Download as pdf or txt
You might also like
- Grammar Tales Teaching GuideDocument124 pagesGrammar Tales Teaching GuideEdilberto Uribe98% (49)
- IntelliVue Information Center HL7 Programmer S Guide PDFDocument210 pagesIntelliVue Information Center HL7 Programmer S Guide PDFhugutuxNo ratings yet
- What Is ResearchDocument12 pagesWhat Is ResearchAdrian Verzo Santo100% (2)
- Global Public Health: Click To Edit Master Title StyleDocument77 pagesGlobal Public Health: Click To Edit Master Title StyleDono WidiatmokoNo ratings yet
- Bioplan Nieto Nahum)Document6 pagesBioplan Nieto Nahum)Claudia Morales UlloaNo ratings yet
- Biodose Models:Nsd, Cre, TDF, LQ& Their Limitations: Moderator: Mr. Ranjit Singh Presented By: Navneet KaurDocument54 pagesBiodose Models:Nsd, Cre, TDF, LQ& Their Limitations: Moderator: Mr. Ranjit Singh Presented By: Navneet KaurSAlonii ChawlaNo ratings yet
- Dose Cluster Model Parameterization of The Parotid Gland in Irradiation of Head and Neck CancerDocument11 pagesDose Cluster Model Parameterization of The Parotid Gland in Irradiation of Head and Neck CancerAlfian AfriansyahNo ratings yet
- Alber 1999Document16 pagesAlber 1999reginafalancaNo ratings yet
- A Raghu Sepsis1Document9 pagesA Raghu Sepsis1Stabak NandiNo ratings yet
- A Raghu Sepsis1Document9 pagesA Raghu Sepsis1Stabak NandiNo ratings yet
- 7 Vol.121 Jan.2021 pp.76-89Document15 pages7 Vol.121 Jan.2021 pp.76-89Terem TebautaNo ratings yet
- 04 v4n2 00057Document13 pages04 v4n2 00057Mauricio Moyano CastilloNo ratings yet
- Internal Dosimetry As A Tool For Radiation Protection of The Patient in Nuclear MedicineDocument11 pagesInternal Dosimetry As A Tool For Radiation Protection of The Patient in Nuclear MedicinesantoshaiimsNo ratings yet
- Research Paper - Econometrics - DiD Event StudiesDocument9 pagesResearch Paper - Econometrics - DiD Event StudiesCem DemirogluNo ratings yet
- Risk Evaluation in Failure Mode and Effects Analysis Based On D Numbers TheoryDocument20 pagesRisk Evaluation in Failure Mode and Effects Analysis Based On D Numbers TheoryasiyahNo ratings yet
- Chapter1 Handout 2023 24Document56 pagesChapter1 Handout 2023 24dophuctoan216No ratings yet
- Statistical Rule of ThumbDocument14 pagesStatistical Rule of Thumbitung23No ratings yet
- Aritificial Intlligence PaperDocument15 pagesAritificial Intlligence PaperHaritaNo ratings yet
- Goodness of Fit and Related Inference Processes For Quantile RegressionDocument16 pagesGoodness of Fit and Related Inference Processes For Quantile RegressionAndersonMonteiroNo ratings yet
- A Multiphase Direct Aperture Optimization For Inverse Planning in RadiotherapyDocument6 pagesA Multiphase Direct Aperture Optimization For Inverse Planning in RadiotherapyMauricio Moyano CastilloNo ratings yet
- Are Dose Calculations During Dose Optimization in Brachytherapy Necessary ?Document15 pagesAre Dose Calculations During Dose Optimization in Brachytherapy Necessary ?mlahanas2No ratings yet
- Project Report Group 9 CC01Document14 pagesProject Report Group 9 CC01caogiatri122004No ratings yet
- Bed Practica RTDocument11 pagesBed Practica RTandresNo ratings yet
- Estimation of Public Compliance With COVID-19 Prevention Standard Operating Procedures Through A Mathematical ModelDocument10 pagesEstimation of Public Compliance With COVID-19 Prevention Standard Operating Procedures Through A Mathematical ModelNORAZALIZA BINTI MOHD JAMILNo ratings yet
- Precise Determination of The Branching Ratio of The Neutral-Pion Dalitz DecayDocument6 pagesPrecise Determination of The Branching Ratio of The Neutral-Pion Dalitz DecayPepe LuisNo ratings yet
- Homework2 AnswerDocument6 pagesHomework2 AnswerDennisParekhNo ratings yet
- MiteshDocument12 pagesMiteshJayanti SahooNo ratings yet
- On The Accuracy and Effectiveness of Dose Reconstruction For TomotherapyDocument25 pagesOn The Accuracy and Effectiveness of Dose Reconstruction For TomotherapyenriquefisicoNo ratings yet
- Identification of Metabolomic Biomarker Using Multiple Statistical Techniques and Recursive Feature EliminationDocument4 pagesIdentification of Metabolomic Biomarker Using Multiple Statistical Techniques and Recursive Feature EliminationKawshik BanerjeeNo ratings yet
- Comparison of Topogram-Based Body Size Indices For CT Dose Consideration and Scan Protocol OptimizationDocument10 pagesComparison of Topogram-Based Body Size Indices For CT Dose Consideration and Scan Protocol OptimizationBen LiNo ratings yet
- Orton - Quantitative RadiobiologyDocument32 pagesOrton - Quantitative RadiobiologydptofisicaflorestaNo ratings yet
- Metrics Jan 2021Document10 pagesMetrics Jan 2021Ahmed leoNo ratings yet
- AudpcDocument9 pagesAudpcVina Enggi WidiyaniNo ratings yet
- Covid 19 Lastversion PDFDocument11 pagesCovid 19 Lastversion PDFRafael AngaritaNo ratings yet
- Homework 3Document3 pagesHomework 3Cloud worldNo ratings yet
- Individual Dosimetry System For Targeted Alpha TheDocument8 pagesIndividual Dosimetry System For Targeted Alpha TheMauricio García CamachoNo ratings yet
- A Mixed-Eects Multinomial Logistic Regression Model: Donald HedekerDocument14 pagesA Mixed-Eects Multinomial Logistic Regression Model: Donald Hedekerluisa fernandaNo ratings yet
- Estimation and Inference of Extremal Quantile Treatment Effects For Heavy-Tailed DistributionsDocument12 pagesEstimation and Inference of Extremal Quantile Treatment Effects For Heavy-Tailed Distributionsshuyingyuan1998No ratings yet
- FR 1 PDFDocument11 pagesFR 1 PDFFrederico GomesNo ratings yet
- Skin FlashDocument1 pageSkin Flashman gobinda chowdhuryNo ratings yet
- ICRU 38 Interstitial ReportingDocument42 pagesICRU 38 Interstitial ReportingLaura MDNo ratings yet
- 8 Fenwick2012Document10 pages8 Fenwick2012RivssNo ratings yet
- Fast Multiple Optimizations Of2 Quadratic Dose Objective Functions in IMRTDocument12 pagesFast Multiple Optimizations Of2 Quadratic Dose Objective Functions in IMRTMauricio Moyano CastilloNo ratings yet
- Why Experiment?Document15 pagesWhy Experiment?Praween NishadNo ratings yet
- MIT6 003S10 Assn01Document6 pagesMIT6 003S10 Assn01thomagtNo ratings yet
- CH 35 Statistical TreatmentDocument28 pagesCH 35 Statistical Treatmentmebajar05No ratings yet
- 2012 Enhancement of Object Detection With Transcranial Direct Current Stimulation Is Associated With Increased AttentionDocument8 pages2012 Enhancement of Object Detection With Transcranial Direct Current Stimulation Is Associated With Increased AttentionAlex KwanNo ratings yet
- Foods 04 00565Document16 pagesFoods 04 00565Md. Habibur Rahman Bejoy Khan ,155408No ratings yet
- Mitesh Kumar JenaDocument12 pagesMitesh Kumar JenaJayanti SahooNo ratings yet
- Unit 5 DefinitionsDocument8 pagesUnit 5 DefinitionslokeshnathNo ratings yet
- Problema Ecuaciones DiferencialesDocument2 pagesProblema Ecuaciones DiferencialesJUAN ESTEBAN ZULUAGA PAREDESNo ratings yet
- 1 s2.0 S0096300318310130 MainDocument11 pages1 s2.0 S0096300318310130 MainIntan PermataNo ratings yet
- Local Search Algorithm Direct Aperture OptimizationDocument6 pagesLocal Search Algorithm Direct Aperture OptimizationMauricio Moyano CastilloNo ratings yet
- Current and Future Accelerator Technologies For Charged Particle TherapyDocument38 pagesCurrent and Future Accelerator Technologies For Charged Particle TherapyHashir SaeedNo ratings yet
- The Power Normal DistributionDocument7 pagesThe Power Normal DistributionMuhammad SatriyoNo ratings yet
- Anon2021 Approximate Birkhoff-von-Neumann Decomposition A Differentiable ApproachDocument15 pagesAnon2021 Approximate Birkhoff-von-Neumann Decomposition A Differentiable Approachhans wurstNo ratings yet
- Estimating Long Run Effects in Models With Cross-Sectional Dependence Using Xtdcce2Document37 pagesEstimating Long Run Effects in Models With Cross-Sectional Dependence Using Xtdcce2fbn2377No ratings yet
- Radiation OncDocument15 pagesRadiation OncMihreta MustaficNo ratings yet
- Artigo - Extremity Exposure in Nuc MedDocument6 pagesArtigo - Extremity Exposure in Nuc MedsamuelNo ratings yet
- 3-Monitoring Drug Concentration in Emergency Medicine PDFDocument10 pages3-Monitoring Drug Concentration in Emergency Medicine PDFMaav.325No ratings yet
- 2015-红皮-LET Painting Beam NumberDocument8 pages2015-红皮-LET Painting Beam Numberbo zhaoNo ratings yet
- Multi ChannelDocument57 pagesMulti Channelbasavaraj hagaratagiNo ratings yet
- v1 CoveredDocument10 pagesv1 CoveredSAbir KhanNo ratings yet
- Neuroscientific based therapy of dysfunctional cognitive overgeneralizations caused by stimulus overload with an "emotionSync" methodFrom EverandNeuroscientific based therapy of dysfunctional cognitive overgeneralizations caused by stimulus overload with an "emotionSync" methodNo ratings yet
- A Comparison of Shielding Calculation Methods For Multi-Slice Computed Tomography (CT) SystemsDocument15 pagesA Comparison of Shielding Calculation Methods For Multi-Slice Computed Tomography (CT) SystemsSamu SimamesaNo ratings yet
- Spek Pheno and Confidence SG E-KatDocument3 pagesSpek Pheno and Confidence SG E-KatSamu SimamesaNo ratings yet
- Shielding Calculation For Nuclear Medicine ServiceDocument10 pagesShielding Calculation For Nuclear Medicine ServiceSamu SimamesaNo ratings yet
- Eye Lens Dose During CT ExamDocument7 pagesEye Lens Dose During CT ExamSamu SimamesaNo ratings yet
- Radiation Shielding Design For Medical Cyclotron: January 2013Document4 pagesRadiation Shielding Design For Medical Cyclotron: January 2013Samu SimamesaNo ratings yet
- Daily QA Report Somatom Go AllDocument17 pagesDaily QA Report Somatom Go AllSamu SimamesaNo ratings yet
- No. 1 CT-Scan 64 Slice SOMATOM Go - AllDocument2 pagesNo. 1 CT-Scan 64 Slice SOMATOM Go - AllSamu SimamesaNo ratings yet
- Neutron InteractionDocument47 pagesNeutron InteractionSamu SimamesaNo ratings yet
- Zosi Wireless NVR & Monitor SystemDocument60 pagesZosi Wireless NVR & Monitor SystemJose RamirezNo ratings yet
- Ac Recovery Machine User Manual PDFDocument39 pagesAc Recovery Machine User Manual PDFmybdt1691No ratings yet
- Telephone EnglishDocument5 pagesTelephone EnglishZaw WinOoNo ratings yet
- Alliance Portfolios and Shareholder Value in post-IPO Firms The Moderating Roles of Portfolio Structure and Firm-Level UncertaintyDocument17 pagesAlliance Portfolios and Shareholder Value in post-IPO Firms The Moderating Roles of Portfolio Structure and Firm-Level Uncertaintygogayin869No ratings yet
- 500kV Aluminum Welded Bus Pipe Terminal PDFDocument9 pages500kV Aluminum Welded Bus Pipe Terminal PDFMohakumar MaranNo ratings yet
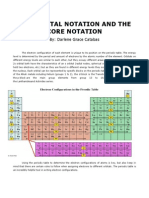
- Catabas Darlene - Orbital Core NotationDocument9 pagesCatabas Darlene - Orbital Core Notationapi-233267698No ratings yet
- Lab Manual Load - Test - On - DC - Shunt - Motor PDFDocument8 pagesLab Manual Load - Test - On - DC - Shunt - Motor PDFfongNo ratings yet
- AP 5902 Liability Supporting NotesDocument6 pagesAP 5902 Liability Supporting NotesMeojh Imissu100% (1)
- Miscellaneous Measurements: and ControlsDocument50 pagesMiscellaneous Measurements: and ControlsJeje JungNo ratings yet
- JES Command OverviewDocument74 pagesJES Command Overviewdb manishNo ratings yet
- Dark Energy and Dark MatterDocument26 pagesDark Energy and Dark MattersaphirehaelNo ratings yet
- CURVESDocument30 pagesCURVESPHULARAM PEGUNo ratings yet
- Selection of Materials For WeldingDocument1 pageSelection of Materials For WeldingIshwarNo ratings yet
- AphishmDocument1 pageAphishmAmit RajputNo ratings yet
- EN Quick Reference Guide Fabian HFOi-V4.0Document30 pagesEN Quick Reference Guide Fabian HFOi-V4.0Tanzimul IslamNo ratings yet
- Syllabusbtechec1 PDFDocument107 pagesSyllabusbtechec1 PDFAmol AmollNo ratings yet
- Safety Alert 365 Bsee Identified Grating and Open Hole Hazards During Risk Based InspectionsDocument3 pagesSafety Alert 365 Bsee Identified Grating and Open Hole Hazards During Risk Based Inspectionsi.kamalNo ratings yet
- Credit RatingDocument15 pagesCredit RatingManisha SinghNo ratings yet
- Bridgeport Series I ManualDocument134 pagesBridgeport Series I ManualMANUEL VICTOR100% (1)
- Camera ConfidenceDocument13 pagesCamera ConfidenceCont ReadNo ratings yet
- LinkBelt 108H5Document20 pagesLinkBelt 108H5amirNo ratings yet
- Daughtrey v. Fresno City Police Department, Et Al. - Document No. 4Document1 pageDaughtrey v. Fresno City Police Department, Et Al. - Document No. 4Justia.comNo ratings yet
- Plaintiffs' Motion For Entry of JudgmentDocument14 pagesPlaintiffs' Motion For Entry of JudgmentBen SheffnerNo ratings yet
- Aa - Moneyback20 - 29-10-2023 8.59.34Document6 pagesAa - Moneyback20 - 29-10-2023 8.59.34do.yogeshaNo ratings yet
- Create Request For QuotationDocument18 pagesCreate Request For QuotationAdauto PolizeliNo ratings yet
- EQ 5D 5L Index Value Calculator V1.1Document146 pagesEQ 5D 5L Index Value Calculator V1.1mmmaw mmNo ratings yet