Download as xlsx, pdf, or txt
You might also like
- Health DeclarationDocument2 pagesHealth DeclarationJerick AlmedaNo ratings yet
- Health DeclarationDocument1 pageHealth DeclarationEdenNo ratings yet
- Parent Orientation On MLDM and Dry Run-1Document25 pagesParent Orientation On MLDM and Dry Run-1PATRICK VEQUILLANo ratings yet
- Parent Orientation On MLDM and Dry RunDocument25 pagesParent Orientation On MLDM and Dry RunPATRICK VEQUILLANo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormJean Manzanilla CarinanNo ratings yet
- Deped Vigan City Covid19 Health ChecklistDocument1 pageDeped Vigan City Covid19 Health ChecklistLemmor ObarNo ratings yet
- School Health Declaration Survey Form A4Document1 pageSchool Health Declaration Survey Form A4Clarizze AnnNo ratings yet
- Students Health SurveyDocument1 pageStudents Health SurveyJulie Basbas-CruzNo ratings yet
- Health Decleration FormDocument1 pageHealth Decleration FormGabrile GUIOGUIONo ratings yet
- Traveller Public Health Declaration Document-Sbloccato-ConvertitoDocument1 pageTraveller Public Health Declaration Document-Sbloccato-ConvertitoPino BellomoNo ratings yet
- Screening FormDocument2 pagesScreening FormMarie I. RosalesNo ratings yet
- Alayon Health Declaration Form 2Document1 pageAlayon Health Declaration Form 2Farah AlayonNo ratings yet
- HEALTH DECLARATION FORM SmallDocument1 pageHEALTH DECLARATION FORM SmallChai BarcelonNo ratings yet
- Health FormDocument1 pageHealth FormLinlen ViagedorNo ratings yet
- Health Declaration Form 1Document1 pageHealth Declaration Form 1April Mae O. MacalesNo ratings yet
- Coronavirus (COVID-19) Health Questionnaire For Contractors and Visitors (APPROVED)Document1 pageCoronavirus (COVID-19) Health Questionnaire For Contractors and Visitors (APPROVED)Giri WakshanNo ratings yet
- ContacttracingDocument2 pagesContacttracingCee Leila ComodasNo ratings yet
- COVID-19 Health Declaration Form (Rev. 4)Document2 pagesCOVID-19 Health Declaration Form (Rev. 4)ammar razaNo ratings yet
- Coronavirus Self Declaration FormDocument1 pageCoronavirus Self Declaration Formvpo almonbevsambNo ratings yet
- HDF For MDC Projects Version 06052020Document1 pageHDF For MDC Projects Version 06052020Jude Bon Albao0% (1)
- Health-Declaration-Form 2Document1 pageHealth-Declaration-Form 2menchieNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAzri AzizNo ratings yet
- Health Checklist Health Checklist Temperature: TemperatureDocument2 pagesHealth Checklist Health Checklist Temperature: TemperatureJeniffer FajardoNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormCristian HolicovNo ratings yet
- Covid-19 Health Declaration Form: Thank You For Your CooperationDocument1 pageCovid-19 Health Declaration Form: Thank You For Your Cooperationsuria qaqcNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageMiamor NatividadNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageJoezerk CarpioNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PagemarieleNo ratings yet
- HDF PDFDocument1 pageHDF PDFJhon Rey GonsalezNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageFedelyn SemenianoNo ratings yet
- Health Form For Civil Service ExamDocument1 pageHealth Form For Civil Service Examralph sabaNo ratings yet
- Health Declaration: YES NODocument1 pageHealth Declaration: YES NOEliezal Dean B. CardeñoNo ratings yet
- 01 - 3【English】 (Sample) Prevaccination Screening QuestionnaireDocument1 page01 - 3【English】 (Sample) Prevaccination Screening QuestionnaireThet Ko WinNo ratings yet
- Traveller Public Health Declaration (English)Document1 pageTraveller Public Health Declaration (English)Margarete Maria AhammerNo ratings yet
- Daily Health Checklist - TruckersDocument1 pageDaily Health Checklist - TruckersElbert Leo AstilleroNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormRandy OpadiaNo ratings yet
- Health DecDocument1 pageHealth DecDhonna ManigbasNo ratings yet
- Adakah Anda Mengalami Gejala-Gejala Respiratori Berikut?Document3 pagesAdakah Anda Mengalami Gejala-Gejala Respiratori Berikut?Eu JinnNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormMary Grace MaribaoNo ratings yet
- Health Mon. Final - Student TempDocument4 pagesHealth Mon. Final - Student TempCherry Mae Joy YbañezNo ratings yet
- Health ChecklistDocument1 pageHealth ChecklistMelba BarcelNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormJelena Borić FarkašNo ratings yet
- Screening Questionnaire (Workplace Prevention and Control)Document1 pageScreening Questionnaire (Workplace Prevention and Control)Tristan BabaylanNo ratings yet
- Maap Health ChecklistDocument1 pageMaap Health ChecklistRaymund MagallonesNo ratings yet
- Declaration - Return To Work Form (Covid 19) : EmployeeDocument2 pagesDeclaration - Return To Work Form (Covid 19) : EmployeeFahad Khalid100% (1)
- Health Declaration Form-1-1Document2 pagesHealth Declaration Form-1-1Jimmy LaguraNo ratings yet
- CHECKLISTDocument1 pageCHECKLISTMarisol NoolNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration Formargie joy marieNo ratings yet
- Region Iv-A Calabarzon Division of Batangas Sto. Niño Formation and Science SchoolDocument2 pagesRegion Iv-A Calabarzon Division of Batangas Sto. Niño Formation and Science SchoolHUMSS 11-BNo ratings yet
- Health Declaration Form 1Document2 pagesHealth Declaration Form 1Elorde M. ShalaniNo ratings yet
- School Health DeclarationDocument3 pagesSchool Health DeclarationRuchie CardenoNo ratings yet
- MG - Guest COVID-19 - Health QuestionnaireDocument2 pagesMG - Guest COVID-19 - Health QuestionnaireSher BNo ratings yet
- Quarantine Form 1Document1 pageQuarantine Form 1Rachel AndesNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormMarriah Izzabelle Suarez RamadaNo ratings yet
- Health-Declaration-Checklist 2Document1 pageHealth-Declaration-Checklist 2Beverly Trangia100% (2)
- Self Declaration ChecklistDocument1 pageSelf Declaration ChecklistRitchelle Quijote DelgadoNo ratings yet
- WCR Annexure - 1 FromDocument1 pageWCR Annexure - 1 FromSaikat DawanNo ratings yet
- Self Assessment / Checklist FormDocument1 pageSelf Assessment / Checklist FormAiza Rhea SantosNo ratings yet
- Health Declaration Form f2f 1Document1 pageHealth Declaration Form f2f 1Paula BurogNo ratings yet
- Health DeclarationDocument2 pagesHealth DeclarationJerick AlmedaNo ratings yet
- Week 1.1 - Introduction To Software EngineeringDocument11 pagesWeek 1.1 - Introduction To Software EngineeringJerick AlmedaNo ratings yet
- Qualified Vendors List (QVL) : Bus Support Card Type Module P/N. Size Chip P/N. Release Date Module Supplier InterfaceDocument1 pageQualified Vendors List (QVL) : Bus Support Card Type Module P/N. Size Chip P/N. Release Date Module Supplier InterfaceVitor JorgeNo ratings yet
- PHP Advanced Series 2 - PHP FunctionsDocument21 pagesPHP Advanced Series 2 - PHP FunctionsJerick AlmedaNo ratings yet
- Case Study For Round 1 of HCCB Case Challenge Season 1Document4 pagesCase Study For Round 1 of HCCB Case Challenge Season 1NitikaNo ratings yet
- Trits SS 4Document1 pageTrits SS 4radiologia hapNo ratings yet
- M8860 SDS (GHS) EngMalayDocument9 pagesM8860 SDS (GHS) EngMalayA4blackNo ratings yet
- Lane, RobertDocument20 pagesLane, RobertVALERIA AGUILARNo ratings yet
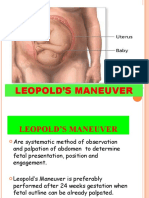
- Leopold's ManeuverDocument22 pagesLeopold's ManeuverArlene Cerdeña Salceda100% (1)
- Colorful Creative Doodle Brand Message InfographicDocument1 pageColorful Creative Doodle Brand Message InfographicRemelina LeeNo ratings yet
- Medical Certificate MC Form 1 All Sports EventsDocument2 pagesMedical Certificate MC Form 1 All Sports EventsKriston CabilesNo ratings yet
- SIKARDocument180 pagesSIKARShweta jainNo ratings yet
- Allegheny ObservershipDocument4 pagesAllegheny ObservershipTayyab Muhammad TahirNo ratings yet
- Test Questionnaires With Key Answer - Gabriel Aand BobisDocument6 pagesTest Questionnaires With Key Answer - Gabriel Aand BobisLeah BobisNo ratings yet
- Physical Education Lesson Plan For Circuit TrainingDocument3 pagesPhysical Education Lesson Plan For Circuit Trainingapi-338679470No ratings yet
- Physical Education and Health 11: Learning Activity Sheet (Week 5-6) Personal Safety Background InformationDocument4 pagesPhysical Education and Health 11: Learning Activity Sheet (Week 5-6) Personal Safety Background InformationRheena-Ann Dupale PadillaNo ratings yet
- Facial Pigmentation Impacts Quality of Life Regardless of Clinical SeverityDocument7 pagesFacial Pigmentation Impacts Quality of Life Regardless of Clinical SeverityMeta SakinaNo ratings yet
- STEM Journal 2017 2018Document147 pagesSTEM Journal 2017 2018Francesco RossetiNo ratings yet
- Exploración de La Eficacia Del Uso de Solución Salina Hipertónica para El Tratamiento de Nebulización en Niños Con Bronquiolitis - Un Metanálisis de Ensayos Controlados AleatoriosDocument24 pagesExploración de La Eficacia Del Uso de Solución Salina Hipertónica para El Tratamiento de Nebulización en Niños Con Bronquiolitis - Un Metanálisis de Ensayos Controlados AleatoriosDiego CastilloNo ratings yet
- Leading and Managing in Nursing 5th Edition Yoder Wise Test BankDocument10 pagesLeading and Managing in Nursing 5th Edition Yoder Wise Test Bankmorgaycarter.tizes100% (29)
- Duron UHP 5W-30: Safety Data SheetDocument11 pagesDuron UHP 5W-30: Safety Data SheetZuhailiNo ratings yet
- Hypertension in Hemodialysis PatientDocument54 pagesHypertension in Hemodialysis PatientIchtiar MahesaNo ratings yet
- Project Wise CSR Expenditure FY202223Document15 pagesProject Wise CSR Expenditure FY202223gowowor677No ratings yet
- BMRCL - SOP For WorksDocument3 pagesBMRCL - SOP For WorksravindraNo ratings yet
- A.Examine A Healthcare Organization That Has Significance To You,...Document7 pagesA.Examine A Healthcare Organization That Has Significance To You,...DrogNo ratings yet
- Canteen Committee SOP IRCC/HR/: 11/2021 Sop No: HR/003Document3 pagesCanteen Committee SOP IRCC/HR/: 11/2021 Sop No: HR/003sham naguNo ratings yet
- Finals Reviewer Funda SkillsDocument9 pagesFinals Reviewer Funda SkillsTricia Maxine DomingoNo ratings yet
- DLP - Grade 8 - Diseases That Result From Nutrient Deficiency and Ingestion of Harmful Substances. EditedDocument9 pagesDLP - Grade 8 - Diseases That Result From Nutrient Deficiency and Ingestion of Harmful Substances. Editedmars100% (3)
- Supporting Students With DisabilitiesDocument29 pagesSupporting Students With Disabilitiesapi-553169681No ratings yet
- Comprehension, Literature, Grammar Study PackDocument30 pagesComprehension, Literature, Grammar Study PackMarwan OsamaNo ratings yet
- ARW1 - Midterm Exam - Virtual 202211 Avanzado 10 17-45-19 - 15Document7 pagesARW1 - Midterm Exam - Virtual 202211 Avanzado 10 17-45-19 - 15Rosa Milagros Mostorino PiconNo ratings yet
- SoP - MIT Media LabsDocument3 pagesSoP - MIT Media LabsAbhilash SreekumarNo ratings yet
- Accessibility Audit: by Dr. Parag NarkhedeDocument27 pagesAccessibility Audit: by Dr. Parag NarkhedeRadhika AgarwalNo ratings yet
- Burnout Among Esl Universiti Teknologi Malaysia EducatorsDocument7 pagesBurnout Among Esl Universiti Teknologi Malaysia Educatorsxll21No ratings yet