
Jurnal Kubba Dan Robertson Pada Tahun 2008, Krim
Jurnal Kubba Dan Robertson Pada Tahun 2008, Krim
You might also like
- Acute and Chronic Wounds - Current Management Concepts (PDFDrive)Document1,872 pagesAcute and Chronic Wounds - Current Management Concepts (PDFDrive)Tasha FarahNo ratings yet
- Vitiligo ObatDocument6 pagesVitiligo ObatLidwina DewiNo ratings yet
- Primary Operative Versus Nonoperative Therapy For Pediatric Empyema: A Meta-AnalysisDocument9 pagesPrimary Operative Versus Nonoperative Therapy For Pediatric Empyema: A Meta-AnalysisDr Nilesh NagdeveNo ratings yet
- Comparison of Amoxicillin/Clavulanic Acid High Dose With Cef Dinir in The Treatment of Acute Otitis MediaDocument8 pagesComparison of Amoxicillin/Clavulanic Acid High Dose With Cef Dinir in The Treatment of Acute Otitis Mediaenggainget8663No ratings yet
- Pediatric Pharmacology and TherapeuticsDocument6 pagesPediatric Pharmacology and TherapeuticsRatna SriwahyuniNo ratings yet
- Nejmoa1911998 PDFDocument11 pagesNejmoa1911998 PDFStella NoviaNo ratings yet
- Sample Critics RTCDocument12 pagesSample Critics RTCGada NagariNo ratings yet
- Journal of Pediatric Surgery: Indepent Review ArticlesDocument4 pagesJournal of Pediatric Surgery: Indepent Review ArticlesNur Ainatun NadrahNo ratings yet
- JURNAL READINGnejmoa1007174Document11 pagesJURNAL READINGnejmoa1007174Sukma WinahyuNo ratings yet
- Pediatrics 1981 Gunn 61 7Document9 pagesPediatrics 1981 Gunn 61 7Marlon SoselisaNo ratings yet
- Clinical Profile of Empyema in Tertiary Health Care Center, HyderabadDocument4 pagesClinical Profile of Empyema in Tertiary Health Care Center, HyderabadririNo ratings yet
- Short-Course Antimicrobial Therapy For Pediatric Community-Acquired Pneumonia - PMCDocument19 pagesShort-Course Antimicrobial Therapy For Pediatric Community-Acquired Pneumonia - PMCFrances Jean T. DoblasNo ratings yet
- Current Success in The Treatment of Intussusception in ChildrenDocument9 pagesCurrent Success in The Treatment of Intussusception in ChildrenOby RomdhoniNo ratings yet
- Complementary Therapies in Medicine: Contents Lists Available atDocument13 pagesComplementary Therapies in Medicine: Contents Lists Available atAndi UmmahNo ratings yet
- 2518-Article Text-13816-1-10-20201215Document6 pages2518-Article Text-13816-1-10-20201215JAN CAMILLE LENONNo ratings yet
- Scopus (29) Many2017Document7 pagesScopus (29) Many2017ika puspitaNo ratings yet
- Role of Dexamethasone in Neonatal Meningitis 2012Document6 pagesRole of Dexamethasone in Neonatal Meningitis 2012jose alberto gamboaNo ratings yet
- 403 Full PDFDocument2 pages403 Full PDFMafia 12mia5No ratings yet
- PXW 011Document5 pagesPXW 011rendyjiwonoNo ratings yet
- 976 FullDocument6 pages976 FullazifadewiatasyaNo ratings yet
- To Study The Effectiveness of Oral Azithromycin As Compared To Parenteral Ceftriaxone in The Treatment of Uncomplicated Enteric FeverDocument5 pagesTo Study The Effectiveness of Oral Azithromycin As Compared To Parenteral Ceftriaxone in The Treatment of Uncomplicated Enteric FeverSari MustikaNo ratings yet
- Epilepsy in Tubero Sclerosis ComplexDocument7 pagesEpilepsy in Tubero Sclerosis ComplexDenny SigarlakiNo ratings yet
- Fetal Inflamatory Response SyndromeDocument9 pagesFetal Inflamatory Response SyndromeAnonymous mvNUtwidNo ratings yet
- Jurnal Sidang RespiDocument4 pagesJurnal Sidang RespiAnis Eka SukmadadariNo ratings yet
- Comparison of Two Different Antibiotic Regimens For The Prophylaxisis of Cases With Preterm Premature Rupture of Membranes: A Randomized Clinical TrialDocument5 pagesComparison of Two Different Antibiotic Regimens For The Prophylaxisis of Cases With Preterm Premature Rupture of Membranes: A Randomized Clinical TrialVindee VictoryNo ratings yet
- Chamnanvanakij, 2005Document6 pagesChamnanvanakij, 2005Fatma ElzaytNo ratings yet
- Chloramphenicol Treatment For Acute Infective Conjunctivitis in Children in Primary Care: A Randomised Double-Blind Placebo-Controlled TrialDocument8 pagesChloramphenicol Treatment For Acute Infective Conjunctivitis in Children in Primary Care: A Randomised Double-Blind Placebo-Controlled TrialFemi OdeNo ratings yet
- Perbandingan Efektifitas Kloramfenikol Dan Gentamisin Pada Dakriosistitis BayiDocument7 pagesPerbandingan Efektifitas Kloramfenikol Dan Gentamisin Pada Dakriosistitis BayiChristian SolihinNo ratings yet
- Management of Rectal Prolapse in ChildrenDocument6 pagesManagement of Rectal Prolapse in ChildrenWaNda GrNo ratings yet
- Treatment of Acute Otitis Media in Children Under 2 Years of AgeDocument29 pagesTreatment of Acute Otitis Media in Children Under 2 Years of AgesellyhdelhiNo ratings yet
- Thoracoscopic Decortication Vs Tube Thoracostomy With Fibrinolysis For Empyema in Children: A Prospective, Randomized TrialDocument6 pagesThoracoscopic Decortication Vs Tube Thoracostomy With Fibrinolysis For Empyema in Children: A Prospective, Randomized TrialcarlaNo ratings yet
- Sedation and Analgesia in Children Undergoing Invasive ProceduresDocument7 pagesSedation and Analgesia in Children Undergoing Invasive ProceduresSantosa TandiNo ratings yet
- Neonatal Mastitis: Controversies in Management: October 2012Document5 pagesNeonatal Mastitis: Controversies in Management: October 2012ditaNo ratings yet
- CAP - Risk Factors and TreatmentDocument5 pagesCAP - Risk Factors and Treatmentgrool29rNo ratings yet
- Early Analgesia For Children With Acute Abdominal Pain: ObjectivesDocument8 pagesEarly Analgesia For Children With Acute Abdominal Pain: Objectivescrizt tyanNo ratings yet
- With Intravenous Antibiotics Urinary Tract Infections in 1-To 3-Month-Old Infants: Ambulatory TreatmentDocument9 pagesWith Intravenous Antibiotics Urinary Tract Infections in 1-To 3-Month-Old Infants: Ambulatory Treatmentsri_jva8No ratings yet
- Piis1474442208701418 PDFDocument8 pagesPiis1474442208701418 PDFsebastian quiroz floresNo ratings yet
- Comparison Between Small and Large Bowel Intussusception in ChildrenDocument3 pagesComparison Between Small and Large Bowel Intussusception in ChildrenParamartha KesumaNo ratings yet
- 1 s2.0 S0002937899707039 MainDocument5 pages1 s2.0 S0002937899707039 MainPutri AgriNo ratings yet
- Kim 2015Document4 pagesKim 2015ruthameliapNo ratings yet
- Comparative Efficacy of Clindamycin Versus Erythromycin in Eradication of AntenatalDocument7 pagesComparative Efficacy of Clindamycin Versus Erythromycin in Eradication of AntenatalSamuel ManurungNo ratings yet
- Intranasal Ketamine For Procedural Sedation and Analgesia in Children: A Systematic ReviewDocument15 pagesIntranasal Ketamine For Procedural Sedation and Analgesia in Children: A Systematic ReviewNADIA VICUÑA CRIADONo ratings yet
- Journal of Pediatric Surgery: Steven L. Lee, Lara Spence, Kyle Mock, James X. Wu, Huan Yan, Daniel A. DeugarteDocument6 pagesJournal of Pediatric Surgery: Steven L. Lee, Lara Spence, Kyle Mock, James X. Wu, Huan Yan, Daniel A. DeugarteMelian AnitaNo ratings yet
- Coates 2016Document2 pagesCoates 2016FebbyNo ratings yet
- Epinephrine and Dexamethasone in Children With BronchiolitisDocument11 pagesEpinephrine and Dexamethasone in Children With BronchiolitisAdelina Wahyuni LubisNo ratings yet
- Comparison of Outcomes of The Epley and Self-Epley Maneuvers inDocument5 pagesComparison of Outcomes of The Epley and Self-Epley Maneuvers inYunie ArmyatiNo ratings yet
- CroupDocument7 pagesCroupnadiaNo ratings yet
- challengesInTheDesignThea 1Document6 pageschallengesInTheDesignThea 1Zolla Verbianti SuwitaNo ratings yet
- Perforated Appendicitis PDFDocument8 pagesPerforated Appendicitis PDFMuhammad AkrimNo ratings yet
- A Multicenter, Double Blind Comparison of - MCLINN, SAMUELDocument15 pagesA Multicenter, Double Blind Comparison of - MCLINN, SAMUELPutri FebrinaNo ratings yet
- Synopsis: ST John'S College of NursingDocument19 pagesSynopsis: ST John'S College of NursingsyarifaNo ratings yet
- Goal-Directed Resuscitation For Patients With Early Septic ShockDocument11 pagesGoal-Directed Resuscitation For Patients With Early Septic ShockmmsNo ratings yet
- Anesthetic Practices For Patients With Preeclampsia or HELLP Syndrome: A SurveyDocument6 pagesAnesthetic Practices For Patients With Preeclampsia or HELLP Syndrome: A SurveyYan Hein TanawaniNo ratings yet
- Hidrogel LanolinaDocument10 pagesHidrogel LanolinagldsbarzolaNo ratings yet
- C01110916 PDFDocument8 pagesC01110916 PDFLestari Chye PouedanNo ratings yet
- Ecet Kaki94Document5 pagesEcet Kaki94Dian NovitasariNo ratings yet
- Archdischfn00035 0041Document5 pagesArchdischfn00035 0041Dian NovitasariNo ratings yet
- Wang2017 Oxcarbazepine Oral Suspension in Pediatric Patients WithDocument9 pagesWang2017 Oxcarbazepine Oral Suspension in Pediatric Patients WithGabriela WidjajaNo ratings yet
- Eria 3Document15 pagesEria 3ruth angelinaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Back To School Infographics by SlidesgoDocument37 pagesBack To School Infographics by SlidesgoRaudhah SimahateNo ratings yet
- Soal Nomor 1: Sgot/Sgpt Hemoglobin Trigliserid Totalkolestrol HDL LDL N Valid Missing Mean Std. DeviationDocument18 pagesSoal Nomor 1: Sgot/Sgpt Hemoglobin Trigliserid Totalkolestrol HDL LDL N Valid Missing Mean Std. DeviationRaudhah SimahateNo ratings yet
- Continue: Erb's Palsy Adalah PDFDocument3 pagesContinue: Erb's Palsy Adalah PDFRaudhah SimahateNo ratings yet
- Dwi Putri Tania (04011181621024)Document34 pagesDwi Putri Tania (04011181621024)Raudhah SimahateNo ratings yet
- Kubba 2001 (Intervention For Recurren Idiopathix Epistaksis in ChildrenDocument26 pagesKubba 2001 (Intervention For Recurren Idiopathix Epistaksis in ChildrenRaudhah SimahateNo ratings yet
- Lembar Jawaban Skill Lab EbmDocument6 pagesLembar Jawaban Skill Lab EbmRaudhah SimahateNo ratings yet
- Internet Gaming Disorder in The DSM-5: Psychiatric Diagnosis (MB First, Section Editor)Document9 pagesInternet Gaming Disorder in The DSM-5: Psychiatric Diagnosis (MB First, Section Editor)Raudhah SimahateNo ratings yet
- How Treatment Anemia in PregnancyDocument36 pagesHow Treatment Anemia in PregnancyRaudhah SimahateNo ratings yet
- The Impact of Internet and Videogaming Addiction On Adolescent Vision: A Review of The LiteratureDocument6 pagesThe Impact of Internet and Videogaming Addiction On Adolescent Vision: A Review of The LiteratureRaudhah SimahateNo ratings yet
- Ethical Case StudiesDocument9 pagesEthical Case StudiesًNo ratings yet
- Laparoscopic Common Bile Duct ExplorationDocument2 pagesLaparoscopic Common Bile Duct ExplorationmhmmdfaizalNo ratings yet
- Spatial Infant MDocument9 pagesSpatial Infant MBezan MeleseNo ratings yet
- Sitrep - Issue 20Document6 pagesSitrep - Issue 20Tupye TutuNo ratings yet
- Fatty AcidDocument2 pagesFatty AcidFahad AhmedNo ratings yet
- Medical Surgical Nursing Assessment and Management of Clinical Problems Lewis 8th Edition Test BankDocument10 pagesMedical Surgical Nursing Assessment and Management of Clinical Problems Lewis 8th Edition Test BankMark Bureau100% (33)
- Occupational Therapy For Rheumatoid Arthritis: A Systematic ReviewDocument14 pagesOccupational Therapy For Rheumatoid Arthritis: A Systematic ReviewispasNo ratings yet
- Chapages Lusanta 3Document137 pagesChapages Lusanta 3Mary Jiel Dionesio LansanganNo ratings yet
- Budiyono2018 PDFDocument14 pagesBudiyono2018 PDFTIRTA JATINo ratings yet
- EDU 404 Course OutlineDocument3 pagesEDU 404 Course OutlineMoses Akano OluwaseunNo ratings yet
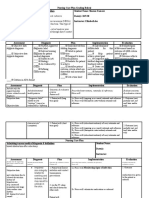
- Nursing Care Plan Template and Grading RubricDocument4 pagesNursing Care Plan Template and Grading RubricSharon TanveerNo ratings yet
- Dental Insurance: Types of Dental PlansDocument5 pagesDental Insurance: Types of Dental PlansVishal ThakkarNo ratings yet
- Case Study: "Burn Injury"Document24 pagesCase Study: "Burn Injury"ChAtmaRosE100% (1)
- Final Research Paper 2Document9 pagesFinal Research Paper 2api-510720092No ratings yet
- Understanding Your Scores On The Emotional Intelligence Self-Assessment ScaleDocument2 pagesUnderstanding Your Scores On The Emotional Intelligence Self-Assessment ScaleFarhat MansuriNo ratings yet
- Routes of Drug AdministrationDocument34 pagesRoutes of Drug AdministrationNa SyaNo ratings yet
- Standard Operating Procedure (Sop) Collecting Swab or Rinse Samples For Chemical and Microbiological AnalysisDocument11 pagesStandard Operating Procedure (Sop) Collecting Swab or Rinse Samples For Chemical and Microbiological AnalysisAbuNo ratings yet
- Safety Data Sheet: Basonat® HI 100 NGDocument17 pagesSafety Data Sheet: Basonat® HI 100 NGRıdvan SürmeliNo ratings yet
- Antiscale (DEQUEST SPE 0001)Document7 pagesAntiscale (DEQUEST SPE 0001)mahdi rasoulianNo ratings yet
- The National Bursary PolicyDocument20 pagesThe National Bursary PolicyCrazyCrafterYTNo ratings yet
- Moving Meditation of SilambamDocument4 pagesMoving Meditation of SilambamGabrielNo ratings yet
- (Template) DVTDocument21 pages(Template) DVTPema Lamu TdkNo ratings yet
- Clement Clarke 100 Year Anniversary BookDocument28 pagesClement Clarke 100 Year Anniversary BookHaag-Streit UK (HS-UK)No ratings yet
- Writers Craft Essay 2Document3 pagesWriters Craft Essay 2api-538026223No ratings yet
- ExamDocument67 pagesExamJOHN CARLO APATANNo ratings yet
- Transient Neonatal Hypocalcemia: Presentation and Outcomes: AuthorsDocument7 pagesTransient Neonatal Hypocalcemia: Presentation and Outcomes: AuthorsMeryNo ratings yet
- Ethics Unit 2Document22 pagesEthics Unit 2SaniNo ratings yet
- 5 Sciatica Exercises For Pain Relief (With Pictures) : Back IntelligenceDocument26 pages5 Sciatica Exercises For Pain Relief (With Pictures) : Back Intelligenceanand sahu100% (1)
- Return Permit For Resident Outside UAEDocument3 pagesReturn Permit For Resident Outside UAEᘉᓋᘻᗗᘙ ᘉᓋᙏᓲ ᖽᐸᗁᕠᘘNo ratings yet

































































































Download as pdf or txt
You might also like
- Acute and Chronic Wounds - Current Management Concepts (PDFDrive)Document1,872 pagesAcute and Chronic Wounds - Current Management Concepts (PDFDrive)Tasha FarahNo ratings yet
- Vitiligo ObatDocument6 pagesVitiligo ObatLidwina DewiNo ratings yet
- Primary Operative Versus Nonoperative Therapy For Pediatric Empyema: A Meta-AnalysisDocument9 pagesPrimary Operative Versus Nonoperative Therapy For Pediatric Empyema: A Meta-AnalysisDr Nilesh NagdeveNo ratings yet
- Comparison of Amoxicillin/Clavulanic Acid High Dose With Cef Dinir in The Treatment of Acute Otitis MediaDocument8 pagesComparison of Amoxicillin/Clavulanic Acid High Dose With Cef Dinir in The Treatment of Acute Otitis Mediaenggainget8663No ratings yet
- Pediatric Pharmacology and TherapeuticsDocument6 pagesPediatric Pharmacology and TherapeuticsRatna SriwahyuniNo ratings yet
- Nejmoa1911998 PDFDocument11 pagesNejmoa1911998 PDFStella NoviaNo ratings yet
- Sample Critics RTCDocument12 pagesSample Critics RTCGada NagariNo ratings yet
- Journal of Pediatric Surgery: Indepent Review ArticlesDocument4 pagesJournal of Pediatric Surgery: Indepent Review ArticlesNur Ainatun NadrahNo ratings yet
- JURNAL READINGnejmoa1007174Document11 pagesJURNAL READINGnejmoa1007174Sukma WinahyuNo ratings yet
- Pediatrics 1981 Gunn 61 7Document9 pagesPediatrics 1981 Gunn 61 7Marlon SoselisaNo ratings yet
- Clinical Profile of Empyema in Tertiary Health Care Center, HyderabadDocument4 pagesClinical Profile of Empyema in Tertiary Health Care Center, HyderabadririNo ratings yet
- Short-Course Antimicrobial Therapy For Pediatric Community-Acquired Pneumonia - PMCDocument19 pagesShort-Course Antimicrobial Therapy For Pediatric Community-Acquired Pneumonia - PMCFrances Jean T. DoblasNo ratings yet
- Current Success in The Treatment of Intussusception in ChildrenDocument9 pagesCurrent Success in The Treatment of Intussusception in ChildrenOby RomdhoniNo ratings yet
- Complementary Therapies in Medicine: Contents Lists Available atDocument13 pagesComplementary Therapies in Medicine: Contents Lists Available atAndi UmmahNo ratings yet
- 2518-Article Text-13816-1-10-20201215Document6 pages2518-Article Text-13816-1-10-20201215JAN CAMILLE LENONNo ratings yet
- Scopus (29) Many2017Document7 pagesScopus (29) Many2017ika puspitaNo ratings yet
- Role of Dexamethasone in Neonatal Meningitis 2012Document6 pagesRole of Dexamethasone in Neonatal Meningitis 2012jose alberto gamboaNo ratings yet
- 403 Full PDFDocument2 pages403 Full PDFMafia 12mia5No ratings yet
- PXW 011Document5 pagesPXW 011rendyjiwonoNo ratings yet
- 976 FullDocument6 pages976 FullazifadewiatasyaNo ratings yet
- To Study The Effectiveness of Oral Azithromycin As Compared To Parenteral Ceftriaxone in The Treatment of Uncomplicated Enteric FeverDocument5 pagesTo Study The Effectiveness of Oral Azithromycin As Compared To Parenteral Ceftriaxone in The Treatment of Uncomplicated Enteric FeverSari MustikaNo ratings yet
- Epilepsy in Tubero Sclerosis ComplexDocument7 pagesEpilepsy in Tubero Sclerosis ComplexDenny SigarlakiNo ratings yet
- Fetal Inflamatory Response SyndromeDocument9 pagesFetal Inflamatory Response SyndromeAnonymous mvNUtwidNo ratings yet
- Jurnal Sidang RespiDocument4 pagesJurnal Sidang RespiAnis Eka SukmadadariNo ratings yet
- Comparison of Two Different Antibiotic Regimens For The Prophylaxisis of Cases With Preterm Premature Rupture of Membranes: A Randomized Clinical TrialDocument5 pagesComparison of Two Different Antibiotic Regimens For The Prophylaxisis of Cases With Preterm Premature Rupture of Membranes: A Randomized Clinical TrialVindee VictoryNo ratings yet
- Chamnanvanakij, 2005Document6 pagesChamnanvanakij, 2005Fatma ElzaytNo ratings yet
- Chloramphenicol Treatment For Acute Infective Conjunctivitis in Children in Primary Care: A Randomised Double-Blind Placebo-Controlled TrialDocument8 pagesChloramphenicol Treatment For Acute Infective Conjunctivitis in Children in Primary Care: A Randomised Double-Blind Placebo-Controlled TrialFemi OdeNo ratings yet
- Perbandingan Efektifitas Kloramfenikol Dan Gentamisin Pada Dakriosistitis BayiDocument7 pagesPerbandingan Efektifitas Kloramfenikol Dan Gentamisin Pada Dakriosistitis BayiChristian SolihinNo ratings yet
- Management of Rectal Prolapse in ChildrenDocument6 pagesManagement of Rectal Prolapse in ChildrenWaNda GrNo ratings yet
- Treatment of Acute Otitis Media in Children Under 2 Years of AgeDocument29 pagesTreatment of Acute Otitis Media in Children Under 2 Years of AgesellyhdelhiNo ratings yet
- Thoracoscopic Decortication Vs Tube Thoracostomy With Fibrinolysis For Empyema in Children: A Prospective, Randomized TrialDocument6 pagesThoracoscopic Decortication Vs Tube Thoracostomy With Fibrinolysis For Empyema in Children: A Prospective, Randomized TrialcarlaNo ratings yet
- Sedation and Analgesia in Children Undergoing Invasive ProceduresDocument7 pagesSedation and Analgesia in Children Undergoing Invasive ProceduresSantosa TandiNo ratings yet
- Neonatal Mastitis: Controversies in Management: October 2012Document5 pagesNeonatal Mastitis: Controversies in Management: October 2012ditaNo ratings yet
- CAP - Risk Factors and TreatmentDocument5 pagesCAP - Risk Factors and Treatmentgrool29rNo ratings yet
- Early Analgesia For Children With Acute Abdominal Pain: ObjectivesDocument8 pagesEarly Analgesia For Children With Acute Abdominal Pain: Objectivescrizt tyanNo ratings yet
- With Intravenous Antibiotics Urinary Tract Infections in 1-To 3-Month-Old Infants: Ambulatory TreatmentDocument9 pagesWith Intravenous Antibiotics Urinary Tract Infections in 1-To 3-Month-Old Infants: Ambulatory Treatmentsri_jva8No ratings yet
- Piis1474442208701418 PDFDocument8 pagesPiis1474442208701418 PDFsebastian quiroz floresNo ratings yet
- Comparison Between Small and Large Bowel Intussusception in ChildrenDocument3 pagesComparison Between Small and Large Bowel Intussusception in ChildrenParamartha KesumaNo ratings yet
- 1 s2.0 S0002937899707039 MainDocument5 pages1 s2.0 S0002937899707039 MainPutri AgriNo ratings yet
- Kim 2015Document4 pagesKim 2015ruthameliapNo ratings yet
- Comparative Efficacy of Clindamycin Versus Erythromycin in Eradication of AntenatalDocument7 pagesComparative Efficacy of Clindamycin Versus Erythromycin in Eradication of AntenatalSamuel ManurungNo ratings yet
- Intranasal Ketamine For Procedural Sedation and Analgesia in Children: A Systematic ReviewDocument15 pagesIntranasal Ketamine For Procedural Sedation and Analgesia in Children: A Systematic ReviewNADIA VICUÑA CRIADONo ratings yet
- Journal of Pediatric Surgery: Steven L. Lee, Lara Spence, Kyle Mock, James X. Wu, Huan Yan, Daniel A. DeugarteDocument6 pagesJournal of Pediatric Surgery: Steven L. Lee, Lara Spence, Kyle Mock, James X. Wu, Huan Yan, Daniel A. DeugarteMelian AnitaNo ratings yet
- Coates 2016Document2 pagesCoates 2016FebbyNo ratings yet
- Epinephrine and Dexamethasone in Children With BronchiolitisDocument11 pagesEpinephrine and Dexamethasone in Children With BronchiolitisAdelina Wahyuni LubisNo ratings yet
- Comparison of Outcomes of The Epley and Self-Epley Maneuvers inDocument5 pagesComparison of Outcomes of The Epley and Self-Epley Maneuvers inYunie ArmyatiNo ratings yet
- CroupDocument7 pagesCroupnadiaNo ratings yet
- challengesInTheDesignThea 1Document6 pageschallengesInTheDesignThea 1Zolla Verbianti SuwitaNo ratings yet
- Perforated Appendicitis PDFDocument8 pagesPerforated Appendicitis PDFMuhammad AkrimNo ratings yet
- A Multicenter, Double Blind Comparison of - MCLINN, SAMUELDocument15 pagesA Multicenter, Double Blind Comparison of - MCLINN, SAMUELPutri FebrinaNo ratings yet
- Synopsis: ST John'S College of NursingDocument19 pagesSynopsis: ST John'S College of NursingsyarifaNo ratings yet
- Goal-Directed Resuscitation For Patients With Early Septic ShockDocument11 pagesGoal-Directed Resuscitation For Patients With Early Septic ShockmmsNo ratings yet
- Anesthetic Practices For Patients With Preeclampsia or HELLP Syndrome: A SurveyDocument6 pagesAnesthetic Practices For Patients With Preeclampsia or HELLP Syndrome: A SurveyYan Hein TanawaniNo ratings yet
- Hidrogel LanolinaDocument10 pagesHidrogel LanolinagldsbarzolaNo ratings yet
- C01110916 PDFDocument8 pagesC01110916 PDFLestari Chye PouedanNo ratings yet
- Ecet Kaki94Document5 pagesEcet Kaki94Dian NovitasariNo ratings yet
- Archdischfn00035 0041Document5 pagesArchdischfn00035 0041Dian NovitasariNo ratings yet
- Wang2017 Oxcarbazepine Oral Suspension in Pediatric Patients WithDocument9 pagesWang2017 Oxcarbazepine Oral Suspension in Pediatric Patients WithGabriela WidjajaNo ratings yet
- Eria 3Document15 pagesEria 3ruth angelinaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Back To School Infographics by SlidesgoDocument37 pagesBack To School Infographics by SlidesgoRaudhah SimahateNo ratings yet
- Soal Nomor 1: Sgot/Sgpt Hemoglobin Trigliserid Totalkolestrol HDL LDL N Valid Missing Mean Std. DeviationDocument18 pagesSoal Nomor 1: Sgot/Sgpt Hemoglobin Trigliserid Totalkolestrol HDL LDL N Valid Missing Mean Std. DeviationRaudhah SimahateNo ratings yet
- Continue: Erb's Palsy Adalah PDFDocument3 pagesContinue: Erb's Palsy Adalah PDFRaudhah SimahateNo ratings yet
- Dwi Putri Tania (04011181621024)Document34 pagesDwi Putri Tania (04011181621024)Raudhah SimahateNo ratings yet
- Kubba 2001 (Intervention For Recurren Idiopathix Epistaksis in ChildrenDocument26 pagesKubba 2001 (Intervention For Recurren Idiopathix Epistaksis in ChildrenRaudhah SimahateNo ratings yet
- Lembar Jawaban Skill Lab EbmDocument6 pagesLembar Jawaban Skill Lab EbmRaudhah SimahateNo ratings yet
- Internet Gaming Disorder in The DSM-5: Psychiatric Diagnosis (MB First, Section Editor)Document9 pagesInternet Gaming Disorder in The DSM-5: Psychiatric Diagnosis (MB First, Section Editor)Raudhah SimahateNo ratings yet
- How Treatment Anemia in PregnancyDocument36 pagesHow Treatment Anemia in PregnancyRaudhah SimahateNo ratings yet
- The Impact of Internet and Videogaming Addiction On Adolescent Vision: A Review of The LiteratureDocument6 pagesThe Impact of Internet and Videogaming Addiction On Adolescent Vision: A Review of The LiteratureRaudhah SimahateNo ratings yet
- Ethical Case StudiesDocument9 pagesEthical Case StudiesًNo ratings yet
- Laparoscopic Common Bile Duct ExplorationDocument2 pagesLaparoscopic Common Bile Duct ExplorationmhmmdfaizalNo ratings yet
- Spatial Infant MDocument9 pagesSpatial Infant MBezan MeleseNo ratings yet
- Sitrep - Issue 20Document6 pagesSitrep - Issue 20Tupye TutuNo ratings yet
- Fatty AcidDocument2 pagesFatty AcidFahad AhmedNo ratings yet
- Medical Surgical Nursing Assessment and Management of Clinical Problems Lewis 8th Edition Test BankDocument10 pagesMedical Surgical Nursing Assessment and Management of Clinical Problems Lewis 8th Edition Test BankMark Bureau100% (33)
- Occupational Therapy For Rheumatoid Arthritis: A Systematic ReviewDocument14 pagesOccupational Therapy For Rheumatoid Arthritis: A Systematic ReviewispasNo ratings yet
- Chapages Lusanta 3Document137 pagesChapages Lusanta 3Mary Jiel Dionesio LansanganNo ratings yet
- Budiyono2018 PDFDocument14 pagesBudiyono2018 PDFTIRTA JATINo ratings yet
- EDU 404 Course OutlineDocument3 pagesEDU 404 Course OutlineMoses Akano OluwaseunNo ratings yet
- Nursing Care Plan Template and Grading RubricDocument4 pagesNursing Care Plan Template and Grading RubricSharon TanveerNo ratings yet
- Dental Insurance: Types of Dental PlansDocument5 pagesDental Insurance: Types of Dental PlansVishal ThakkarNo ratings yet
- Case Study: "Burn Injury"Document24 pagesCase Study: "Burn Injury"ChAtmaRosE100% (1)
- Final Research Paper 2Document9 pagesFinal Research Paper 2api-510720092No ratings yet
- Understanding Your Scores On The Emotional Intelligence Self-Assessment ScaleDocument2 pagesUnderstanding Your Scores On The Emotional Intelligence Self-Assessment ScaleFarhat MansuriNo ratings yet
- Routes of Drug AdministrationDocument34 pagesRoutes of Drug AdministrationNa SyaNo ratings yet
- Standard Operating Procedure (Sop) Collecting Swab or Rinse Samples For Chemical and Microbiological AnalysisDocument11 pagesStandard Operating Procedure (Sop) Collecting Swab or Rinse Samples For Chemical and Microbiological AnalysisAbuNo ratings yet
- Safety Data Sheet: Basonat® HI 100 NGDocument17 pagesSafety Data Sheet: Basonat® HI 100 NGRıdvan SürmeliNo ratings yet
- Antiscale (DEQUEST SPE 0001)Document7 pagesAntiscale (DEQUEST SPE 0001)mahdi rasoulianNo ratings yet
- The National Bursary PolicyDocument20 pagesThe National Bursary PolicyCrazyCrafterYTNo ratings yet
- Moving Meditation of SilambamDocument4 pagesMoving Meditation of SilambamGabrielNo ratings yet
- (Template) DVTDocument21 pages(Template) DVTPema Lamu TdkNo ratings yet
- Clement Clarke 100 Year Anniversary BookDocument28 pagesClement Clarke 100 Year Anniversary BookHaag-Streit UK (HS-UK)No ratings yet
- Writers Craft Essay 2Document3 pagesWriters Craft Essay 2api-538026223No ratings yet
- ExamDocument67 pagesExamJOHN CARLO APATANNo ratings yet
- Transient Neonatal Hypocalcemia: Presentation and Outcomes: AuthorsDocument7 pagesTransient Neonatal Hypocalcemia: Presentation and Outcomes: AuthorsMeryNo ratings yet
- Ethics Unit 2Document22 pagesEthics Unit 2SaniNo ratings yet
- 5 Sciatica Exercises For Pain Relief (With Pictures) : Back IntelligenceDocument26 pages5 Sciatica Exercises For Pain Relief (With Pictures) : Back Intelligenceanand sahu100% (1)
- Return Permit For Resident Outside UAEDocument3 pagesReturn Permit For Resident Outside UAEᘉᓋᘻᗗᘙ ᘉᓋᙏᓲ ᖽᐸᗁᕠᘘNo ratings yet