Download as pdf or txt
You might also like
- 1 The Basics 1Document19 pages1 The Basics 11202blackNo ratings yet
- Republic of The Philippines Nueva Vizcaya State University Bayombong, Nueva VizcayaDocument8 pagesRepublic of The Philippines Nueva Vizcaya State University Bayombong, Nueva VizcayaNica Hannah100% (2)
- Conceptual and Philosophical Foundations of Professional Nursing PracticeDocument36 pagesConceptual and Philosophical Foundations of Professional Nursing PracticeDip Ayan MNo ratings yet
- The Education of Nurses On The Leading Edge of TransformationDocument31 pagesThe Education of Nurses On The Leading Edge of TransformationDip Ayan M100% (2)
- Fluid Balance Monitoring PosterDocument1 pageFluid Balance Monitoring PosterSania oktaNo ratings yet
- K Sembulingam Essentials of Medical Physiology 6th 008Document7 pagesK Sembulingam Essentials of Medical Physiology 6th 008Hajara Abubakari SadiqNo ratings yet
- Fluid BalanceCorr PDFDocument5 pagesFluid BalanceCorr PDFSu'ud DeLoco's100% (1)
- Fluid Management For Critically Ill PatientDocument7 pagesFluid Management For Critically Ill PatientNatalindah Jokiem Woecandra T. D.No ratings yet
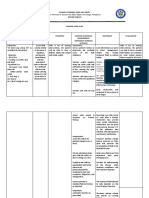
- Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan Assessment Diagnosis Planning Intervention Rationale EvaluationMiss GNo ratings yet
- Tor ElekDocument9 pagesTor ElekChaori NurfadillahNo ratings yet
- Drug Study FormatDocument16 pagesDrug Study FormatFranchieNo ratings yet
- Fluid and ElectrolytesDocument20 pagesFluid and ElectrolytesWyn Agustin100% (1)
- Course in The WardDocument12 pagesCourse in The Wardmikhaela sencilNo ratings yet
- NCP Deficient Fluid Volume Related To Fluid Loss DHNDocument2 pagesNCP Deficient Fluid Volume Related To Fluid Loss DHNMa. Elaine Carla Tating38% (8)
- Fii and Electrolyte ManagemeDocument7 pagesFii and Electrolyte ManagemeAulia lestariNo ratings yet
- Jain 2015Document12 pagesJain 2015Carla CANo ratings yet
- Assessment of Dry Weight in Hemodialysis: An Overview: ReviewDocument12 pagesAssessment of Dry Weight in Hemodialysis: An Overview: ReviewAshleyNo ratings yet
- Como Calcular LiquidosDocument8 pagesComo Calcular Liquidoskaterinavila300No ratings yet
- Assessing Patient HydrationDocument5 pagesAssessing Patient HydrationDuvan F Triana ViviescasNo ratings yet
- Fluids and Electrolytes: An Easy and Intuitive Way to Understand and Memorize Fluids, Electrolytes, and Acidic-Base BalanceFrom EverandFluids and Electrolytes: An Easy and Intuitive Way to Understand and Memorize Fluids, Electrolytes, and Acidic-Base BalanceRating: 5 out of 5 stars5/5 (2)
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument3 pagesSan Francisco St. Butuan City 8600, Region XIII Caraga, Philippineskuro hanabusaNo ratings yet
- Fluids and Electrolytes Nursing Care Management and Study GuideDocument23 pagesFluids and Electrolytes Nursing Care Management and Study GuideFatima DajoyagNo ratings yet
- Fluid Deficit NCPDocument2 pagesFluid Deficit NCPjustinekaye diongsonNo ratings yet
- Oedema Causes, Physiology and Nursing Management - 2004Document7 pagesOedema Causes, Physiology and Nursing Management - 2004endang sriNo ratings yet
- Perioperative Fluids in ChildrenDocument7 pagesPerioperative Fluids in ChildrenRosallia MegawatiNo ratings yet
- General Principles of Fluid Therapy in Small Animal MedicineDocument11 pagesGeneral Principles of Fluid Therapy in Small Animal MedicineAna Laura Villanueva ArellanoNo ratings yet
- Fluids and ElectrolytesDocument142 pagesFluids and ElectrolytesAndradaLavricNo ratings yet
- Fluid Stewardship 1660380556Document9 pagesFluid Stewardship 1660380556Mohammed VHNo ratings yet
- High Acuity Fluid and Electrolytes Chapter 25Document19 pagesHigh Acuity Fluid and Electrolytes Chapter 25AANo ratings yet
- NCP Notes Acute GlomerulonephritisDocument3 pagesNCP Notes Acute GlomerulonephritisMargareth DandanNo ratings yet
- IV Fluids What Nurses Need To KnowDocument9 pagesIV Fluids What Nurses Need To KnowAlex ChicasNo ratings yet
- Assessment Nursing Diagnosis Inference Plan of Care Interventions Rationale EvaluationDocument3 pagesAssessment Nursing Diagnosis Inference Plan of Care Interventions Rationale EvaluationPatricia OrtegaNo ratings yet
- Facto NCPDocument3 pagesFacto NCPkkd nyleNo ratings yet
- Renal 3 - Regulation of Body Fluid Vol and Fluid OsmolarityDocument8 pagesRenal 3 - Regulation of Body Fluid Vol and Fluid OsmolarityManci Bito-onNo ratings yet
- NCP Lab ResultDocument5 pagesNCP Lab ResultJoy Mariel Isadora BurgosNo ratings yet
- Nutrients: Narrative Review of Hydration and Selected Health Outcomes in The General PopulationDocument29 pagesNutrients: Narrative Review of Hydration and Selected Health Outcomes in The General PopulationwachoNo ratings yet
- Fluid and ElectrolyteDocument19 pagesFluid and ElectrolyteahmedNo ratings yet
- Fluid and Hyponatremia Management: by Craig B. Whitman, Pharm.D., BCPS, BCCCPDocument16 pagesFluid and Hyponatremia Management: by Craig B. Whitman, Pharm.D., BCPS, BCCCPAleksandar Dimovski100% (1)
- Update Terapi Cairan Pada: Pasien Covid-19Document43 pagesUpdate Terapi Cairan Pada: Pasien Covid-19Alita Mei RosfyanitaNo ratings yet
- IV Fluids (What Nurses Need To Know)Document9 pagesIV Fluids (What Nurses Need To Know)ChelseaLovell100% (2)
- Perioperative Fluid Therapy For Major Surgery: Clinical Focus ReviewDocument8 pagesPerioperative Fluid Therapy For Major Surgery: Clinical Focus ReviewAbhishek LonikarNo ratings yet
- Blood & Body Fluid Tortora 15TH EditionDocument20 pagesBlood & Body Fluid Tortora 15TH Edition334scisyb2020rishabhsingalNo ratings yet
- NCP Drug Study 2, Ojoy Dan Joshua LDocument4 pagesNCP Drug Study 2, Ojoy Dan Joshua Ldan.ojoy18No ratings yet
- Chapter 15 Fluid and Chemical BalanceDocument47 pagesChapter 15 Fluid and Chemical BalanceIntan FirmallahNo ratings yet
- A Review of Hydration.6Document8 pagesA Review of Hydration.6Paulo TsunetaNo ratings yet
- PGDBC IDocument47 pagesPGDBC IDr Estari MamidalaNo ratings yet
- Fluid and ElectrolytesDocument10 pagesFluid and ElectrolytesYunisa IrenNo ratings yet
- Fluid and ElectrolytesDocument29 pagesFluid and ElectrolytesLinh Tra100% (1)
- Fluid Therapy in Cattle PDFDocument21 pagesFluid Therapy in Cattle PDFYuNo ratings yet
- Applied Physiology of Body Fluids in Dogs and CatsDocument24 pagesApplied Physiology of Body Fluids in Dogs and CatsJuan Carlos RuaNo ratings yet
- Name: Age/Sex: Medical Diagnosis: Nursing Diagnosis: Short Term Goal: Long Term GoalDocument5 pagesName: Age/Sex: Medical Diagnosis: Nursing Diagnosis: Short Term Goal: Long Term GoalThoLitz AguinaldoNo ratings yet
- Water As An Essential Nutrient The PhysiologyDocument10 pagesWater As An Essential Nutrient The PhysiologyGianinaMihalacheCojocaruNo ratings yet
- Chronic Renal Failure Nursing Care PlanDocument6 pagesChronic Renal Failure Nursing Care PlanRuva Oscass JimmyNo ratings yet
- Nursing Care Plan: Fluid VolumeDocument2 pagesNursing Care Plan: Fluid VolumeShazu kNo ratings yet
- Apothecary and Household Measurements and Metric ConversionsDocument2 pagesApothecary and Household Measurements and Metric ConversionsDennis GarrettNo ratings yet
- Ricafort, Maxine S. GRP 2H Nursing Care Plan Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesRicafort, Maxine S. GRP 2H Nursing Care Plan Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationMaxine RicafortNo ratings yet
- Fluids and ElectrolytesDocument9 pagesFluids and ElectrolytesAlvin Jay DacilloNo ratings yet
- Fluids ElectrolytesDocument17 pagesFluids ElectrolytesShing Mae MarieNo ratings yet
- 4F-A:: Fluid & Electrolytes Concept: Protein Which Is18%, We Have Fat Which 16%, The Mineral and Etc. Is 6%Document11 pages4F-A:: Fluid & Electrolytes Concept: Protein Which Is18%, We Have Fat Which 16%, The Mineral and Etc. Is 6%Alyssa Claire TumulakNo ratings yet
- 4 Body Fluid, Haemostasis, ApoptosisDocument68 pages4 Body Fluid, Haemostasis, Apoptosischochojk36No ratings yet
- I Know You Know: Integrating Traditional and Contemporary Healing Thinking and ApplicationFrom EverandI Know You Know: Integrating Traditional and Contemporary Healing Thinking and ApplicationNo ratings yet
- Thesis TemplateDocument14 pagesThesis TemplateDip Ayan MNo ratings yet
- Health System Delivery in BangladeshDocument50 pagesHealth System Delivery in BangladeshDip Ayan M100% (1)
- Communication & Colaboration in NursingDocument35 pagesCommunication & Colaboration in NursingDip Ayan MNo ratings yet
- Political Activism in Nursing Final PresentationDocument30 pagesPolitical Activism in Nursing Final PresentationDip Ayan MNo ratings yet
- Illness, Culture and Caring Impact On Patients, Families and NursesDocument18 pagesIllness, Culture and Caring Impact On Patients, Families and NursesDip Ayan MNo ratings yet
- Nursing Theory - The Basis For Professional NursingDocument66 pagesNursing Theory - The Basis For Professional NursingDip Ayan MNo ratings yet
- Presentation Profesionalism Dipali MamDocument20 pagesPresentation Profesionalism Dipali MamDip Ayan MNo ratings yet
- Critical Thinking, Nursing Process and Clinical JudgmentDocument25 pagesCritical Thinking, Nursing Process and Clinical JudgmentDip Ayan MNo ratings yet
- Infusion Quiz 3Document6 pagesInfusion Quiz 3Dip Ayan MNo ratings yet
- ASSIGNMENT Cover AfsanaDocument1 pageASSIGNMENT Cover AfsanaDip Ayan MNo ratings yet
- Assessment of Fluid and ElectrolyteDocument15 pagesAssessment of Fluid and ElectrolyteDip Ayan MNo ratings yet
- Partial CorrelationDocument2 pagesPartial CorrelationDip Ayan MNo ratings yet
- 01 Staff Nurse AIIMS Rishikesh Memory Based QuestionDocument2 pages01 Staff Nurse AIIMS Rishikesh Memory Based QuestionDip Ayan MNo ratings yet
- The Largest Organ of The Body IsDocument10 pagesThe Largest Organ of The Body IsDip Ayan MNo ratings yet
- S C R S C: Ymptom Lusters Elated To Pecific AncersDocument6 pagesS C R S C: Ymptom Lusters Elated To Pecific AncersDip Ayan MNo ratings yet
- Antimicrobial ResistanceDocument4 pagesAntimicrobial ResistanceDip Ayan MNo ratings yet
- Symptom ClusterDocument7 pagesSymptom ClusterDip Ayan MNo ratings yet
- Occupational StressDocument8 pagesOccupational StressDip Ayan MNo ratings yet
- Provincial Government of Oriental Mindoro Summary List of Office/G.O. Divisions Performance RatingsDocument3 pagesProvincial Government of Oriental Mindoro Summary List of Office/G.O. Divisions Performance RatingsZyreen Kate CataquisNo ratings yet
- Lab Work 1Document2 pagesLab Work 1Adly HakimNo ratings yet
- WELDING Book AWSD1.1 Rev-3ADocument35 pagesWELDING Book AWSD1.1 Rev-3AFerdie OS100% (1)
- McKinsey Survey-Managing SustainabilityDocument10 pagesMcKinsey Survey-Managing SustainabilityAminur RahamanNo ratings yet
- L 0606279Document179 pagesL 0606279Jeff ImmerNo ratings yet
- Terraria Official Lore PDFDocument3 pagesTerraria Official Lore PDFCavalo SebosoNo ratings yet
- WVA Consulting Engineers PVT LTD: Analsyis and Design of Steel Watch TowerDocument23 pagesWVA Consulting Engineers PVT LTD: Analsyis and Design of Steel Watch TowerRomyMohanNo ratings yet
- Group 3 CW - Role of NGOs in Socio EconomicDocument9 pagesGroup 3 CW - Role of NGOs in Socio EconomicKisyenene JamusiNo ratings yet
- 74 20 03Document6 pages74 20 03vanmorrison69No ratings yet
- Corporate Nvidia in BriefDocument2 pagesCorporate Nvidia in BriefakesplwebsiteNo ratings yet
- FFS PINNSEF 30 November 2020Document1 pageFFS PINNSEF 30 November 2020teguhsunyotoNo ratings yet
- HX DG V 5.1.0 PDFDocument136 pagesHX DG V 5.1.0 PDFLyu SeyNo ratings yet
- English8 q1 Mod4of5 Cohesivedevices v2Document19 pagesEnglish8 q1 Mod4of5 Cohesivedevices v2shania puppyNo ratings yet
- Cartilla Didactica de Negocios y ContabilidadDocument118 pagesCartilla Didactica de Negocios y ContabilidadJesus Angel SalvadorNo ratings yet
- Talent AcquisitionDocument2 pagesTalent AcquisitionkiranNo ratings yet
- Bosch Solar Cell M 3BB EnglischDocument2 pagesBosch Solar Cell M 3BB EnglischAlberto AbsantNo ratings yet
- Enron ScandalDocument2 pagesEnron ScandalKoko LaineNo ratings yet
- Building Construction and Materials Report: Curtain Wall Building Type Building Name: Seagrams BuildingDocument6 pagesBuilding Construction and Materials Report: Curtain Wall Building Type Building Name: Seagrams BuildingAyushi AroraNo ratings yet
- Congential 3 Musculoskeletal 3 Neurological 3 Abusive DisordersDocument7 pagesCongential 3 Musculoskeletal 3 Neurological 3 Abusive DisordersNichole CollinsNo ratings yet
- Common Size Statement Analysis PDF Notes 1Document10 pagesCommon Size Statement Analysis PDF Notes 124.7upskill Lakshmi V0% (1)
- Final Sample Report of Maruti Car CompanyDocument69 pagesFinal Sample Report of Maruti Car Companyofficial vrNo ratings yet
- Multiple Choice QuestionsDocument6 pagesMultiple Choice QuestionsJamie DayagbilNo ratings yet
- Advanced Digital Controls Improve PFC PerformanceDocument18 pagesAdvanced Digital Controls Improve PFC Performancediablo diablolordNo ratings yet
- Neverwhere by Neil Gaiman - Teacher Study GuideDocument3 pagesNeverwhere by Neil Gaiman - Teacher Study GuideHarperAcademic33% (3)
- Chargesheet For ProjectDocument4 pagesChargesheet For ProjectSom Dutt VyasNo ratings yet
- Final INTERNSHIP Report-AshishDocument66 pagesFinal INTERNSHIP Report-AshishAshish PantNo ratings yet
- Piyumal PereraDocument1 pagePiyumal Pererays7mjwyqhsNo ratings yet
- The 73rd Constitutional Amendment ActDocument26 pagesThe 73rd Constitutional Amendment ActYasser ArfatNo ratings yet