Download as pdf or txt
You might also like
- Benzodiazepine Comparison Chart - Commonly Available Sedative Hypnotic Anti Anxiety (Anxiolytic) Anti Epileptic MedicationsDocument2 pagesBenzodiazepine Comparison Chart - Commonly Available Sedative Hypnotic Anti Anxiety (Anxiolytic) Anti Epileptic MedicationsChristopher Chrysostom100% (3)
- Questionnaire For Food PricesDocument1 pageQuestionnaire For Food PricesTerrissa67% (3)
- Section 1 Treatment of Depression May 2021Document13 pagesSection 1 Treatment of Depression May 2021Reem AbuziedNo ratings yet
- Antihistamine Dose ChartDocument1 pageAntihistamine Dose ChartKerin KNo ratings yet
- Opioid Equianalgesic Table EtcDocument2 pagesOpioid Equianalgesic Table EtcHerrera MiguelNo ratings yet
- Essential Medicine in Saudi ArabiaDocument11 pagesEssential Medicine in Saudi ArabiaEman MohamedNo ratings yet
- 2020 Ed Dilution ProtocolDocument72 pages2020 Ed Dilution ProtocolTuan SharatulNo ratings yet
- Daftar Obat Siap Tersedia DR Sumber Luar 2018Document8 pagesDaftar Obat Siap Tersedia DR Sumber Luar 2018tripurwaniNo ratings yet
- Treatment of Common SymptomsDocument12 pagesTreatment of Common Symptomsxjunhao100% (3)
- Tapentadol Dose Conversion Chart FinalDocument1 pageTapentadol Dose Conversion Chart FinalMehroze SalmanNo ratings yet
- Activity 8Document5 pagesActivity 8HEXALANE E. LABRADORNo ratings yet
- CNS Drugs Pharmaceutical Form Therapeutic Group: 6mg, 8mgDocument7 pagesCNS Drugs Pharmaceutical Form Therapeutic Group: 6mg, 8mgCha GabrielNo ratings yet
- Gastrointestinal Tract Drugs: Pharmacist Marwan QasimDocument20 pagesGastrointestinal Tract Drugs: Pharmacist Marwan QasimWaliNo ratings yet
- LTC-Parkinsonism 1079Document1 pageLTC-Parkinsonism 1079DanielleNo ratings yet
- GP/Locum Drug List - 5 May 2013: RespiratoryDocument14 pagesGP/Locum Drug List - 5 May 2013: RespiratoryAdam ChungNo ratings yet
- Anaesthetics: Kiribati Essential Drugs List (Revised March 2009)Document12 pagesAnaesthetics: Kiribati Essential Drugs List (Revised March 2009)portosinNo ratings yet
- ValuesDocument1 pageValuesphelvskevinNo ratings yet
- Formularium Rs KambangDocument56 pagesFormularium Rs KambangNora SadanaNo ratings yet
- BenzodiazepinesDocument20 pagesBenzodiazepinesfarmasi_hmNo ratings yet
- Tugas Individu - Nur Indah Sari (PO713251201030) - 1Document6 pagesTugas Individu - Nur Indah Sari (PO713251201030) - 1Nur indah sariNo ratings yet
- Parent Her AlDocument29 pagesParent Her AlshannyNo ratings yet
- ACTIVITY ON MEDICINES-KeyDocument5 pagesACTIVITY ON MEDICINES-KeyPATRICIA ROSE SORIANONo ratings yet
- Penggunaan BenzodiazepinDocument7 pagesPenggunaan BenzodiazepinNajib Al FatinNo ratings yet
- Antidiabetic AgentsDocument2 pagesAntidiabetic AgentsDanielleNo ratings yet
- Medicamento Dosis Vxdía Presentación ComercialDocument2 pagesMedicamento Dosis Vxdía Presentación ComercialIsmal MachacaNo ratings yet
- Combine PDFDocument44 pagesCombine PDFruang belajar farmasiNo ratings yet
- Daftar Dosis Dan Sediaan Obat KardiovaskularDocument2 pagesDaftar Dosis Dan Sediaan Obat KardiovaskularnadiaNo ratings yet
- Opioid Tapering Flow Sheet: Start HereDocument2 pagesOpioid Tapering Flow Sheet: Start HeregegeNo ratings yet
- A3 COVID EoL Drugs Table V1 5Document2 pagesA3 COVID EoL Drugs Table V1 5Tim BrownNo ratings yet
- A3 COVID EoL Drugs Table V1 - 5Document2 pagesA3 COVID EoL Drugs Table V1 - 5Tim BrownNo ratings yet
- Dosis Obat AnakDocument3 pagesDosis Obat Anakimam mulyadiNo ratings yet
- Dosis Obat AnakDocument3 pagesDosis Obat AnakhannaNo ratings yet
- Remedi Standard Acute Medicine List (Formulary) 2021: Who We AreDocument9 pagesRemedi Standard Acute Medicine List (Formulary) 2021: Who We AreWayne LinksNo ratings yet
- MPR-MS (Muscle Spasm) - 1299Document1 pageMPR-MS (Muscle Spasm) - 1299DanielleNo ratings yet
- Daftar Obat High Alert & LasaDocument2 pagesDaftar Obat High Alert & LasaMoy KecilNo ratings yet
- Emergency DrugsDocument5 pagesEmergency DrugsRalp ManglicmotNo ratings yet
- J Partn R RM y Cart Ist: F S Cras SuppDocument2 pagesJ Partn R RM y Cart Ist: F S Cras SuppMatthew DelaneyNo ratings yet
- Mpr-Aa (Diabetes) - 2pt (67) - 1127Document2 pagesMpr-Aa (Diabetes) - 2pt (67) - 1127Edmond ChanNo ratings yet
- Benzodiazepine Equivalents DassaDocument2 pagesBenzodiazepine Equivalents DassaPsikiater PanturaNo ratings yet
- 1: Adhd: Scientific Name Dose CommentsDocument4 pages1: Adhd: Scientific Name Dose CommentsSadiq Abdo92No ratings yet
- New Microsoft Word DocumentDocument3 pagesNew Microsoft Word DocumentMuhammad Haris Khan KhattakNo ratings yet
- 8.2.1.6 Form ObatDocument20 pages8.2.1.6 Form ObatwandiNo ratings yet
- Standarisari ObatDocument28 pagesStandarisari Obatmelisa memelNo ratings yet
- Asam Tranexamat Betahistin BicolaxDocument2 pagesAsam Tranexamat Betahistin BicolaxSyahidatul ArifaNo ratings yet
- Drug DilutionDocument4 pagesDrug Dilutiondr.rrajesh92No ratings yet
- Obat Muntah HamilDocument6 pagesObat Muntah HamilIlham KurniawanNo ratings yet
- Patient Information Leaflet: ABOUT Your MedicineDocument3 pagesPatient Information Leaflet: ABOUT Your MedicineFitria Nusa Eka PratiwyNo ratings yet
- Pediatric DosageDocument2 pagesPediatric DosageAllene PaderangaNo ratings yet
- 10mkday X 3 5 Day 10 Mkday 1 Day The 2-5 5 Mkday: Solve MkdoseDocument2 pages10mkday X 3 5 Day 10 Mkday 1 Day The 2-5 5 Mkday: Solve Mkdoseนีล ไบรอันNo ratings yet
- Group 1Document46 pagesGroup 1Raghda NimerNo ratings yet
- Dhian Rachma M - 20340073 - Tugas Penggolongan ObatDocument5 pagesDhian Rachma M - 20340073 - Tugas Penggolongan ObatRachmaNo ratings yet
- Dhian Rachma M - 20340073 - Tugas Penggolongan ObatDocument5 pagesDhian Rachma M - 20340073 - Tugas Penggolongan ObatRachmaNo ratings yet
- PrescribingDocument2 pagesPrescribingPei Xing KwekNo ratings yet
- Dosis PCT 10mg/kg/× Ibuprofen 5-10mg/kg/xDocument3 pagesDosis PCT 10mg/kg/× Ibuprofen 5-10mg/kg/xdeaaannnnnnNo ratings yet
- Daftar Obat High Alert 2017Document1 pageDaftar Obat High Alert 2017suherti100% (1)
- Perspectives in PharmacyDocument9 pagesPerspectives in PharmacyPRECIOUS FAITH PALMANo ratings yet
- Addendum To The List of Vat Exempt Drugs Nov 2019Document2 pagesAddendum To The List of Vat Exempt Drugs Nov 2019sc law officeNo ratings yet
- Teen Sex Trafficking & Sexual Exploitation Awareness Brochure For School AdministrationDocument6 pagesTeen Sex Trafficking & Sexual Exploitation Awareness Brochure For School AdministrationmccaininstituteNo ratings yet
- AngioplastyDocument45 pagesAngioplastym maskNo ratings yet
- Low Cost PVC CrutchesDocument2 pagesLow Cost PVC CrutchesMohd Asri TaipNo ratings yet
- 30 Days of Yoga Challenge CalendarDocument1 page30 Days of Yoga Challenge CalendarअनितNo ratings yet
- Hearing Aid DataDocument16 pagesHearing Aid DataUdayan AwasthiNo ratings yet
- Herbs - Invigorate BloodDocument13 pagesHerbs - Invigorate BloodyayanicaNo ratings yet
- Competence Vs QualificationDocument25 pagesCompetence Vs QualificationJohn OoNo ratings yet
- Historical Development of Community Health and Community Health Nursing in India and WorldDocument37 pagesHistorical Development of Community Health and Community Health Nursing in India and WorldAni mathewNo ratings yet
- IFPO SO Risks Competencies 1stDocument89 pagesIFPO SO Risks Competencies 1stqadeer386No ratings yet
- Advanced Medicine Recall-A Must For MRCPDocument712 pagesAdvanced Medicine Recall-A Must For MRCPDr Sumant Sharma80% (5)
- Porque Necesitamos Suplementos 2Document6 pagesPorque Necesitamos Suplementos 2Fabio DiezNo ratings yet
- Pages From ASHRAE HVAC Design Manual For Hospitals and Clinics, 2nd Ed. PDFDocument4 pagesPages From ASHRAE HVAC Design Manual For Hospitals and Clinics, 2nd Ed. PDFAhmed Rabie Abd ElazeemNo ratings yet
- Harmful Traditional PracticesDocument2 pagesHarmful Traditional PracticesFentahun Ze WoinambaNo ratings yet
- Medical Library AssociationsDocument7 pagesMedical Library AssociationsYamna Irfan SiddiquiNo ratings yet
- Growth Drivers For QuornDocument2 pagesGrowth Drivers For Quornkyla christineNo ratings yet
- Updated PPO (Preffered Provider Organization) List December 2018Document8 pagesUpdated PPO (Preffered Provider Organization) List December 2018Uttam GolderNo ratings yet
- Units 6-10 AssessmentDocument9 pagesUnits 6-10 AssessmentNguyen Thanh Thang PH 1 6 5 8 4No ratings yet
- The Anchorage Bend in The Begg TechniqueDocument7 pagesThe Anchorage Bend in The Begg TechniqueSyed Mohammad Osama AhsanNo ratings yet
- Periodontal PocketsDocument51 pagesPeriodontal PocketsShawqi ANo ratings yet
- SpankingDocument7 pagesSpankingNicole PicardNo ratings yet
- NFPA-Hot Work Fact Sheet5Document2 pagesNFPA-Hot Work Fact Sheet5Laxminarayan NayakNo ratings yet
- Neuro Type 2A and Best Damn Workout - Christian Thibaudeau Coaching - Forums - T NationDocument4 pagesNeuro Type 2A and Best Damn Workout - Christian Thibaudeau Coaching - Forums - T NationVladimir OlefirenkoNo ratings yet
- Hallucinations Rating Scale - SAMPLEDocument3 pagesHallucinations Rating Scale - SAMPLETauqeer AhmedNo ratings yet
- Chapter 1 5Document132 pagesChapter 1 5Kylle AlimosaNo ratings yet
- Organ Donation PresentationDocument40 pagesOrgan Donation PresentationKryza Dale Bunado Batican100% (1)
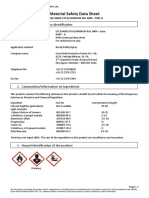
- Msds - Exlthane 570 Aluminium Ral 9006Document6 pagesMsds - Exlthane 570 Aluminium Ral 9006Okpeke EneNo ratings yet
- Original PDF Esska Instructional Course Lecture Book Glasgow 2018 PDFDocument41 pagesOriginal PDF Esska Instructional Course Lecture Book Glasgow 2018 PDFpatricia.morrison594100% (39)
- Test Bank For Mechanical Ventilation 7th Edition J M CairoDocument13 pagesTest Bank For Mechanical Ventilation 7th Edition J M CairocalliopesilasaagyNo ratings yet
- Case - Study - A - Questions (1) 2Document5 pagesCase - Study - A - Questions (1) 2ReaganNo ratings yet