Download as docx, pdf, or txt
You might also like
- Endodontic SealersDocument138 pagesEndodontic SealersGayathri100% (2)
- Continuum Spinal Cord AnatomyDocument25 pagesContinuum Spinal Cord AnatomyslojnotakNo ratings yet
- Thespinalcord: A Review of Functional NeuroanatomyDocument18 pagesThespinalcord: A Review of Functional NeuroanatomyasfwegereNo ratings yet
- #Anatomy of The Spinal CordDocument15 pages#Anatomy of The Spinal CordMaryamNo ratings yet
- Spinal Cord: StructureDocument5 pagesSpinal Cord: StructureIka LestariNo ratings yet
- Anatomy and Localization of Spinal Cord DisordersDocument23 pagesAnatomy and Localization of Spinal Cord DisordersMichael RojasNo ratings yet
- Lab 17 The Spinal Cord Somatic NervesDocument18 pagesLab 17 The Spinal Cord Somatic Nervesrhycelayon304No ratings yet
- Anatomy and Physiology of The Spine: Google ImagesDocument9 pagesAnatomy and Physiology of The Spine: Google Imagesraquel maniegoNo ratings yet
- Spinal CordDocument9 pagesSpinal Cordpromisearinzechi4No ratings yet
- 1 - Spinal Cord NotesDocument7 pages1 - Spinal Cord NotesOceanChan QdNo ratings yet
- Katya Anaphysio NewDocument6 pagesKatya Anaphysio NewKriska Herrero TumamakNo ratings yet
- Anatomy SpineDocument6 pagesAnatomy SpineKris AdiNo ratings yet
- Saraf Spinal: Neuroanatomy, Somatic Nervous SystemDocument10 pagesSaraf Spinal: Neuroanatomy, Somatic Nervous SystemFitri SukmawatiNo ratings yet
- Chapter 3: Anatomy of The Spinal Cord: Skip To Main Contentskip To Navigation (Accesskey N)Document12 pagesChapter 3: Anatomy of The Spinal Cord: Skip To Main Contentskip To Navigation (Accesskey N)SN WijesinheNo ratings yet
- Anatomia Si Localizare in Boli SpinaleDocument8 pagesAnatomia Si Localizare in Boli SpinaleHalit DianaNo ratings yet
- Neuroanatomy, Cerebellum: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2023 JanDocument5 pagesNeuroanatomy, Cerebellum: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2023 JanANISA RIFKA RIDHONo ratings yet
- Anatomy of The Spinal CordDocument13 pagesAnatomy of The Spinal CordMumba MatthewsNo ratings yet
- Central Nervous System: DR Muhammad Ressam NazirDocument28 pagesCentral Nervous System: DR Muhammad Ressam NazirRessam NazirNo ratings yet
- International Standards For Neurological and Functional Classification of Spinal Cord InjuryDocument14 pagesInternational Standards For Neurological and Functional Classification of Spinal Cord InjuryVijay IyerNo ratings yet
- Spine Structure and FunctionDocument19 pagesSpine Structure and Functionakhil dattaNo ratings yet
- Blood Supply of Spinal Cord... 2022Document31 pagesBlood Supply of Spinal Cord... 2022David Pinto SilvaNo ratings yet
- Biomechanics of NervesDocument65 pagesBiomechanics of NervesZinneRah RahManNo ratings yet
- Biomechanics of Peripheral and Spinal Nerve RootsDocument86 pagesBiomechanics of Peripheral and Spinal Nerve RootsJawad HassanNo ratings yet
- Essentials of Regional Anesthesia Anatomy NYSORA - The New York School of Regional AnesthesiaDocument31 pagesEssentials of Regional Anesthesia Anatomy NYSORA - The New York School of Regional Anesthesiajorge ceballos troncosoNo ratings yet
- Iv. The Spinal Cord: Cordotomy Lumbar PunctureDocument0 pagesIv. The Spinal Cord: Cordotomy Lumbar PunctureAnonymous t5TDwdNo ratings yet
- Gardner 1948Document14 pagesGardner 1948mitroisergiuNo ratings yet
- Nerves of Upper LimbDocument9 pagesNerves of Upper LimbRaymond PosumaNo ratings yet
- Anatomy of The Spinal Cord: Dr. Eyad M. HusseinDocument41 pagesAnatomy of The Spinal Cord: Dr. Eyad M. Husseinأمال داود100% (1)
- Bio Mechanics of Nerve 03Document72 pagesBio Mechanics of Nerve 03deepuphysioNo ratings yet
- ЦНС - 2019Document50 pagesЦНС - 2019bekafop813No ratings yet
- Cabatbat, Sable A. BSN Iv - D: Brain MusclesDocument4 pagesCabatbat, Sable A. BSN Iv - D: Brain MusclesOdyNo ratings yet
- Spinal Cord AnatomyDocument34 pagesSpinal Cord AnatomyYana CatherineNo ratings yet
- 03-Spinal Cord Phys & AnatDocument9 pages03-Spinal Cord Phys & AnatAzwar Arsyad S SiNo ratings yet
- Spinal CordDocument59 pagesSpinal Cordveegeer100% (1)
- Spinal CordDocument4 pagesSpinal CordMabel LynNo ratings yet
- Neuroanatomy Notes 2010Document33 pagesNeuroanatomy Notes 2010Jennifer David InauenNo ratings yet
- Anatomy and Physiology For Bacterial MeningitisDocument4 pagesAnatomy and Physiology For Bacterial MeningitisynecesityNo ratings yet
- Neuroanatomy 1Document65 pagesNeuroanatomy 1maNo ratings yet
- Spinal CordDocument6 pagesSpinal Cordsangesh kNo ratings yet
- 1.wall of ThoraxDocument14 pages1.wall of ThoraxChandru ANo ratings yet
- Spinal Cord, Ascending PathwayDocument52 pagesSpinal Cord, Ascending PathwayKolawole Adesina KehindeNo ratings yet
- Neuroanatomy, Cerebellar Dysfunction: Gross AnatomyDocument5 pagesNeuroanatomy, Cerebellar Dysfunction: Gross AnatomyANISA RIFKA RIDHONo ratings yet
- Spinal Cord: Achmad AminuddinDocument29 pagesSpinal Cord: Achmad AminuddinSurajul AudaNo ratings yet
- Overview of Spinal NervesDocument12 pagesOverview of Spinal NervesGrace VersoniNo ratings yet
- Structures of The Spinal CanalDocument7 pagesStructures of The Spinal CanalveronicalovirgenNo ratings yet
- CGM 102 PPT 6Document21 pagesCGM 102 PPT 6Siddharth SharmaNo ratings yet
- Ни Т.Ю. spinal nervesDocument47 pagesНи Т.Ю. spinal nervesNur IffahNo ratings yet
- ue 1-Broc s Are ʹ an area of the frontal lobe, usually in the left hemisphere, that directs the muscle movements involvedDocument31 pagesue 1-Broc s Are ʹ an area of the frontal lobe, usually in the left hemisphere, that directs the muscle movements involvedMhmd IrakyNo ratings yet
- AD 5 Vertebral AnatomyDocument37 pagesAD 5 Vertebral AnatomyLintang ZerlinaNo ratings yet
- Spinalcord and It's Connections Neuro Anatomy - 2Document30 pagesSpinalcord and It's Connections Neuro Anatomy - 2Jamaru NishaNo ratings yet
- Anatomy Lec 13Document11 pagesAnatomy Lec 13Sajad H. HassanNo ratings yet
- Anatomy of The Spinal CordDocument68 pagesAnatomy of The Spinal Cordgloria anyebeNo ratings yet
- The Spinal Cord - FunctionsDocument11 pagesThe Spinal Cord - FunctionsMurali SgNo ratings yet
- Spinal CordDocument27 pagesSpinal Cordsiddharth.roy26587No ratings yet
- 03 Human Anatomy 1st YearDocument9 pages03 Human Anatomy 1st Yearit's EimyNo ratings yet
- 1 My Trigeminal NerveDocument23 pages1 My Trigeminal NerveDan 04No ratings yet
- The Spinal Cord: Lec-11-Dr - Maysoon AlkazzazDocument12 pagesThe Spinal Cord: Lec-11-Dr - Maysoon AlkazzazRose ParisNo ratings yet
- Thoracic and Coracoid Arteries In Two Families of Birds, Columbidae and HirundinidaeFrom EverandThoracic and Coracoid Arteries In Two Families of Birds, Columbidae and HirundinidaeNo ratings yet
- Maternal and Child Nursing: ST TH ST ND THDocument15 pagesMaternal and Child Nursing: ST TH ST ND THKatrina CaveNo ratings yet
- (Zerrudo) OB Refresher NotesDocument13 pages(Zerrudo) OB Refresher NotesKatrina CaveNo ratings yet
- Jestian Ryll B Delacruz Bsn-IvDocument3 pagesJestian Ryll B Delacruz Bsn-IvKatrina CaveNo ratings yet
- Reaction Paper (Self-Awareness)Document2 pagesReaction Paper (Self-Awareness)Katrina CaveNo ratings yet
- TH THDocument19 pagesTH THKatrina CaveNo ratings yet
- Img - 0200 3Document10 pagesImg - 0200 3Katrina CaveNo ratings yet
- 2 Scrub 1 CircuDocument3 pages2 Scrub 1 CircuKatrina CaveNo ratings yet
- Entrepreneurship ExamsDocument15 pagesEntrepreneurship ExamsKatrina CaveNo ratings yet
- Entrep Act - QuizzesDocument22 pagesEntrep Act - QuizzesKatrina CaveNo ratings yet
- Print Ko BukasDocument3 pagesPrint Ko BukasKatrina CaveNo ratings yet
- Proposed Strategies To Enhance The Self-Esteem of The Student NursesDocument10 pagesProposed Strategies To Enhance The Self-Esteem of The Student NursesKatrina CaveNo ratings yet
- 1 Scrub 2 CircuDocument2 pages1 Scrub 2 CircuKatrina CaveNo ratings yet
- A. Malpractice, Negligence, Torts and CrimesDocument7 pagesA. Malpractice, Negligence, Torts and CrimesKatrina CaveNo ratings yet
- Control of Diarrheal Diseases (CDD) : ObjectivesDocument39 pagesControl of Diarrheal Diseases (CDD) : ObjectivesKatrina CaveNo ratings yet
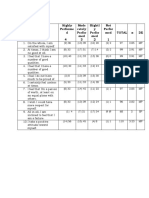
- Highly Performe D 4 Mode Rately Perfor Med 3 Slightl y Perfor Med 2 Not Perfor Med 1 Total X DEDocument4 pagesHighly Performe D 4 Mode Rately Perfor Med 3 Slightl y Perfor Med 2 Not Perfor Med 1 Total X DEKatrina CaveNo ratings yet
- Hiatal Hernia: No SymptomsDocument2 pagesHiatal Hernia: No SymptomsKatrina CaveNo ratings yet
- Return Demo GuideDocument1 pageReturn Demo GuideKatrina CaveNo ratings yet
- References AnalyzationDocument4 pagesReferences AnalyzationKatrina CaveNo ratings yet
- Jerome RepatoDocument4 pagesJerome RepatoKatrina CaveNo ratings yet
- Research SELF ESTEEM Grp4. 2Document47 pagesResearch SELF ESTEEM Grp4. 2Katrina Cave100% (2)
- Galperin - Stage-by-Stage Formation As A Method of Psychological InvestigationDocument21 pagesGalperin - Stage-by-Stage Formation As A Method of Psychological InvestigationPamela CNo ratings yet
- Organization and Evolution of The Nuclear Genome: Princess Lorraine Garcia Bs-Biology IvDocument25 pagesOrganization and Evolution of The Nuclear Genome: Princess Lorraine Garcia Bs-Biology IvLouella ArtatesNo ratings yet
- DLL ScienceDocument4 pagesDLL ScienceMark Adrian ArenasNo ratings yet
- Formulation and Evaluation of Nanoemulsion For Solubility Enhancement of KetoconazoleDocument14 pagesFormulation and Evaluation of Nanoemulsion For Solubility Enhancement of KetoconazoledgdNo ratings yet
- Lpe2501 Writing Portfolio Task 3 (Writing Form - Draft)Document4 pagesLpe2501 Writing Portfolio Task 3 (Writing Form - Draft)amin badrulNo ratings yet
- Extraction Procedure PDFDocument7 pagesExtraction Procedure PDFanushaNo ratings yet
- Sem PDFDocument20 pagesSem PDFSher AbbasNo ratings yet
- CH 13Document120 pagesCH 13mariamNo ratings yet
- NMAT BiologyDocument6 pagesNMAT BiologyJyl Yan SelasorNo ratings yet
- 2018 Trial 1 Biology Questions and Marking SchemeDocument11 pages2018 Trial 1 Biology Questions and Marking SchemeKodhekNo ratings yet
- Diabetic Gastropathy Gastric Neuromuscular Dysfunction in Diabetes Mellitus A Review of Symptoms, Pathophysiology, and TreatmentDocument15 pagesDiabetic Gastropathy Gastric Neuromuscular Dysfunction in Diabetes Mellitus A Review of Symptoms, Pathophysiology, and Treatmentrizkiya novitaNo ratings yet
- NaturalselectionprotocolDocument10 pagesNaturalselectionprotocolapi-319172404No ratings yet
- Ceramics For Medical ApplicationsDocument12 pagesCeramics For Medical ApplicationsEric KirschnerNo ratings yet
- Animal and Plant CellDocument30 pagesAnimal and Plant CellNetty BontuyanNo ratings yet
- Nstructions: Part 1: Short ConversationsDocument8 pagesNstructions: Part 1: Short ConversationsDenise Pelekouda-OikonomouNo ratings yet
- A Study On The Diversity and Abundance of Spiders in Arakulam VillageDocument5 pagesA Study On The Diversity and Abundance of Spiders in Arakulam Villagefebi chackoNo ratings yet
- BBOK407Document3 pagesBBOK407m7090899358No ratings yet
- The Brothers Flexner by Nancy Turner Banks MD MBADocument41 pagesThe Brothers Flexner by Nancy Turner Banks MD MBAOny997100% (1)
- C1 - An Introduction of Fermentation TechnologyDocument31 pagesC1 - An Introduction of Fermentation TechnologyThanh LiêmNo ratings yet
- Soft Computing (SC) Topper SolutionDocument35 pagesSoft Computing (SC) Topper Solutionakash100% (2)
- Sci Sumative ReviewerDocument4 pagesSci Sumative ReviewerGianni Micha E. AnsaldoNo ratings yet
- Determination of HemolysisDocument3 pagesDetermination of Hemolysislindsay becudoNo ratings yet
- Histology & Function of Connective Tissue: June 2015Document8 pagesHistology & Function of Connective Tissue: June 2015Subha DeyNo ratings yet
- The Role of Enzymes in The Digestive SystemDocument2 pagesThe Role of Enzymes in The Digestive SystemJeanAnzurezNo ratings yet
- Chap 9 BiomoleculesDocument4 pagesChap 9 BiomoleculesJayesh RautNo ratings yet
- PFMDocument24 pagesPFMFreudensteinitzNo ratings yet
- Aqua Pour Deluxe (EN/FR)Document12 pagesAqua Pour Deluxe (EN/FR)Nikken, Inc.No ratings yet
- Manuscript - Editing The Genome of CropsDocument20 pagesManuscript - Editing The Genome of CropsNiharika DasNo ratings yet
- Bulletin 6376 PDFDocument2 pagesBulletin 6376 PDFSky ImranNo ratings yet