and DynamicsDocument3 pagesInitial Data Base For Family Nursing Practice: A. Family Structure Characteristics and DynamicsjajaNo ratings yet
- FNCPDocument1 pageFNCPSummer SuarezNo ratings yet
- Water Source (Level 1) (Bacalla) : Criteria Score Weight Computation Actual Score JustificationDocument2 pagesWater Source (Level 1) (Bacalla) : Criteria Score Weight Computation Actual Score JustificationlovlyNo ratings yet
- Family Nursing Care Plan - HypertensionDocument3 pagesFamily Nursing Care Plan - HypertensionBiway RegalaNo ratings yet
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Objectives Interventions Rationale EvaluationAkiraMamoNo ratings yet
- Maternal PPT 2Document18 pagesMaternal PPT 2Judy UrciaNo ratings yet
- FNCP HyperacidityDocument2 pagesFNCP HyperacidityJeriel DelavinNo ratings yet
- Family Nursing Care Plan - Cough and ColdsDocument1 pageFamily Nursing Care Plan - Cough and ColdsArnx QuilonNo ratings yet
- FNCP FormatDocument1 pageFNCP FormatMav JavierNo ratings yet
- Initial Database For Family Nursing PracticeDocument17 pagesInitial Database For Family Nursing PracticeLevi Cyr PerezNo ratings yet
- CHN Fam PlanDocument6 pagesCHN Fam PlanmarcivandomingoNo ratings yet
- Justification - PataganDocument15 pagesJustification - PataganMariroseNo ratings yet
- Andrea Mae P. Salazar Bsn2Y1-Irr2 Criteria Computation Actual Score JustificationDocument7 pagesAndrea Mae P. Salazar Bsn2Y1-Irr2 Criteria Computation Actual Score Justificationerica mae rasNo ratings yet
- CHN FNCP IdbDocument8 pagesCHN FNCP IdbKaren AngelNo ratings yet
- Assessment of CardioDocument2 pagesAssessment of CardioEdraline LumawigNo ratings yet
- Assessment of RespiratoryDocument6 pagesAssessment of RespiratoryEdraline LumawigNo ratings yet
- Assessment of CardioDocument2 pagesAssessment of CardioEdraline LumawigNo ratings yet
- Anemia in Children CBC (Complete Blood Count)Document4 pagesAnemia in Children CBC (Complete Blood Count)Edraline LumawigNo ratings yet
- Republic Act 9512 or National Environmental Awareness and Education Act of 2008Document1 pageRepublic Act 9512 or National Environmental Awareness and Education Act of 2008Edraline LumawigNo ratings yet
- The Cask of AmontilladoDocument6 pagesThe Cask of AmontilladoEdraline LumawigNo ratings yet
- The FluDocument1 pageThe FluEdraline LumawigNo ratings yet
- TechnologyDocument2 pagesTechnologyEdraline LumawigNo ratings yet
- Does Age Matter in A RelationshipDocument3 pagesDoes Age Matter in A RelationshipEdraline LumawigNo ratings yet
- TechnologyDocument2 pagesTechnologyEdraline LumawigNo ratings yet
- Final Wiki - Martha RogersDocument4 pagesFinal Wiki - Martha Rogerslms93093No ratings yet
- CHAPTER 18 Application Theory in Nursing PracticeDocument27 pagesCHAPTER 18 Application Theory in Nursing PracticeRong Yu100% (2)
- Co SkillsDocument60 pagesCo SkillsTammy FlynnNo ratings yet
- PMCH ResearchDocument3 pagesPMCH ResearchGiormaru CuntapayNo ratings yet
- A New 2Document3 pagesA New 2Amy LalringhluaniNo ratings yet
- Admission and DischargeDocument61 pagesAdmission and DischargeRafia Khalil100% (2)
- Leadership MNGT .PPT Online PresentationDocument58 pagesLeadership MNGT .PPT Online PresentationDivynne Bless Madelo100% (2)
- Final 2014Document414 pagesFinal 2014Bhavesh Bhakodiya0% (1)
- English Form 1 - Question PaperDocument9 pagesEnglish Form 1 - Question PaperFredrick LangatNo ratings yet
- TFN PDFDocument5 pagesTFN PDFNoel TanNo ratings yet
- Ebp PicotDocument16 pagesEbp Picotapi-574405992No ratings yet
- Family Care Plan-Health DeficitDocument3 pagesFamily Care Plan-Health DeficitGia Espinosa Ocbeña100% (1)
- Go Ishi Nadine R.Document5 pagesGo Ishi Nadine R.SAMANTHA T. MODESTONo ratings yet
- Module I Group WorkDocument6 pagesModule I Group WorkNur Sanaani100% (1)
- NCMB317 RUBRICS Mental Status ExaminationDocument1 pageNCMB317 RUBRICS Mental Status Examinationkpbalay5921pamNo ratings yet
- Communication Is A Vital Component of Case Management SkillsDocument8 pagesCommunication Is A Vital Component of Case Management SkillsZK WriterNo ratings yet
- Communication Skills Education For Doctors: An UpdateDocument50 pagesCommunication Skills Education For Doctors: An UpdateDaniel PendickNo ratings yet
- History of Nursing: Florence NightingaleDocument4 pagesHistory of Nursing: Florence NightingaleMA. LOUIMAR CATUNo ratings yet
- Role of Hospital Management Information System in Tertiary Care HospitalDocument7 pagesRole of Hospital Management Information System in Tertiary Care HospitalKunal PatelNo ratings yet
- Consolidated Advertisement No. 02/2016Document4 pagesConsolidated Advertisement No. 02/2016Ahsan KhanNo ratings yet
- Philippine Nursing LawDocument1 pagePhilippine Nursing LawReann LeeNo ratings yet
- Assessment: Mental Health Care PlanDocument3 pagesAssessment: Mental Health Care PlannamitaNo ratings yet
- School ResumeDocument1 pageSchool Resumerachel crawfordNo ratings yet
- NCP - Disturbed Sleep PatternDocument3 pagesNCP - Disturbed Sleep PatternKyla CalzadoNo ratings yet
- Newman'S Theory of Health As Expanding Consciousness: Margaret A. Newman, RN, PHDDocument17 pagesNewman'S Theory of Health As Expanding Consciousness: Margaret A. Newman, RN, PHDLany Saccuan Coloma100% (1)
- Pubmed - Australia - Clinical - brokenAffLastHistoDocument131 pagesPubmed - Australia - Clinical - brokenAffLastHistoHNNo ratings yet


































































































Download as docx, pdf, or txt
You might also like
- Public Health Nursing in The Philippines-1 1599890831 PDFDocument400 pagesPublic Health Nursing in The Philippines-1 1599890831 PDFBsusbs89% (18)
- NCP Impaired Verbal CommunicationDocument2 pagesNCP Impaired Verbal CommunicationLovelie Grace GalarpeNo ratings yet
- FNCP Risk For InfectionDocument4 pagesFNCP Risk For InfectionAemz Alacasnap Ainegud0% (1)
- Instrument of NormalDocument17 pagesInstrument of NormalEdraline Lumawig100% (2)
- MCN-OB Questions and RationalesDocument23 pagesMCN-OB Questions and RationalesRI NA100% (3)
- SMC and Tbi Fl11-035Document3 pagesSMC and Tbi Fl11-035Jim100% (1)
- FNCPDocument10 pagesFNCPMark Jaco AngNo ratings yet
- Family Nursing Care Plan: Cadavos, K. Pci Cero, P. Pci Cadavos, S. Pci Gula, M. PciDocument15 pagesFamily Nursing Care Plan: Cadavos, K. Pci Cero, P. Pci Cadavos, S. Pci Gula, M. PciLouis Gabriel AdayaNo ratings yet
- Family Nursing Care PlanDocument4 pagesFamily Nursing Care PlanSyvNo ratings yet
- Inadequate Living Space - NCPDocument2 pagesInadequate Living Space - NCPissaiahnicolleNo ratings yet
- Malnutrition FNCPDocument3 pagesMalnutrition FNCPMaribel ValenzuelaNo ratings yet
- FCP (Gorres)Document3 pagesFCP (Gorres)Kaloy KamaoNo ratings yet
- Family Nursing Care Plan - Inadequate Living SpaceDocument1 pageFamily Nursing Care Plan - Inadequate Living SpaceAngelica Malacay RevilNo ratings yet
- Family Care Plan of ROSARIO: (1 Level Assessment) (2 Level Assessment) (Specific)Document3 pagesFamily Care Plan of ROSARIO: (1 Level Assessment) (2 Level Assessment) (Specific)Eduard Reyjell MontañoNo ratings yet
- FNCP Inadequate Living SpaceDocument2 pagesFNCP Inadequate Living SpaceRouwi Desiatco100% (1)
- FNCP 1Document13 pagesFNCP 1Mikee PeraltaNo ratings yet
- Improper Food HandlingDocument2 pagesImproper Food HandlingampalNo ratings yet
- 2an - Chn-Family Interview Sheet - RamosDocument8 pages2an - Chn-Family Interview Sheet - RamosLouwella RamosNo ratings yet
- Family Nursing Care Plan FinalDocument1 pageFamily Nursing Care Plan FinalKhrisha Anne Davillo100% (1)
- Initial Data Base Fro Ics CHNDocument16 pagesInitial Data Base Fro Ics CHNMay Chelle ErazoNo ratings yet
- vINA Faulty Eating HabitsDocument2 pagesvINA Faulty Eating HabitsMyrshaida IbrahimNo ratings yet
- First Level AssessmentDocument2 pagesFirst Level AssessmentWenalyn Grace Abella LlavanNo ratings yet
- Family Nursing Care Plan Group 5Document2 pagesFamily Nursing Care Plan Group 5Aireen100% (1)
- FNCP Prioritization SheetDocument3 pagesFNCP Prioritization SheetAndrea Franchesca DelaCruz DescalzoNo ratings yet
- Typology of Nursing Care ProblemsDocument2 pagesTypology of Nursing Care ProblemsJohnny Yao JrNo ratings yet
- Typology of Nursing Problems in Family Nursing Practice and Scale Ranking Health Conditions and Problems According To PrioritiesDocument24 pagesTypology of Nursing Problems in Family Nursing Practice and Scale Ranking Health Conditions and Problems According To PrioritiesHannah Ros Quitorio II100% (1)
- Typology of A Problem and Family Nursing Care PlanDocument11 pagesTypology of A Problem and Family Nursing Care PlanAngelica Cassandra Villena100% (1)
- CHN FCPsDocument9 pagesCHN FCPsKZ100% (1)
- Criteria Computation Actual Score Justification 1.nature of The ProblemDocument4 pagesCriteria Computation Actual Score Justification 1.nature of The ProblemBeverly DatuNo ratings yet
- NCPDocument6 pagesNCPHaifa KanapiaNo ratings yet
- FNCPDocument4 pagesFNCPsenyorakathNo ratings yet
- Self/Home Medication As A Health Threat I. Inability ToDocument11 pagesSelf/Home Medication As A Health Threat I. Inability Tolan100% (1)
- Family Health Problems With CuesDocument4 pagesFamily Health Problems With CuesgerimyNo ratings yet
- FNCP Final EditedDocument10 pagesFNCP Final EditedMrLarry DolorNo ratings yet
- Problem: Diabetes Mellitus: Criteria Computation Actual Score Justification I. Nature of The ProblemDocument2 pagesProblem: Diabetes Mellitus: Criteria Computation Actual Score Justification I. Nature of The ProblemYessamin Paith Roderos100% (1)
- FNCPDocument3 pagesFNCPDarcey NicholeNo ratings yet
- Kat PrioDocument2 pagesKat PrioKatyana CesarNo ratings yet
- Family Nursing Care PlanDocument3 pagesFamily Nursing Care PlanJarda DacuagNo ratings yet
- ECOMAP Community Health Nursing CHNDocument1 pageECOMAP Community Health Nursing CHNmNo ratings yet
- Dysfunctional Uterine Bleeding (DUB)Document1 pageDysfunctional Uterine Bleeding (DUB)Bheru LalNo ratings yet
- Family Nursing Care Plan CHNDocument5 pagesFamily Nursing Care Plan CHNmachriza12308023No ratings yet
- FNCP For FAMPLANDocument2 pagesFNCP For FAMPLANJairah CandaoNo ratings yet
- Family Nursing Care Plan SampleDocument2 pagesFamily Nursing Care Plan SampleKhylamarie VillalunaNo ratings yet
- HypertensionDocument3 pagesHypertensionCheryl Lim SorianoNo ratings yet
- Poor Personal Hygiene PriorityDocument4 pagesPoor Personal Hygiene PrioritycamziiiNo ratings yet
- Cues/Data Family Nursing Problems: Unsanitary Food Handling and Preparation IDocument3 pagesCues/Data Family Nursing Problems: Unsanitary Food Handling and Preparation IAlbert GamasNo ratings yet
- FNCP Proper RevisedDocument2 pagesFNCP Proper RevisedKevinNo ratings yet
- Sample FNCP Accident HazardDocument2 pagesSample FNCP Accident HazardMichael PiducaNo ratings yet
- Family Nursing Care PlanDocument2 pagesFamily Nursing Care PlanXerxes DejitoNo ratings yet
- POST NATAL FNCP - DotdotDocument1 pagePOST NATAL FNCP - DotdotGiselle EstoquiaNo ratings yet
- Family Nursing Care Plan-MalnutritionDocument2 pagesFamily Nursing Care Plan-MalnutritionNovelyn PuaNo ratings yet
- Initial Data Base For Family Nursing Practice: A. Family Structure Characteristics and DynamicsDocument3 pagesInitial Data Base For Family Nursing Practice: A. Family Structure Characteristics and DynamicsjajaNo ratings yet
- FNCPDocument1 pageFNCPSummer SuarezNo ratings yet
- Water Source (Level 1) (Bacalla) : Criteria Score Weight Computation Actual Score JustificationDocument2 pagesWater Source (Level 1) (Bacalla) : Criteria Score Weight Computation Actual Score JustificationlovlyNo ratings yet
- Family Nursing Care Plan - HypertensionDocument3 pagesFamily Nursing Care Plan - HypertensionBiway RegalaNo ratings yet
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Objectives Interventions Rationale EvaluationAkiraMamoNo ratings yet
- Maternal PPT 2Document18 pagesMaternal PPT 2Judy UrciaNo ratings yet
- FNCP HyperacidityDocument2 pagesFNCP HyperacidityJeriel DelavinNo ratings yet
- Family Nursing Care Plan - Cough and ColdsDocument1 pageFamily Nursing Care Plan - Cough and ColdsArnx QuilonNo ratings yet
- FNCP FormatDocument1 pageFNCP FormatMav JavierNo ratings yet
- Initial Database For Family Nursing PracticeDocument17 pagesInitial Database For Family Nursing PracticeLevi Cyr PerezNo ratings yet
- CHN Fam PlanDocument6 pagesCHN Fam PlanmarcivandomingoNo ratings yet
- Justification - PataganDocument15 pagesJustification - PataganMariroseNo ratings yet
- Andrea Mae P. Salazar Bsn2Y1-Irr2 Criteria Computation Actual Score JustificationDocument7 pagesAndrea Mae P. Salazar Bsn2Y1-Irr2 Criteria Computation Actual Score Justificationerica mae rasNo ratings yet
- CHN FNCP IdbDocument8 pagesCHN FNCP IdbKaren AngelNo ratings yet
- Assessment of CardioDocument2 pagesAssessment of CardioEdraline LumawigNo ratings yet
- Assessment of RespiratoryDocument6 pagesAssessment of RespiratoryEdraline LumawigNo ratings yet
- Assessment of CardioDocument2 pagesAssessment of CardioEdraline LumawigNo ratings yet
- Anemia in Children CBC (Complete Blood Count)Document4 pagesAnemia in Children CBC (Complete Blood Count)Edraline LumawigNo ratings yet
- Republic Act 9512 or National Environmental Awareness and Education Act of 2008Document1 pageRepublic Act 9512 or National Environmental Awareness and Education Act of 2008Edraline LumawigNo ratings yet
- The Cask of AmontilladoDocument6 pagesThe Cask of AmontilladoEdraline LumawigNo ratings yet
- The FluDocument1 pageThe FluEdraline LumawigNo ratings yet
- TechnologyDocument2 pagesTechnologyEdraline LumawigNo ratings yet
- Does Age Matter in A RelationshipDocument3 pagesDoes Age Matter in A RelationshipEdraline LumawigNo ratings yet
- TechnologyDocument2 pagesTechnologyEdraline LumawigNo ratings yet
- Final Wiki - Martha RogersDocument4 pagesFinal Wiki - Martha Rogerslms93093No ratings yet
- CHAPTER 18 Application Theory in Nursing PracticeDocument27 pagesCHAPTER 18 Application Theory in Nursing PracticeRong Yu100% (2)
- Co SkillsDocument60 pagesCo SkillsTammy FlynnNo ratings yet
- PMCH ResearchDocument3 pagesPMCH ResearchGiormaru CuntapayNo ratings yet
- A New 2Document3 pagesA New 2Amy LalringhluaniNo ratings yet
- Admission and DischargeDocument61 pagesAdmission and DischargeRafia Khalil100% (2)
- Leadership MNGT .PPT Online PresentationDocument58 pagesLeadership MNGT .PPT Online PresentationDivynne Bless Madelo100% (2)
- Final 2014Document414 pagesFinal 2014Bhavesh Bhakodiya0% (1)
- English Form 1 - Question PaperDocument9 pagesEnglish Form 1 - Question PaperFredrick LangatNo ratings yet
- TFN PDFDocument5 pagesTFN PDFNoel TanNo ratings yet
- Ebp PicotDocument16 pagesEbp Picotapi-574405992No ratings yet
- Family Care Plan-Health DeficitDocument3 pagesFamily Care Plan-Health DeficitGia Espinosa Ocbeña100% (1)
- Go Ishi Nadine R.Document5 pagesGo Ishi Nadine R.SAMANTHA T. MODESTONo ratings yet
- Module I Group WorkDocument6 pagesModule I Group WorkNur Sanaani100% (1)
- NCMB317 RUBRICS Mental Status ExaminationDocument1 pageNCMB317 RUBRICS Mental Status Examinationkpbalay5921pamNo ratings yet
- Communication Is A Vital Component of Case Management SkillsDocument8 pagesCommunication Is A Vital Component of Case Management SkillsZK WriterNo ratings yet
- Communication Skills Education For Doctors: An UpdateDocument50 pagesCommunication Skills Education For Doctors: An UpdateDaniel PendickNo ratings yet
- History of Nursing: Florence NightingaleDocument4 pagesHistory of Nursing: Florence NightingaleMA. LOUIMAR CATUNo ratings yet
- Role of Hospital Management Information System in Tertiary Care HospitalDocument7 pagesRole of Hospital Management Information System in Tertiary Care HospitalKunal PatelNo ratings yet
- Consolidated Advertisement No. 02/2016Document4 pagesConsolidated Advertisement No. 02/2016Ahsan KhanNo ratings yet
- Philippine Nursing LawDocument1 pagePhilippine Nursing LawReann LeeNo ratings yet
- Assessment: Mental Health Care PlanDocument3 pagesAssessment: Mental Health Care PlannamitaNo ratings yet
- School ResumeDocument1 pageSchool Resumerachel crawfordNo ratings yet
- NCP - Disturbed Sleep PatternDocument3 pagesNCP - Disturbed Sleep PatternKyla CalzadoNo ratings yet
- Newman'S Theory of Health As Expanding Consciousness: Margaret A. Newman, RN, PHDDocument17 pagesNewman'S Theory of Health As Expanding Consciousness: Margaret A. Newman, RN, PHDLany Saccuan Coloma100% (1)
- Pubmed - Australia - Clinical - brokenAffLastHistoDocument131 pagesPubmed - Australia - Clinical - brokenAffLastHistoHNNo ratings yet